Weekly Roundup -
February 18, 2026
Smart. Strategic. Essential.
Unmatched Healthcare Insights from HMA,
Leavitt Partners & Wakely.
Featured:
Case Study Report: Lessons Learned from HealthySteps Technical Assistance in California
READ BRIEF

Trending: In Focus
Updates on Federal Funding for Rural Communities through the Rural Health Transformation Program
The Long View
On December 29, 2025, the Centers for Medicare & Medicaid Services (CMS) announced the highly anticipated funding awards to states for the Rural Health Transformation Program (RHTP)—a five-year, $50 billion federal initiative designed to stabilize and transform rural health systems across the country. This new federal investment marks a pivotal moment for states and their partners to address long-standing challenges in rural healthcare while laying the foundation for broader transformation. It provides an opportunity to reimagine care delivery, strengthen infrastructure, and build sustainable models that address entrenched gaps in rural health.
Directing Resources to Rural Communities
RHTP is designed with a focus on rural communities, where residents face persistent challenges such as provider shortages, hospital closures, and limited access to care. RHTP investments will support infrastructure development, IT system implementations and trainings, workforce recruitment and retention, and innovative care models tailored to rural community needs. The long-term goal is to create lasting capacity and resilience in rural health systems and promote better health outcomes for residents.
But the vision doesn’t stop there.
Catalyzing Statewide Transformation
While rural communities are the primary beneficiaries, we believe the impact of the RHTP will extend beyond rural borders. The program’s design encourages states to develop initiatives that can serve as pilots and start-ups, creating scalable solutions that can be adopted statewide. Workforce development programs, for example, may begin by focusing on rural providers and community health workers (CHWs) and training these individuals but, over time, strengthen the healthcare workforce across entire states and regions.
Much of the federal funding will enable states and their partners to invest in technology modernization, telehealth expansion, and integrated care models. These improvements assuredly will enhance access and quality for rural residents. And these same technologies can be deployed to enhance efficiency and coordination across entire health systems, laying the groundwork for broader system transformation and health improvement. The focus on chronic care management and innovative care arrangements has the potential to improve outcomes for all populations.
Collaborative Pathways for States and Partners
States and their partners—including health systems, community-based organizations, and technology innovators—have a valuable opportunity to collaborate on initiatives. In our review of state applications and the initial wave of state driven funding solicitations, we identified efforts to tackle long-standing system challenges, including:
- Data Sharing and Interoperability. States responded to the federal application with extensive technology and data interoperability related investments that have statewide benefits. Several states include information system initiatives that can scale care coordination statewide, including initiatives to build dedicated teams for analytics, data integration, and evaluation and tracking outcomes across initiatives. They have an opportunity to create the statewide backbone—starting with rural hubs and then expanding interfaces systemwide. States also will be advancing consumer-facing technology for preventive and chronic care, grounded in statewide health information exchange (HIE) and data strategy, again testing first in rural settings and accelerating statewide adoption of effective approaches.
- Maternal Health & Perinatal Care. Several states proposed embedding family medicine with obstetrics fellowships, expanding doula/midwife pathways, and deploying remote prenatal monitoring with support from nursing teams. These rural pilots could help standardize practice, improve outcomes, and scale across the state. Many other state proposals explicitly include initiatives to strengthen access to maternity care, linked to broader workforce and technology investments that can be adopted in urban settings.
- EMS Modernization. States also plan to develop and strengthen emergency medical services (EMS)-led preventive and complex care support in rural areas. One application, for example, formalizes such EMS-led support in rural areas, with protocols and training designed to scale broadly. Another state references mobile health and EMS integration, creating rural pilots to improve response, navigation, and handoffs that can be standardized across the emergency care system.
Looking Ahead
RHTP is more than a funding stream. It is a catalyst for innovation and collaboration, providing an important avenue to address the chronic inequities in quality, access, and outcomes that people living in our nation’s rural communities often experience. But it also could foster improvement statewide. Program evaluation and performance monitoring of the small, community-based programs and the large-scale, multi-site, multi-year initiatives will provide insights that inform strategic decision-making at the local, state and federal levels. By scaling effective rural health-focused initiatives and investing in new and feasible tools, strategies, and programs, states can create models that improve care delivery for all their residents in the future. This is a moment for states, providers, and partners to think big and design programs that deliver lasting impact.
Health Management Associates (HMA) offers support to state agencies, health systems, and community partners shaping rural-first pilots that are designed for scalability—from maternal and perinatal care networks, EMS community care models, caregiver and CHW pipelines, to telehealth modernization and behavioral health integration. Our rural expertise and our unique ability to combine expertise in clinical, operational, policy, and data reforms for care improvement are well-suited to the goals of RHTP.
With the RHTP funding advancing to state partners early in 2026 and annual recalculations of state awards tied to performance, the time to design rural pilots that become statewide programs is now.
For questions about the RHTP opportunities for your organization and the solutions HMA can tailor to meet the needs of your state, contact Kathleen Nolan and Andrea Maresca.
Connecting the Dots: A new blog series for 2026
Connecting the Dots is a monthly HMA blog series that brings together insights from our experts to examine the major policy, program, and market forces shaping healthcare coverage, delivery systems, and financing in 2026. The posts look beyond individual changes, instead connect emerging developments across programs and markets to help leaders understand what’s changing, why it matters, and how their decisions shape the path ahead.
CBO’s New Baseline Signals Shifting Cost and Risk Dynamics in Medicaid and Medicare
On February 11, 2026, the Congressional Budget Office (CBO) released The Budget and Economic Outlook: 2026 to 2036 report. The publication, which represents the first time CBO has released Medicare and Medicaid spending baseline projections since January 2025, reflects the impact of the 2025 Budget Reconciliation Act (P.L. 119-21, OBBBA), recent changes to Medicare reimbursement for skin substitute products, and the latest Medicare Part D and Medicare Advantage bids.
CBO’s baseline serves many functions, including serving as the official “scorekeeping” benchmark used for cost estimates of proposed legislation under consideration in Congress.
Changes to CBO’s Medicaid Baseline
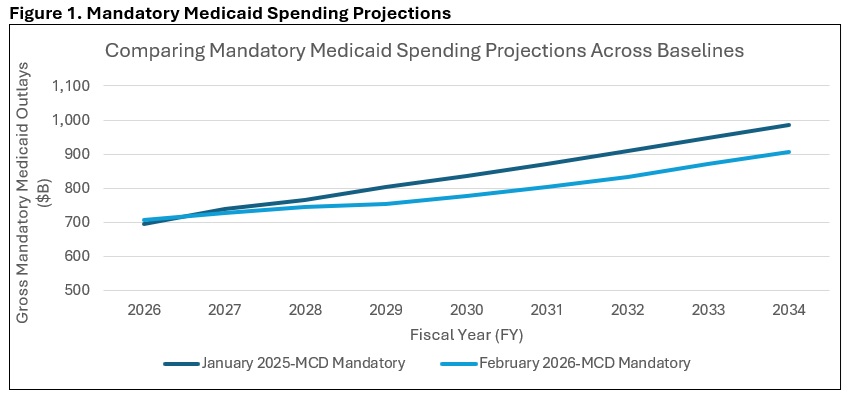
CBO decreased its projections of 2026–2035 Medicaid mandatory outlays by approximately $514 million from its January 2025 baseline update. The main driver of that reduction is the impact of the Medicaid provisions in the 2025 Budget Reconciliation Act, which CBO expects will reduce total Medicaid enrollment by 13.1 million people in 2035. The drop in Medicaid spending from the OBBBA-related enrollment reductions was partially offset by technical changes CBO made to the Medicaid baseline.
Medicaid costs per enrollee grew by 16 percent in 2025, which was more than CBO had anticipated. The agency attributes the cost per enrollee growth to a reported decrease in the average health status of Medicaid enrollees following the end of the COVID-era continuous eligibility policy.
CBO anticipates that payment rates for Medicaid managed care plans will begin to rise in 2026 because of this decrease in the average health status of enrollees, and the agency has updated the Medicaid baseline accordingly (see Figure 1).
Changes to CBO’s Medicare Baseline
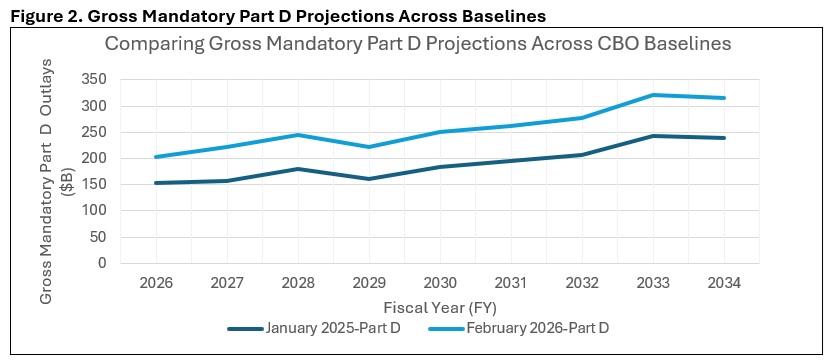
Compared with its January 2025 baseline, CBO increased its projections of Medicare’s 2026–2035 mandatory outlays by about $1 trillion (roughly $942 billion, by Health Management Associates (HMA) calculations). The main driver of that increase came from CBO’s updates to its Medicare Part D spending projections, which were increased to reflect higher than expected 2026 bids from private insurance plans that administer the Part D benefit. According to their 2026 bids, Part D plans anticipate a 35 percent increase in their annual per enrollee costs in 2026—a trend that CBO was not expecting and wants to study further. Part D spending per beneficiary in 2035 is now projected to exceed $4,000, up from less than $3,000 in the January 2025 baseline (See Figure 2).
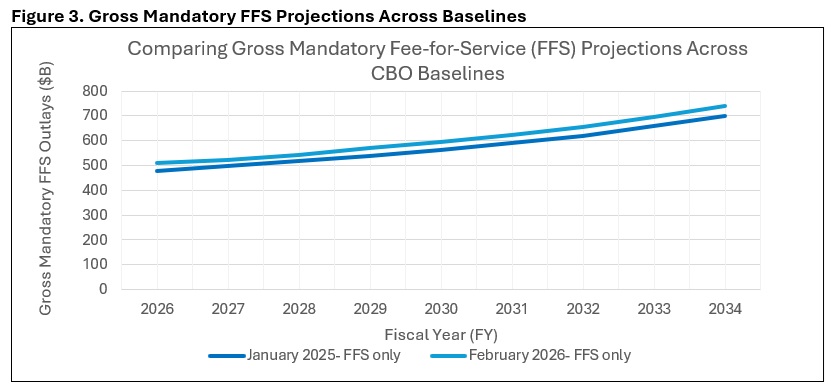
The agency’s Medicare Part A fee-for-service (FFS) spending projection increase was the result of larger than expected increases in 2025 enrollment and per enrollee spending. Those trends were also seen in Medicare Part B FFS but were partially offset by the Centers for Medicare & Medicaid Services’s (CMS) recent reimbursement changes to skin substitute products. Overall, CBO estimates that the skin substitute reform issued in CMS’s Medicare Physician Fee Schedule (MPFS) and Outpatient Prospective Payment System (OPPS) CY 2026 final rules will save $245 billion over the 2026–2035 period, including the effects on the Medicare Advantage (MA) program (see Figure 3).
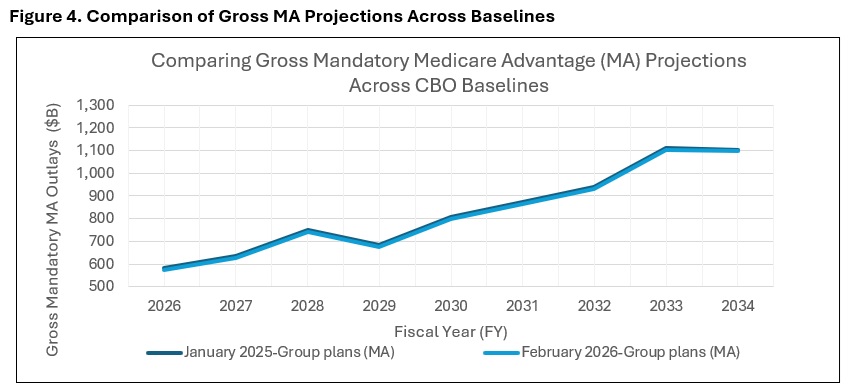
Finally, CBO reduced its spending projections for MA compared to the January 2025 baseline. This change was made to reflect lower-than-expected Medicare Advantage enrollment in 2025, although the spending implications of lower enrollment were partially offset by higher-than-expected bids in 2026 by providers of MA plans (see Figure 4).
Contact an HMA Expert Today
Interested in understanding how CBO’s latest baseline update affects the federal budgetary implications of certain Medicare or Medicaid policy topics or proposals? Contact our experts, Mark Desmaris and Rachel Matthews, to learn more about HMA’s “CBO-style” federal budgetary scoring work, which relies on The Moran Company’s long-standing methodology. [1]
Beyond federal budget scoring, HMA is working with states, health plans, and providers to assess how changes in enrollee health status are affecting utilization, costs, and payment rates—and what those trends may mean for Medicaid and MA organizations and providers. Our teams support states in evaluating managed care rate setting and program design, help Medicaid and MA plans anticipate risk and bid implications, and assist providers in understanding how changes in patient acuity could affect care delivery, contracting, and financial performance.
[1]Specifically, we apply our understanding of CBO precedents to predict how CBO will likely evaluate the budgetary impact of the legislation in question. We use our best judgment to adopt the assumptions CBO would tend to use, with the understanding that any variance in the assumptions CBO ultimately adopts could cause our estimate to differ from theirs.
Federal Policy News
Fueled By Leavitt Partners Weekly Health Intelligence
Leadership Changes at HHS Mark a New Phase for 2026 Priorities
Last week, the US Department of Health and Human Services (HHS) announced several changes to its leadership team, including the appointment of staff to new roles and the departure of Acting Centers for Disease Control and Prevention (CDC) Director and Deputy Secretary of HHS Jim O’Neill from the Department. Following Mr. O’Neill’s announced departure, on February 18, it has been reported that Jay Bhattacharya—currently serving as Director of the National Institutes of Health (NIH)—has been appointed Acting Director of the Centers for Disease Control and Prevention (CDC).
Alongside Mr. O’Neill, it had been reported that HHS General Counsel Mike Stuart would depart from his role, however, HHS spokesperson Andrew Nixon posted on social media that, Mr. Stuart “continues to serve as HHS General Counsel pending his appointment to a position in the administration where he will continue to focus on fighting fraud for hardworking taxpayers.”
Additionally, HHS formally announced several additions to the Secretary’s team of counselors, including the appointment of Chris Klomp, who has been serving as deputy administrator of the Centers for Medicare & Medicaid Services (CMS) and director of Medicare, to the role of Chief Counselor of HHS, as well as the appointment of both Kyle Diamantas, US Food and Drug Administration (FDA) Deputy Commissioner for Human Foods, and Grace Graham, FDA Deputy Commissioner for Policy, Legislation, and International Affairs, to the role of FDA Senior Counselors, and John Brooks, CMS Chief Policy and Regulatory Officer, to the role of CMS Senior Counselor. The staff will generally retain their current roles, in addition to joining the Immediate Office of the Secretary. Following this formal announcement by HHS, via internal communications, it was also announced that HHS Chief of Staff Matt Buckham will become “senior counselor for operations and personnel,” and Ken Callahan, the Chief Policy Adviser, will become senior counselor for policy.
HRSA Issues RFI on 340B Pilot as Agency Weighs Next Steps
On February 13, the Health Resources & Services Administration (HRSA) issued a Request for Information (RFI) on a potential new 340B rebate model pilot program. The RFI comes in the wake of HRSA cancelling a model that was anticipated to launch this year. The decision to suspend the initial model came after the American Hospital Association and several other 340B covered entities brought legal challenges to the pilot program, and a district court judge issued a blocking implementation which was then upheld, halting the model program. In a February 5 joint filing related to the litigation, HHS agreed to halt implementation of the planned model and issue a new notice, including soliciting new manufacturer applications, should the administration decide to implement a new 340B rebate program in the future. HHS also agreed to solicit comments in conjunction with such a new program.
In the RFI, HRSA requests stakeholders, including covered entities and manufacturers, respond to several questions concerning the implementation of a new model and related potential challenges. HRSA asks for detailed responses and relevant data from 340B covered entities on administrative costs, impacts on cash flow and financial sustainability, as well as privacy and security concerns related to patient information and data submission. HRSA also invites input from stakeholders regarding opportunities in the program’s design to offset such concerns, including offsets for administrative and operation costs and a potential requirement for rebates to be paid to covered entities within 10 days. The RFI also requests information from manufacturers regarding multiple aspects of the model, including data on their experience with duplicate discounts, as well as required reporting associated with participation in the program. Responses to the RFI are due by March 19.
FDA Begins Revising Safety Warnings for Hormone Replacement Therapies
On February 12, the US Food and Drug Administration (FDA) announced approval of labeling changes for six hormone replacement therapy (HRT) products for menopause, removing certain “black box” warnings of risk for breast cancer, cardiovascular disease, and dementia. FDA notes that it has received requests from 29 drug companies for proposed label changes, and that the six approved are “the first batch.” In November, FDA issued an announcement that it was initiating actions to remove the “black box” warnings, stating that FDA had originally applied the warnings following a Women’s Health Initiative study that found a “statistically non-significant increase in the risk of breast cancer diagnosis” after HRT use.
Revised 988 Lifeline Bill Directs FCC to Examine Geolocation Challenges
On February 12, the Senate Committee on Commerce, Science, and Transportation voted to advance eight bipartisan bills out of committee, including S. 3199, the 988 Lifeline Location Improvement Act of 2025, with a substitute amendment. While the introduced legislation would have required the Federal Communications Commission (FCC), in coordination with HHS, to establish an advisory committee to address challenges in transmitting geolocation information with calls to the 988 Suicide and Crisis Lifeline, Senator Ben Ray Luján’s (D-NM) substitute amendment was adopted and directs FCC to initiate a notice of inquiry to address such challenges within 270 days of enactment.
In assessing responses to the inquiry, the substitute amendment directs FCC to consider a range of factors related to requiring transmission of geolocation information, including legal authorities, protection of consumer privacy, feasibility and technical implementation standards, an assessment of potential costs and funding requirements, technical challenges for users who access the 988 American Sign Language line, and technologies currently available to provide dispatchable location information and relaying it from 988 to 911 centers. The substitute also requires GAO to study and report on the opportunities and challenges associated with implementing geolocation for the 988 Suicide and Crisis Lifeline within 180 days of the bill’s enactment. In developing the report, GAO is directed to consult with a range of relevant stakeholders.
Ready to talk about your organization's challenges?
Schedule a Consultation
State Policy News
Florida
Florida House Proposes to Continue Medicaid MCO Withhold Policy. Florida Politics reported on February 12, 2026, that the Florida House of Representatives fiscal 2027 budget proposal includes a provision that would require the Agency for Healthcare Administration to continue withholding two percent of Medicaid managed care organizations’ (MCO) capitation payments, which has been in place since October 2025, and require the MCOs to meet certain metrics to earn some of it back. Under the proposal, only two of the eight MCOs in Florida could earn back the two percent, by having the largest reduction of the infant mortality rate and by reporting the greatest reduction in the number of infant mortality cases. Other plans could receive some of the withheld payments by showing improvements year over year. The Senate has yet to release its budget proposal.
Hawaii
Hawaii Issues Behavioral Health Services for Community Care Services Program RFP. The Hawaii Department of Human Services released on February 16, 2026, a request for proposals (RFP) seeking a single qualified behavioral health organization (BHO) to provide statewide behavioral health services through the Community Care Services Program (CCS) to Medicaid eligible adults diagnosed as seriously mentally ill and seriously and persistently mentally ill covered by QUEST Integration (QI) Health Plans. The BHO will be responsible for providing intensive and basic behavioral health services while ensuring that beneficiaries’ behavioral health services are integrated with physical health needs. The incumbent BHO is Centene/Ohana Health Plan. Responses are due March 20, 2026, and Hawaii estimates it will award the contract around April 10, 2026. The contract, worth approximately $60 million per year, would begin July 1, 2026, and run through June 30, 2029, with three optional one-year renewals.
Iowa
Iowa Awards $78.6 Million in Grants to Implement RHTP. Iowa Governor Kim Reynolds announced on January 30, 2026, that the state Department of Health and Human Services has awarded over $78.6 million in grants after undergoing two requests for proposals (RFPs) to find organizations that will help the state implement the federal Rural Health Transformation Program (RHTP). The grants support the Hometown Connections initiative of Iowa’s RHTP, called the Healthy Hometowns Project, which aims to build partnerships to restructure rural healthcare delivery options. Iowa announced $66 million for awardees of the Medical Equipment Procurement and Installation RFP and $12.6 million for awardees of the Health Care Workforce Recruitment RFP. The medical equipment dollars will fund imaging systems, robotic surgical systems, and other advanced equipment, and the workforce dollars will fund physicians, advanced practice providers, physician assistants, registered nurses, and specialty providers.
Nevada
Nevada Re-Releases Children’s Specialty Managed Care Plan RFP. The Nevada Health Authority re-released on February 12, 2026, a request for proposals (RFP) seeking plans to administer risk-based capitated managed care services for children and youth with complex behavioral health needs. This procurement will establish a new Children’s Specialty Managed Care Plan designed to improve access to physical health, behavioral health, and pharmacy services for children and young adults with behavioral health disabilities who are involved in the child welfare system. The primary goals of the specialty plan are to improve health outcomes for enrollees, support enrollees living at home with their family or caregiver in their communities and ensure compliance with the Department of Justice Settlement Agreement that led to the creation of the program. Nevada intends to award one contract with an initial term effective July 1, 2027, through December 31, 2030, and the option for a two-year extension. Proposals are due May 1, 2026. The notice of intent to award is expected around June 13, 2026, and final awards are expected to be announced around July 28, 2026.
New York
New York Receives CMS Approval for Extension of MCO Tax. Crain’s New York Business reported on February 12, 2026, that New York has received a nine month extension from the federal government for its Medicaid managed care organization (MCO) tax. The extension is estimated to generate an extra $1.2 billion for the state. The New York Department of Health currently holds an existing $1.4 billion in MCO taxes, and lawmakers have questioned how health officials plan to allocate all of the current and incoming revenue.
Oregon
Oregon Announces $25 Million in Grants for CBOs to Advance Health Equity. The Oregon Health Authority announced on February 11, 2026, that it has awarded $25 million in grants to 125 community-based organizations (CBOs) to help aid in improving public health equity. The funding, which is available through OHA’s Partnerships for Community Health Program, will support long-term public health efforts between January 1, 2026, and June 30, 2027, related to adolescent and school health, communicable disease prevention, commercial tobacco prevention, community resilience, environmental public health, overdose prevention, and preventing environmental exposures for children’s health. The grant award aims to improve health outcomes, increase healthcare and prevention service access, and eliminate health inequities.

Private Market News
Fueled By Wakely Consulting Group
Centene Sells Magellan Health to Madison Health Group
Health Payer Specialist reported on February 17, 2026, that Centene has sold its behavioral health provider Magellan Health to Madison Health Group for an undisclosed amount. The deal is pending regulatory approval.
Humana Acquires Primary Care Provider MaxHealth
Modern Healthcare reported on February 17, 2026, that Humana has acquired MaxHealth, a primary care provider focused on Medicare, Medicare Advantage, and managed Medicaid patients in Central and South Florida, in a deal reportedly valued at nearly $1 billion. The acquisition adds dozens of clinics and more than 100 providers to Humana’s CenterWell primary care network, further expanding its footprint in Florida. MaxHealth serves over 80,000 Medicare Advantage members and strengthens Humana’s strategy of vertically integrating insurance and primary care to better manage senior populations and control costs.
Our Insights
Fueled By Experts Across Our HMA Companies
Health Management Associates
Lessons Learned from HealthySteps Technical Assistance in California
This report synthesizes insights from multiple efforts to support the financial sustainability of HealthySteps sites in California, including federally qualified health centers (FQHCs), community clinics (non-FQHCs), private practices, and other settings. Led by the HealthySteps National Office and Health Management Associates (HMA), the technical assistance (TA) elevated challenges, strategies and best practices to achieve sustainability informed by learning collaboratives, individualized TA sessions, and financial modeling exercises. This report complements additional resources that the HS National Office and HMA developed.
Wakely
The Value Shift: Inside the C-SNP Surge
Chronic Condition Special Needs Plans (C-SNPs) are rapidly reshaping the Medicare Advantage landscape heading into 2026, evolving from a niche product into one of the fastest-growing MA segments. Part of Wakely’s The Value Shift series, this whitepaper examines how C-SNP growth has been highly concentrated by condition and geography, driven primarily by plans targeting diabetes, cardiovascular disease, and chronic heart failure, while many other CMS-approved chronic conditions and markets remain underserved. Using Wakely’s Medicare Advantage Competitive Analysis Tool (WMACAT) and Strategic Market Analysis and Ranking Tool (SMART), the paper analyzes plan growth, enrollment patterns, geographic concentration, and benefit design trends from 2025 to 2026. The findings highlight a market that is expanding quickly but unevenly, underscoring the need for clear strategy, condition-aligned benefit design, and operational readiness as C-SNPs play an increasingly central role in Medicare Advantage portfolios.
Managed Medicaid Enrollment and Profitability 2019-2025
Managed Medicaid Care has experienced several policy shocks in recent years. As a result of Families First Coronavirus Response Act (FFCRA), starting in March 2020 states were given extra Medicaid funding on the condition that the states maintained continuous enrollment. Between February 2020 and April 2023 Medicaid enrollment grew from 66 million to 87 million. Continuous enrollment ended as a result of another Congressional act (the Consolidated Appropriation Act) and the end of the Public Health Emergency (PHE) which enabled states to begin Medicaid renewals and disenrollments starting in April 2023. The ending of continuous enrollment and implementation of Medicaid disenrollment resulted in massive changes to the Medicaid population as over 31% of those people who had their coverage redetermined were disenrolled. The purpose of this report is to look at managed Medicaid profitability and enrollment prior to, during, and following the continuous enrollment period.
Webinar: PACE: Advance Notice Review
In this webinar, experts from Wakely will be reviewing changes to the PACE program announced in the recent 2027 Medicare Advantage and Part D Advance Notice published by CMS on January 26, 2026. Primary amongst these changes, the risk adjustment model transition for PACE programs from the legacy Risk Adjustment Processing System (RAPS) to the encounter data system (EDS) is accelerating to a 50/50 weighting in 2027. The webinar will also review how the commonly quoted Effective Growth Rate translates to PACE plan Medicare revenue in 2027. Finally, the webinar will discuss how all of the model changes coming to the Medicare Part D program affect PACE plans. How will these changes impact your organization’s bottom line? Tune in to learn more.
Leavitt Partners
Policy Brief on Addressing the Health Care Needs of People with Intellectual and/or Developmental Disabilities (I/DD)
Individuals with intellectual and/or developmental disabilities (I/DD) face disproportionate difficulties in accessing high-quality healthcare services, and experience poorer health outcomes and ultimately shorter lifespans than the general population. To help improve the lives of people with I/DD, Special Olympics has promoted the concept of Inclusive Health, a set of principles designed to ensure that people with I/DD have access to, and can fully participate in, their own healthcare decisions. In a workshop during the Summer of 2025, Leavitt Partners and Institute for Exceptional Care (IEC) convened people with I/DD, their caregivers, physicians, payers, and health policy experts with state and federal expertise to discuss how to advance Inclusive Health models. Insights from that workshop are included in this policy brief.
Watch the February 12, 2026 webinar here for additional insights.
RFP Calendar
RFP Calendar
| Date | State/Program | Event | Beneficiaries |
|---|---|---|---|
| Date: February 2026 | State/Program: Illinois | Event: Awards | Beneficiaries: 2,400,000 |
| Date: March 20, 2026 | State/Program: Hawaii Community Care Services | Event: Proposals Due | Beneficiaries: 5,500 |
| Date: April 10, 2026 | State/Program: Hawaii Community Care Services | Event: Awards | Beneficiaries: 5,500 |
| Date: May 1, 2026 | State/Program: Nevada Children's Specialty | Event: Proposals Due | Beneficiaries: NA |
| Date: May 12, 2026 | State/Program: Nevada CO D-SNP | Event: Awards | Beneficiaries: 88,000 |
| Date: June 24, 2026 | State/Program: Wisconsin LTC GSR 3 | Event: Awards | Beneficiaries: 56,000 (all GSR) |
| Date: July 1, 2026 | State/Program: Hawaii Community Care Services | Event: Implementation | Beneficiaries: 5,500 |
| Date: July 28, 2026 | State/Program: Nevada Children's Specialty | Event: Awards | Beneficiaries: NA |
| Date: August 2026 | State/Program: Indiana | Event: RFP Release | Beneficiaries: 1,400,000 |
| Date: January 1, 2027 | State/Program: Illinois | Event: Implementation | Beneficiaries: 2,400,000 |
| Date: January 1, 2027 | State/Program: Nevada CO D-SNP | Event: Implementation | Beneficiaries: 88,000 |
| Date: January 1, 2027 | State/Program: Wisconsin LTC GSR 3 | Event: Implementation | Beneficiaries: 56,000 (all GSR) |
| Date: January 1, 2027 | State/Program: Illinois Tailored Care Management Program | Event: Implementation | Beneficiaries: 22,400 |
| Date: July 1, 2027 | State/Program: Nevada Children's Specialty | Event: Implementation | Beneficiaries: NA |
| Date: January 1, 2028 | State/Program: Wisconsin LTC GSR 4,6 | Event: Implementation | Beneficiaries: 56,000 (all GSR) |
| Date: Fall 2027 | State/Program: Oregon | Event: RFP Release | Beneficiaries: 1,200,000 |
| Date: 2028 | State/Program: North Carolina | Event: RFP Release | Beneficiaries: 2,200,000 |
| Date: 2029 | State/Program: California | Event: RFP Release | Beneficiaries: NA |