This week, our second In Focus article addresses the transition to end the Medicare Advantage Value-Based Insurance Design (VBID) model, which launched in 2017 and subsequently has been expanded with bipartisan support. This model was designed to promote flexible benefit design, reduce cost barriers, and enhance care for targeted populations, especially dual eligibles and individuals with chronic conditions. In December 2024, however, the Centers for Medicare & Medicaid Services (CMS) announced that the model would be terminated by the end of 2025, citing unmitigable costs to the Medicare Trust Funds, totaling more than $4.5 billion across 2021 and 2022 alone.
Despite its popularity and effectiveness in improving medication adherence and addressing social determinants of health, CMS concluded that the cost trajectory was unsustainable within the parameters of the Innovation Center’s mandate.
The end of the VBID model is not the end of innovation in Medicare Advantage (MA); rather, it is a strategic inflection point. Plans that approach this transition with a proactive, data-driven lens will be best positioned to maintain competitive advantage, compliance, and member trust. This article reviews critical steps VBID plans should be taking and how Medicare Advantage Organizations (MAOs) and their partners can best prepare for future opportunities.
Pain Points and Key Strategic Decisions for MAOs
As plans prepare for a post-VBID world, they face a series of complex trade-offs—especially those with Dual Eligible Special Needs Plans (D-SNPs) that had $0 drug cost sharing under VBID. With the end of CMS’s drug cost offset in the initial coverage phase, MAOs will need to determine whether and how to absorb those costs through alternative mechanisms. In addition, plans will need to make important decisions regarding their other VBID benefits, namely, whether to discontinue or transition them to the special supplemental benefits for the chronically ill (SSBCI) program. MAOs should consider the following key strategic decisions:
- Offer an Enhanced Alternative (EA) or Basic Alternative (BA) Part D Plan: To replicate $0 cost sharing, MAOs would need to use EA or BA plan designs with $0 deductibles and $0 copays across all tiers—an expensive move and potentially untenable investment for many.
- Tier-Specific Buy-Downs (T1/T2): Some plans may consider buying down T1 and T2 copays to $0, a much less costly approach. Others may consider moving key T2 drugs to T1, while keeping T1 copays at $0 to protect access and using non-zero dollar T2 copays to limit costs.
- Competitive Alignment Considerations: MAOs offering broader cost-sharing reductions (e.g., $0 copays on both T1 and T2 drugs) may experience undesirable shifts in enrollment patterns depending on how competitors structure their formularies and benefit designs. MAOs should consider competitive parity and attempt to maintain a balanced benefit structure that aligns with market norms.
- Transferring VBID Benefits to SSBCI: Some benefits—like non-health-related transportation, healthy foods, and general supports for living—could migrate to the SSBCI program. But SSBCI has strict eligibility, documentation, and operational requirements, calling for nuanced workflows and cross-departmental coordination.
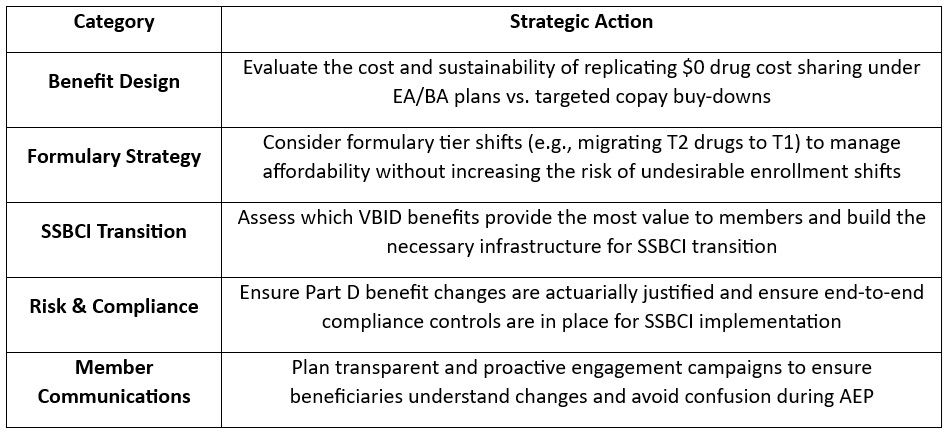
Action Plan: What MAOs Should Be Doing Now
To navigate this transition successfully, teams of experts at Wakely, a Health Management Associates, Inc. (HMA) Company, are already working with VBID stakeholders to evaluate multiple transition scenarios. Our experts recommend that MAOs take the following actions:
What to Watch: Future Innovation in Medicare Advantage
Though VBID is ending, the innovation landscape is far from static. With the new Trump Administration and the return of Abe Sutton—a VBID expansion advocate—appointed as Director of the CMS Innovation Center, our experts are closely monitoring the potential for a revised version of VBID or similar models. Stakeholder advocacy could influence how CMS prioritizes the next wave of innovation. Plans should consider engaging in dialogue now to shape what happens next.
Connect with Us
Wakely is embedded in MA strategy and policy. Wakely and HMA teams are working with clients to evaluate multiple transition scenarios, helping them optimize value, protect Star Ratings, and preserve member satisfaction during this pivotal shift, while also supporting targeted policy engagement efforts to ensure their perspectives are reflected in future CMS and Innovation Center decision making.
Our joint capabilities bring together:
- Actuarial modeling expertise to quantify cost and risk impacts of design alternatives
- Regulatory insight to ensure compliance with CMS requirements
- Operational support to help you implement SSBCI programs efficiently
- Market strategy consulting to align your plan offerings with local competition and enrollment goals
- Policy advocacy to help clients engage in the conversation around what comes next after VBID
To connect on additional questions contact our featured experts below.
