This week, our In Focus section reviews CMS’s proposed changes to the federal Medicaid managed care access, finance, and quality regulation (CMS-2439-P). A future In Focus will take a closer look at the proposed changes to the federal Medicaid access to care regulation (CMS-2442-P), which also has significant implications for state Medicaid programs.
On April 28, 2023, the Centers for Medicare & Medicaid Services (CMS) unveiled two significant and related proposed rules addressing Medicaid managed care access, finance, and quality requirements. Together these proposed rules signal a new era of accountability and transparency in the Medicaid program. They also strengthen beneficiaries’ role in influencing the policies and administration of state Medicaid programs.
Table 1 identifies a few of the key themes and issues addressed in the Medicaid managed care proposed rule. The deadline for submitting comments to CMS is July 3, 2023.
Table 1. Medicaid Managed Care Proposed Rule: Snapshot of Proposed Changes
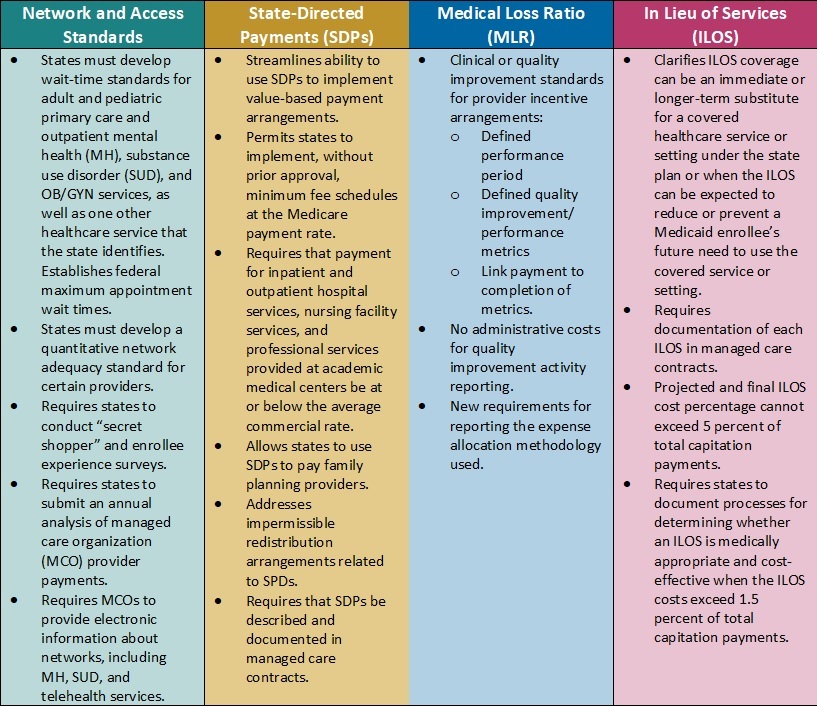
Key Themes and Considerations
Payment Ceilings May Accelerate Value-Based Payment Arrangements. Current federal regulations allow states to direct managed care organizations (MCOs) to pay providers according to specific rates or methods. States have used these directed payment arrangements to set minimum payment rates for certain types of providers or to require participation in value-based payment (VBP) initiatives.
In the proposed rule, CMS calls for establishing an upper limit for these payments. Specifically, the agency plans to limit the projected total payment rates to the average commercial rate (ACR) for inpatient and outpatient hospital services, nursing facility services, and qualified practitioner services at academic medical centers that states include in state-directed payment (SDP) arrangements. The ACR limit, in concert with the proposed SDP documentation and reporting, is among the most significant and complex proposed changes in the rule.
Considerations: The proposed changes represent a strong federal regulatory push to accelerate movement to VBP in Medicaid, which provides states with new levers to drive value in their Medicaid delivery systems. It also means that MCOs, providers, and other stakeholders will need to navigate and help inform the policies and contractual arrangements that will flow from the pending changes. For example, states may need to reflect on the following considerations:
- Whether the proposals will require them to reduce reimbursement
- Whether they will need to develop new value-based arrangements through SDPs and how these policies will be structured
- What outcomes they might need to prioritize
- How transparency in reporting provider-level payments could affect non-federal funding and SDP initiatives
Updated Approach to in Lieu of Services (ILOS) Facilitates Whole-Person Care. In January 2023, CMS issued a State Medicaid Director Letter (SMDL#23-001) advising states of the option to use the ILOS authority in Medicaid managed care programs to reduce healthcare inequities and address unmet health-related social needs (HRSNs), such as housing, food insecurity, and intimate partner violence. The proposed Medicaid managed care rule would expand upon and codify in regulation that guidance.
Considerations: Although the ILOS proposal adds reporting requirements and guardrails to address fiscal accountability, overall, the updated policy signals CMS’s willingness to support innovative state approaches to meet a continuum of beneficiary needs, including HRSNs that affect the social drivers of health. Notably, CMS advises that the substitution of an ILOS for a state plan service or setting should be cost-effective but does not need to be budget-neutral. States also can specify that an ILOS can be an immediate or longer-term substitute for a state plan service or setting.
States could pursue a variety of options under CMS’s revised ILOS framework. State Medicaid agencies and their partners can collaborate on ILOS strategies that will allow them to make further progress toward reducing healthcare inequities, as well as fulfill their quality strategy goals and objectives.
New Standards for Medical Loss Ratio Strengthen Link to Performance Improvement. Existing federal regulations require Medicaid managed care plans to report their medical loss ratio (MLR) to states annually, and, in turn, states must submit a summary of those reports to CMS. Many state MCO contracts require plans to comply with provider incentive and bonus policies; however, MCOs infrequently make incentive payments contingent on the provider meeting quantitative clinical or quality improvement standards.
Consistent with the healthcare sector’s transition toward value-based care, CMS proposes to strengthen the link between an MCOs incentive payment to a provider and the provider meeting defined quality improvement or performance metrics. Additionally, contractual language between MCOs and providers will need to more explicitly identify the dollar amounts tied to successful completion of these metrics. Only incentive payments based on quality improvement will be considered incurred claims when plans calculate their MLR; administrative costs cannot be included in quality improvement activity reporting.
Considerations. The proposed requirements are expected to add more transparency to negotiations between Medicaid MCOs and providers. MCOs will retain flexibility to determine the quality improvement or quantitative performance metrics, which carry more weight and accountability in CMS’s revised regulatory framework.
Network Adequacy Requirements Strengthen Link to Access and Rates. CMS also proposes policies that the agency believes will help strengthen Medicaid enrollees’ access to services. For example, the rule would require states to develop wait-time standards for adult and pediatric primary care and outpatient mental health, substance use disorder (SUD), and OB/GYN services, with CMS establishing federal minimum appointment wait times. States also will need to develop a quantitative network adequacy standard, beyond wait times, for certain providers.
Notably, CMS also plans to require states to submit an MCO-level analysis of MCO-to-provider payments. This analysis may provide more insights about the relationship between rates and access to certain types of providers and services. It may also improve alignment in access policies across delivery systems.
Considerations: States and MCOs should expect to need more sophisticated analysis of provider capacity at state and local market levels. This information will be critical in developing network adequacy standards and determining where additional provider support may be necessary. Expanded and new strategies may be needed to ensure compliance with the federal rules and resulting changes to state policies.
What’s Next
Many of CMS’s proposals track closely with many recent recommendations from federal commissions and oversight entities, including the Medicaid and CHIP Payment and Access Commission (MACPAC) and Government Accountability Office (GAO), which may indicate a greater likelihood that CMS will finalize those policies. If they are finalized largely as proposed, the rule will further the Biden Administration’s directional imprint on the Medicaid program.
Within the proposed rules described above, CMS identifies numerous areas where stakeholder input would be beneficial. States, MCOs, providers, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. Stakeholders also may use this time to begin planning for 2024 and determining what resources and tools they may need to prepare for implementation of the final regulations, as well as how their approach may vary based on state-specific factors.
For questions about the rule and how HMA’s team of experts can support your organization’s response, please contact our experts below.

