This week’s second In Focus continues the conversation on drug policies and trends, providing updates and insights into the current landscape of Medicare’s drug price negotiations.
The Centers for Medicare & Medicaid Services (CMS) recently released the negotiated prices for the first 10 Medicare Part D drugs under the Inflation Reduction Act’s (IRA’s) negotiation authority. CMS plans to add more drugs to the negotiation list, including 15 additional Part D drugs in 2027 and 15 more products from both Part D (pharmacy benefit drugs) and Part B (mostly physician administered drugs). In 2029 and later years, another 20 drugs from either Part B or Part D will be chosen.
Negotiated Prices for First 10 Drugs Leave Unanswered Questions
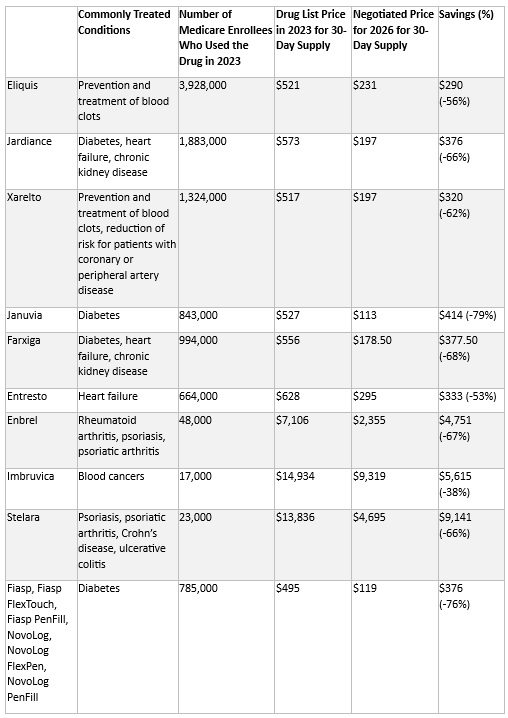
CMS estimates the negotiated prices for 30-day supplies of each medication will result in savings ranging from 38 percent to 79 percent compared with list prices when they take effect in 2026. This comparison, however, does not account for several factors that could affect the actual savings for the Medicare program and beneficiaries, including:
- Current negotiated discounts available to Medicare Part D plans
- Changes in tier placement for the negotiated drugs and their impact on patient cost sharing
- The exemption for manufacturers from the 10 percent discount during the initial coverage phase and the 20 percent discount thereafter once negotiated prices take effect in 2026
- The effect of Medicare’s negotiations on prices paid by other payers
- The impact of the IRA program on prices for other products and manufacturer investments in research and development of new products
CMS is required to provide a detailed explanation of how negotiated prices were determined by March 1. The price comparisons with privately negotiated prices, however, will remain unclear and the effects on other payers and longer-term investments in new products may not be fully understood for some time. The table below lists the negotiated discounts for the first 10 drugs, which CMS selected from the top 50 Part D drugs by spending, which lacked generic or biosimilar alternatives and met other IRA criteria.
Negotiated Drug Prices Applicable in 2026
Looking Ahead
Age of Products and Role of Generic and Biosimilar Competition: Drugs eligible for negotiation are typically the highest expenditure drugs that have been on the market for at least seven years or 11 years in the case of biologics. Importantly, products with generic or biosimilar competition are exempt from negotiation. This exemption may increase the speed at which biosimilar or generic competition comes to market, as the IRA requires competitors to engage in bona fide marketing to exempt an innovator from negotiation. Despite approval, biosimilars for some of the drugs will remain subject to negotiated prices until their marketing efforts begin.1
Impact on Medicaid and Other Payers: The IRA’s negotiated discounts are not required to be available outside of the Medicare program. It remains uncertain whether other payers will use Medicare-negotiated prices as leverage in their own negotiations. For Medicaid, the direct impact of negotiations themselves is expected to be negligible; however, the IRA’s inflation penalties could encourage more manufacturers to moderate price increases over time, potentially leading to reduced inflation penalty rebates to state Medicaid programs.
Connect with Us
To explore these topics further, join Health Management Associates at the upcoming event, Unlocking Solutions in Medicaid, Medicare, and Marketplace. Engage with our Medicare experts below who will lead a small group discussion on trends in prescription drug policies during the pre-conference workshop.
For details on IRA pricing issues or other Medicare health policy developments, contact our featured experts below. HMA’s Wakely Actuaries also are available to discuss the IRA’s role in Medicare Part D.


