December 4, 2024
This week's roundup:
- In Focus: CMS Proposes Major Changes to Medicare Advantage and Part D for 2026

- California Establishes 15 Percent Primary Care Spending Target by 2034
- Florida Medicaid Managed Care Contracts Worth $143 Billion Over Six Years
- Georgia Awards Medicaid Managed Care Contracts to Four Plans
- Maryland Submits Section 1115 Demonstration Amendment for Housing Support Services
- Michigan Re-Awards Same Plans for MI Coordinated Health HIDE SNP
- Washington Releases TPA for Medicaid Reentry Services RFP
- Wakely Releases Analysis of Potential Election Impacts on the Individual Market
- CMS Revises Centene, UnitedHealth Medicare Advantage Star Ratings
- UnitedHealthcare CEO Brian Thompson Fatally Shot Ahead of Investor Meeting
- More News Here
In Focus
CMS Proposes Major Changes to Medicare Advantage and Part D for 2026
This week, our In Focus section reviews a comprehensive proposed rule that the Centers for Medicare & Medicaid Services (CMS) released November 26, 2024. These highly anticipated regulations—which represent the last major Medicare regulations from the Biden Administration—include several significant and far-reaching proposals designed to strengthen plan oversight and enhance beneficiary protections for millions of Medicare beneficiaries who have coverage through Medicare Advantage and Medicare Part D plans beginning in contract year 2026. The rule also comprises proposals with fiscal and policy implications for state Medicaid programs.
Comments on the proposed rule are due by January 27, 2025, and the incoming Trump Administration could make significant changes before finalization. New administration officials may choose to delay certain provisions, scale back, or eliminate certain proposed policy changes when they finalize the regulations next year.
This article explains several of the proposed policies, considerations for healthcare stakeholders, and developments that Health Management Associates (HMA) experts will be tracking in the coming weeks.
Coverage of Anti-Obesity Medications Under Medicare Part D and Medicaid
In the proposed regulations, CMS seeks to expand coverage of anti-obesity medications (AOMs) under the Medicare Part D and Medicaid programs. Under current Medicare Part D coverage rules, medications used exclusively for weight loss are excluded from the definition of a Part D covered drug. Through the proposed change, CMS is seeking to align Medicare and Medicaid coverage policy with the prevailing medical consensus that recognizes obesity as a chronic disease.
Under the proposed reinterpretation, CMS would expand eligibility for Part D coverage of AOMs for Medicare beneficiaries with obesity. AOMs used for weight loss or chronic weight management would continue to be excluded from Part D coverage under the proposed regulation.
As it relates to Medicaid, CMS’s proposed reinterpretation would require Medicaid coverage for anti-obesity medications when used for weight loss or chronic weight management for the treatment of obesity. State Medicaid programs would continue to have discretion to use preferred drug lists and prior authorization (PA) to establish certain limitations on the coverage of these drugs, consistent with existing statutory requirements.
CMS estimates the proposal would increase federal costs by $24.8 billion as the result of expanded Part D coverage and $14.8 billion because of expanded Medicaid coverage over a 10-year period.
Key considerations: Though expanded access to innovative medications may improve access and outcomes for obese patients, these considerations may need to be balanced against the proposal’s considerable fiscal costs. In addition, key health nominees put forth by President-Elect Donald J. Trump have different views about how best to prevent and treat chronic disease, creating additional uncertainty about whether this proposed expansion will go forward.
Strengthening Prior Authorization and Utilization Management Guardrails
The proposed rule includes a series of recommendations for reforming Medicare Advantage PA, utilization management (UM), and coverage decisions, which include:
- Defining the meaning of internal coverage criteria to clarify when MA plans may apply UM
- Ensuring MA plans’ internal coverage policies are transparent and readily available to the public
- Requiring plans to inform beneficiaries of their appeal rights
- Revising the current metrics for the annual health equity analysis on the use of PA to require more detailed and granular reporting to allow CMS to determine whether MA plans disproportionately deny certain services
Key considerations: Continued scrutiny of MA plans’ PA practices and strong bipartisan support for reforms increase the likelihood that certain changes will be made to these policies within the next year.
Enhancing Medicare Plan Finder to Include Information on Plan Provider Directories
Another notable proposal would require MA plans to make provider directory data available to CMS for inclusion in Medicare Plan Finder (MPF), the online tool that allows beneficiaries to compare coverage options, including Medicare Advantage and Part D plans. At present, provider directories must be accessible on MA plans websites.
CMS seeks to enhance MPF with searchable provider information for all MA plans while requiring plans to attest to the accuracy of the provider directory data, including updating data within 30 days of receiving notification that provider information has changed. CMS would ensure compliance with this expectation by requiring plans to meet data compliance and quality checks, which will be detailed in upcoming technical guidance.
Improving Access to Behavioral Health Care
The proposed rule furthers federal policymakers’ initiatives to address the nation’s behavioral health crisis. CMS proposes to establish the following three standards to ensure that beneficiary cost sharing in Medicare Advantage is no greater than in Traditional Medicare:
- A 20 percent coinsurance or an actuarially equivalent copayment rate for mental health specialty services, psychiatric services, partial hospitalization, and outpatient substance abuse services
- No cost sharing for opioid treatment programs
- All (100 percent) of the estimated Traditional Medicare cost sharing for inpatient psychiatric services
Improve Oversight and Administration of Supplemental Benefits
MA plans may offer a variety of supplemental benefits such as vision, dental, and gym memberships, which have come under increasing scrutiny by CMS. CMS proposed several actions to reduce misuse of these benefits, including:
- Outlining proper usage by MA organizations and enrollees
- Adding disclosure rules for transparency
- Ensuring enrollees can access covered services through alternative methods
- Requiring real-time electronic links between debit cards and covered services
- Defining acceptable over-the-counter products.
Key Considerations: CMS officials in President-Elect Trump’s first administration expanded flexibility for plans to offer supplemental benefits. Incoming policy officials may seek an opportunity to fully review the Biden Administration’s proposals. Data and experience-informed comments from MA plans and stakeholders can support such discussions.
Improve Care Experience for Dual Eligibles
CMS proposed the following two new federal requirements for Dual Eligible Special Needs Plans (D-SNPs) that are applicable integrated plans (AIPs):
- AIP D-SNPs will need to have integrated member ID cards for their Medicare and Medicaid plans.
- D-SNPs will be required to conduct an integrated health risk assessment for Medicare and Medicaid, rather than separate ones for each program.
Key Considerations: These proposals further CMS’s multi-year work to advance integrated care by applying Medicare-Medicaid Plan features into D-SNP requirements. States and MA and Medicaid plans should plan for operational and policy changes if the proposals are finalized.
Formulary Inclusion and Placement of Generics and Biosimilars
CMS proposes to require Part D formularies to provide beneficiaries with broad access to generic, biosimilar, and other low-cost drugs while also ensuring that tier placement and UM practices do not limit access to these drugs as compared with more expensive brand name and reference products.
Key considerations: If finalized, the proposal would require MA-PD and Part D plans to update their approach and considerations for plan formulary development. Consumer groups and other stakeholders should consider the possibility that the proposal will improve access to lower cost products.
Other Topics in the Proposed Rule
In addition, the proposed rule calls for the following:
- Guardrails for artificial intelligence to protect access to health services, such as requiring that MA plans ensure services are provided equitably, regardless of delivery method or origin (i.e., human or automated systems)
- Changes to MA and Part D medical loss ratio (MLR) reporting to improve the meaningfulness and comparability of MLR across plan contracts
- Expanded Part D medication therapy management eligibility criteria
- Adding and updating measures addressed in this proposed rule, beginning with the 2028 Star Ratings
- Promoting community-based services and enhancing transparency of in-home service providers, including new definitions and standards for community-based organizations
- Codifying existing guidance related to implementation of the Medicare Prescription Payment Plan, which is part of the Inflation Reduction Act (IRA)
What to Watch
During the lame duck session, Congress could advance legislation related to some proposals in this rule. Specifically, PA has been an area of significant bipartisan interest, along with access to and cost of GLP-1 products. CMS will need to ensure the final MA and Part D policy and technical rule for contract year 2026 reflects approved statutory changes.
In addition, HMA is watching key appointments within the US Department of Health and Human Services, including individuals selected to lead CMS’ Medicare and Medicaid centers. These appointments will provide valuable insights on the emerging policy agenda of the incoming administration.
Connect with Us
HMA’s Medicare and Medicaid experts will continue to assess and analyze the policy and political landscape, which will determine the final policies in the MA and Part D policy and technical rule for contract year 2026. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist organizations that engage in the rulemaking process and to support implementation of final policies, including policy development, tailored analysis, and modeling capabilities, as well as quality improvement initiatives and plan benefit design.
For further analysis of the MA and Part D proposed rule and potential impact on MA and Part D plans, Medicaid programs, providers, and beneficiaries, contact Greg Gierer, Amy Bassano, and Julie Faulhaber.
HMA Roundup
Alaska
Alaska Releases MMIS Service Authorization Solution RFI. The Alaska Department of Health (DOH) issued on November 14, 2024, a request for information (RFI) seeking input regarding an electronic Service Authorization (SA) solution that could be implemented as part of Alaska’s Medicaid Management Information System (MMIS). The immediate need is to reduce the administrative burden and processing time required for manual entry and routing of prior authorizations. The state is looking for a vendor to offer direct data entry of SA requests; a configurable rules engine to automate or recommend approvals; system capability with minimal workflow routing; the ability for users to track the status of SAs during the review and approval process; and conformance to the Centers for Medicare & Medicaid Services 2024 Interoperability and Prior Authorization Final Rule. Responses are due December 10.
Arizona
Arizona Submits 1115 Amendment Request to Expand Coverage for Former Foster Youth. The Centers for Medicare & Medicaid Services announced on December 3, 2024, that Arizona has submitted an amendment request for its section 1115 Arizona Health Care Cost Containment System demonstration. Under the amendment, the state seeks to extend eligibility for Medicaid state plan benefits to former foster youth who are under age 26. The amendment aims to address chronic health conditions and health related social needs experienced by foster youth and former foster youth, including an increased prevalence of physical and behavioral health needs and higher rates of homelessness. Public comments will be accepted through January 1, 2025.
Arkansas
Arkansas PASSEs Request Exemption on Prior Authorization Restrictions. Health Payer Specialist reported on November 27, 2024, that several Arkansas Provider-Led Shared Savings Entities (PASSEs) are requesting approval from the state’s Legislative Council for an exemption on prior authorization restrictions, made available under provisions of the 2017 state law. The organizations include Summit Community Care, CareSource, Empower Healthcare Solutions and Arkansas Total Care. During the Arkansas Senate’s Public Health, Welfare and Labor Committee meeting, State Representative Lee Johnson stated that he expects additional amendments to the law in order to accommodate the requests.
Arkansas Governor Proposes $13 Million in New Medicaid Funding for Fiscal 2026. The Associated Press reported on November 21, 2024, that Arkansas Governor Sarah Huckabee Sanders proposed a nearly $6.5 billion budget for fiscal 2026, which includes $13 million in new Medicaid funding to pay for proposals issued by a panel she formed to address maternal health. The budget plan would also set aside $100 million of the state’s projected $300 million surplus for Medicaid.
California
California Establishes 15 Percent Primary Care Spending Target by 2034. KFF Health News reported on November 21, 2024, that California’s board of the state Office of Health Care Affordability has set a goal for insurers to direct 15 percent of their spending towards primary care by 2034. The current industry benchmark is to spend seven percent on primary care. The goal is part of California’s effort to expand access to primary care and preventative services, improve health management and disease prevention, expand the primary care workforce, and reduce costly care.
Florida
Florida Medicaid Managed Care Contracts Worth $143 Billion Over Six Years. Florida Phoenix reported on December 3, 2024, that Florida will pay insurers approximately $143 billion over six years to run the Statewide Medicaid Managed Care (SMMC) program, according to state legislators. The state announced SMMC contract awardees in April and July, and contracts are slated to begin in 2025.
Florida Delays Implementation of Canadian Prescription Drug Import Plan. KFF Health News reported on November 21, 2024, that Florida has not set a start date to implement its prescription drug importation plan, which the U.S. Food and Drug Administration (FDA) previously cleared to start in January 2024. The plan has bipartisan support but is opposed by the prescription drug industry, which has raised concerns over the imports causing an influx of counterfeit medications.
Georgia
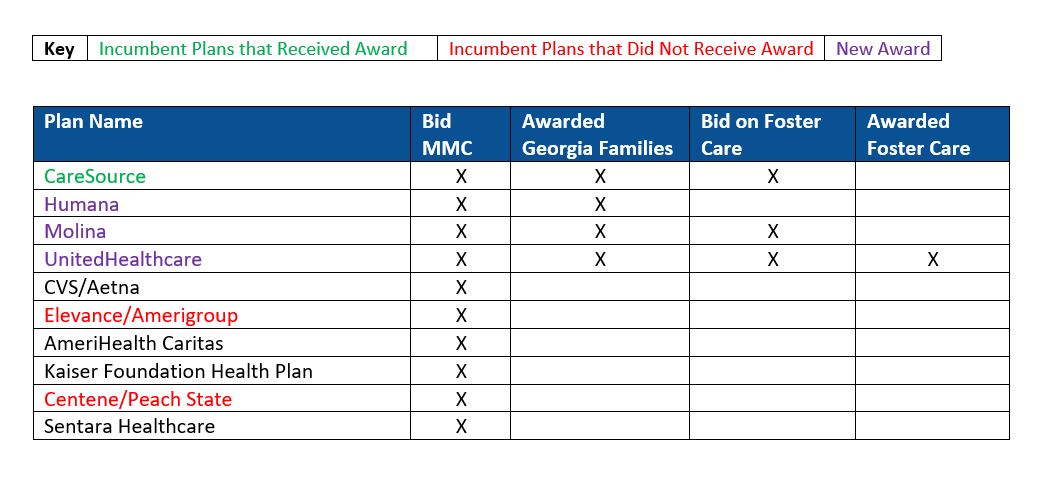
Georgia Awards Medicaid Managed Care Contracts to Four Plans. The Georgia Department of Community Health (DCH) released on December 2, 2024, award recommendations to four health plans for the Georgia Families and Families 360° program, covering approximately 1.5 million beneficiaries. Of the four plans, CareSource, which currently has under 377,000 lives, was the sole incumbent. New plans Humana, Molina, and UnitedHealthcare will serve the remaining 1.1 million lives. The RFP explains the open-enrollment and auto-assignment processes with the selected awardees. UnitedHealthcare was also awarded a contract for the Georgia Families 360° program which covers 27,000 children in foster care, adoption assistance, and certain juvenile justice programs. Under the procurement, Georgia intends to carve in select ABD populations into managed care through a phased approach. Only a subset of the ABD population will be included in the initial phase of the transition, beginning with SSI non-dual and non-home and community-based services members as of the effective date, and rolling in nursing home, non-SSI, and two HCBS waiver programs (elderly and physically disabled) in year three. While the award announcement does not specify a start date, current contracts were extended through June 30, 2026. Incumbents that were not awarded a contract are Elevance and Centene. Additional RFP documents can be found here.
Illinois
Illinois Extends Pharmacy Benefit Management System Contract with Change Healthcare through December 2025. The Illinois Healthcare and Family Services (HFS) released on November 25, 2024, a notice of emergency contract extension from December 13, 2024, through December 14, 2025, for the state’s pharmacy benefit management system (PBMS). The current PBMS was awarded through a competitive procurement in 2014 to Change Healthcare Pharmacy Solutions. Change Healthcare will continue to provide operations under the current PBMS to ensure continuity of medical and pharmaceutical care for the state’s Medicaid population.
Iowa
Iowa Senate Likely to Propose Medicaid Work Requirements. Radio Iowa reported on December 3, 2024, that Iowa Senator Mike Bousselot (R-Ankeny), chairman of the Senate Commerce Committee, stated that Senate Republicans are gearing up to propose work requirements for Medicaid coverage when the Iowa General Assembly reconvenes.
Maine
Maine Proposes Staffing Requirement Increases for Residential Care Facilities, Memory Care Units. ProPublica reported on November 27, 2024, that the Maine Department of Health and Human Services (DHHS) has proposed doubling the number of direct care workers at residential care facilities overnight and significantly increasing staffing requirements in memory care units. An investigation by The Maine Monitor and ProPublica into the state’s largest residential care facilities found numerous violations of resident rights, including incidents of abuse and neglect, and medication/treatment violations. DHHS must present its proposed regulations to lawmakers by January 10 in order for them to be considered in the upcoming legislative session.
Maryland
Maryland Submits Section 1115 Demonstration Amendment for Housing Support Services. The Centers for Medicare & Medicaid Services (CMS) announced on November 25, 2024, that the Maryland Department of Health submitted an amendment request for its Maryland Health Choice Section 1115 demonstration seeking expansion for the Assistance in Community Integration Services (ACIS) pilot program to update payment methodologies and increase participant slots to support housing and tenancy-based case management services for Medicaid enrollees. The amendment also seeks to cover fertility preservation procedures for people with or at risk of iatrogenic infertility and implement express lane eligibility for non-Modified Adjusted Gross Income adults. Public comments are open through December 25, 2024.
Michigan
Michigan Re-Awards Same Plans for MI Coordinated Health HIDE SNP. Health Payer Specialist reported on December 4, 2024, that Michigan has re-awarded contracts worth $6.9 billion to the same nine health plans for the MI Coordinated Health program, the state’s new Highly Integrated Dual Eligible Special Needs Plan (HIDE SNP), launching January 1, 2026. Awarded plans include incumbents CVS/Aetna, AmeriHealth Caritas, HAP/CareSource, Centene/Meridian Health Plan, Molina, and Upper Peninsula Health Plan, and non-incumbents: Humana, Priority Health Choice, UnitedHealthcare. Zing Health did not receive an award. Plans were awarded by region, and remain the same from the original award recommendation.
Mississippi
Mississippi Prenatal Presumptive Medicaid Eligibility Delayed Over Federal Law Compliance. The Clarion Ledger reported on November 21, 2024, that implementation for the Mississippi prenatal presumptive Medicaid eligibility program continues to be stalled due to pending federal approval and required legislative revisions. During a Senate hearing, Mississippi Division of Medicaid Executive Director Cindy Bradshaw stated that they are close to a resolution with the Centers for Medicare & Medicaid Services. The legislation, which was due for implementation on July 1, 2024, provides up to 60 days of prenatal presumptive Medicaid eligibility.
Nebraska
Nebraska to Strengthen Oversight of Medicaid-covered ABA for Autistic Youth. The Nebraska Examiner reported on December 4, 2024, that the Nebraska Department of Health and Human Services (DHHS) is considering stricter guardrails and parameters around applied behavioral analysis (ABA), a type of therapy for people with autism, after ABA costs rose more than 1,000 percent over three years. Agency officials attribute the rising costs in part to pay rate increases for ABA providers, relaxed telehealth rules, and more lenient controls over ABA compared to other disciplines, which officials said may be leading to over-authorization of services. DHHS aims to ensure appropriate billing practices and a sustainable program, and expects potential changes to roll out in 2025.
New Mexico
New Mexico Lawmakers to Introduce Private Option Bill, Remove Medicaid Eligibility Income Caps. The Santa Fe New Mexican reported on November 23, 2024, that New Mexico lawmakers are preparing to introduce a bill, called Medicaid Forward, during the upcoming legislative session that would reduce the financial requirements for Medicaid eligibility by removing income caps and allowing anyone to access Medicaid by paying 5 percent of their household income. The coverage options would be available through the Affordable Care Act Marketplace. It is expected that the bill would expand Medicaid coverage to nearly 300,000 individuals.
New York
New York Faces Lawsuit Over Single Statewide Fiscal Intermediary CDPAP Contract Decision. The Times Union reported on November 27, 2024, that Freedom Care LLC has filed a lawsuit against the New York Department of Health and Public Partnerships LLC (PPL) over New York’s decision to award PPL with the single statewide fiscal intermediary contract to run the $9 billion consumer-directed personal assistance program (CDPAP). The lawsuit alleges that the state health department tailored the CDPAP fiscal intermediary request for proposals in PPL’s favor, imposing eligibility requirements that eliminated many of PPL’s competitors. The suit also alleges that the state and PPL unlawfully coordinated before awards were announced. The state denies wrongdoing, claiming that the lawsuit’s allegations do not hold merit. Freedom Care is seeking to annul the contract.
New York to Impose Stricter Regulations on PBMs. Modern Healthcare reported on November 20, 2024, that New York has new rules taking effect this month to further regulate the state’s pharmacy benefit managers (PBMs). The regulations will require PBMs to publish lists of the drugs they cover and directories of pharmacies in their networks, prohibit PBMs from directing patients to affiliated pharmacies, and prohibit them from barring small pharmacies from offering mail-order and home delivery of prescriptions.
North Dakota
North Dakota Seeks Public Feedback on 2025-2027 Medicaid Quality Strategy. KXNET reported on November 29, 2024, that the North Dakota Department of Health and Human Services (HHS) is looking for input on the latest draft of its 2025-2027 Medicaid Quality Strategy. The new three-year plan summarizes the work that will be done to monitor and improve the quality of care and services provided by state Medicaid programs. Goals of the new strategy include improving preventative health, postpartum care, and behavioral health; improving outcomes for members with substance use disorders and chronic conditions; enhancing member experience; and focusing on value-based care. Public comments will be accepted through December 30, 2024.
Oregon
Oregon Releases MES System Integration RFI. The Oregon Health Authority (OHA), released on November 26, 2024, a request for information (RFI) seeking feedback regarding the integration and enhancement of OHA’s Medicaid Enterprise System (MES). The agency is looking for input from qualified vendors on possible solutions for system integration services and a system integration platform to help improve efficiency, data accessibility, and service delivery. Responses are due January 16, 2025.
OR Releases State-Based Marketplace Vendor RFP. The Oregon Health Authority (OHA)released on November 22, 2024, a request for proposals (RFP) seeking a state-based insurance marketplace vendor to comply with enrolled Senate Bill 972, which requires OHA to transition from the federal Marketplace to a state-based platform for open enrollment beginning in 2027. The state will award one or more vendors to administer an information technology platform and call center, which must be ready by November 1, 2026. This RFP replaces the previous state-based marketplace vendor RFP issued in July 2024. Proposals are due December 30, 2024.
Oregon Behavioral Health Resource Networks See Increased Client Utilization. The Oregon Health Authority reported on November 20, 2024, that utilization of Behavioral Health Resource Networks (BHRNs), which connect substance users with services and treatment, grew in the last quarter ending June 30, 2024, according to the state’s quarterly report. Client encounters rose from 248,651 to 299,662 during this time. The newly reported data was collected after legislative reforms to Measure 110 were passed but have yet to be fully implemented. Measure 110, which established and funded BHRNs, was recently amended to decriminalize most unlawful possession of a controlled substance offenses. The report also showed supported employment, peer services, and housing supports have more than tripled since BHRNs launched.
Texas
Texas Requests Funding to Address Delays in Processing Medicaid Applications. KXAN reported on November 21, 2024, that Texas has nearly 233,000 overdue Medicaid applications that are out of compliance with federal timeliness standards. The Texas Health and Human Services Commission (HHSC) has requested more than $391 million in their biannual legislative appropriations request to streamline their processing of applications and avoid federal penalties. The average wait time for Texas Works Medicaid and the Children’s Health Insurance Program is 71 days, which is nearly a month longer than the timeframe allowed under federal rules. HHSC has been under a Corrective Action Plan from the federal government since 2020.
Utah
Utah Submits 1115 Medicaid Reform Demonstration Amendment for Traditional Healing Services. The Centers for Medicare & Medicaid Services announced on December 3, 2024, that Utah has submitted an amendment request for its section 1115 Medicaid Reform demonstration. The amendment seeks to reimburse for traditional healing services provided by a traditional healing provider in an eligible facility to Medicaid enrollees who are members of an American Indian or Alaskan Native tribe. Public comments will be accepted through January 1, 2025.
Washington
Washington Releases TPA for Medicaid Reentry Services RFP. The Washington State Health Care Authority released on November 22, 2024, a request for proposals (RFP) seeking one entity to serve as a third-party administrator (TPA) for Medicaid reentry services available through the state’s approved Section 1115 Reentry Demonstration Initiative. The chosen TPA will work with various providers to support the clinical and social care needs of incarcerated enrollees, and help improve health outcomes, support case management, and stabilize enrollees’ health and wellness before release to reduce recidivism, emergency department visits, overdoses, and death. The contract will run from May 1, 2025 to June 30, 2026, with the option of three one-year extensions. Proposals are due January 23, 2025, and awardees will be announced in late February 2025.
National
Wakely Releases Analysis of Potential Election Impacts on the Individual Market. Wakely, an HMA Company, released in November 2024, a white paper on potential election impacts on the individual market, and specifically the Marketplace. The paper outlines numerous factors including legislation and operational changes since the Biden Administration took over, and key considerations and potential areas of change to keep in mind with the Trump Administration poised to retake control of Presidency.
CMS Announces Two Drug Manufacturers Participating in Cell and Gene Therapy Access Model. The Centers for Medicare & Medicaid Services (CMS) announced on December 4, 2024, that Bluebird Bio and Vertex Pharmaceuticals have entered into agreements with CMS to participate in the Cell and Gene Therapy Access Model. The voluntary model aims to improve health outcomes of people with sickle cell disease, increase access to cell and gene therapies, and lower healthcare costs. The outcome-based agreements will tie payments to health outcomes of patients using the medications. CMS will now engage with states participating in the Medicaid Drug Rebate program to see if they will participate in the model, which launches in January 2025.
CMS Finalizes Model to Increase Kidney Transplant Access For Individuals with ESRD. The Centers for Medicare & Medicaid Services (CMS) reported on November 26, 2024, that it has finalized a rule establishing a new mandatory six-year Increasing Organ Transplant Access (IOTA) Model, which aims to increase access to kidney transplants for all people living with end-stage renal disease (ESRD), launching July 1, 2025. CMS plans to select half of the donation service areas (DSAs) and all eligible kidney transplant hospitals in those DSAs to participate in the mandatory model. This final rule also adopts standard provisions that will apply to the Radiation Oncology Model, the ESRD Treatment Choices Model, and mandatory Innovation Center models whose first performance period begins on or after January 1, 2025.
President-elect Donald Trump Nominates Jim O’Neill as HHS Deputy Secretary. Politico reported on November 26, 2024, that President-elect Donald Trump nominated Jim O’Neill to be the Department of Health and Human Services (HHS) deputy secretary. O’Neill previously served as HHS principal associate deputy secretary during the George W. Bush administration.
Nearly 988,000 New Consumers Enroll in Health Insurance Marketplace for 2025. The Centers for Medicare & Medicaid Services (CMS) announced on December 4, 2024, that nearly 5.4 million individuals have enrolled in a health insurance Marketplace plan for 2025, including 4.4 million for the Healthcare.gov marketplace. Approximately 988,000 individuals are new Marketplace consumers for 2025, and 4.4 million are returning consumers. The Marketplace open enrollment period for HealthCare.gov ends January 15, 2025.
Medicaid, CHIP Enrollment Drops by 75,000 in August 2024, CMS Reports. The Centers for Medicare & Medicaid Services (CMS) reported on November 27, 2024, that enrollment in Medicaid and the Children’s Health Insurance Program (CHIP) was 79.4 million in August 2024, reflecting a decrease in enrollment of 75,307 from July 2024. Medicare enrollment was 67.8 million, up 132,500 from July 2024, including more than 34.2 million in Medicare Advantage plans. More than 8 million Medicare-Medicaid dual eligible individuals are counted in both programs.
Medicare Plans Pay Significantly Different Drug Prices Despite Using Same PBM. The Wall Street Journal reported on November 26, 2024, that Medicare plans paid significantly different prices for drugs even when the same pharmacy benefit manager (PBM) negotiated prices, according to an analysis by 46brooklyn Research. Prices are affected by factors such as what pharmacies charge Medicare for a drug and the facility where a patient is getting care. Approximately 61 drugs had monthly prices that diverged by at least $30,000, with commonly used generic versions of prostate-cancer treatment Zytiga having more than 2,200 prices in Medicare drug plans. Otezla had the largest price differences among branded medicines, with 633 different prices across health plans that used Express Scripts, while Optum Rx carried 569 different prices and Caremark had 431.
CMS Releases 200 New Medicare-funded GME Residency Slots to Hospitals. Modern Healthcare reported on November 22, 2024, that the Centers for Medicare & Medicaid Services (CMS) released 200 new graduate medical education (GME) residency slots, with about 70 percent of total slots set aside for either psychiatry or primary care. The slots, which go into effect in July 2025, include positions at 109 teaching hospitals across 33 states. Lawmakers allocated funding for a total of 1,200 new slots in the Consolidated Appropriations Act of 2021 and the CAA of 2023, and CMS has already distributed half of the new slots funded.
CMS Releases 2022 Medicaid LTSS User Trends and Expenditures Reports. The Centers for Medicare & Medicaid Services (CMS) released on November 21, 2024, several publications on Medicaid long-term services and supports (LTSS) user trends and expenditures for home and community-based services (HCBS) and institutional care in 2022. The reports found that 86.6 percent of LTSS users received HCBS and 64.6 percent of LTSS expenditures were for HCBS in 2022. CMS also found that 2.5 million HCBS users ages 0 to 20 accounted for $17 billion in spending, and approximately 100,000 institutional users ages 0 to 20 accounted for $3.5 billion in spending. State plan rehabilitative services were most common among HCBS users ages 0 to 20 and mental health facility services were the most common institutional service type.
CMS Issues Updated Provisions on Medicaid Coverage of Substance Use Disorder Treatment. The Centers for Medicare & Medicaid Services (CMS) issued on November 19, 2024, a State Medicaid Director Letter addressing updates to coverage requirements for substance use disorder (SUD) treatment made in 2024. The updates include making medications for opioid use disorder a permanent mandatory Medicaid benefit, and making permanent a state plan option to cover SUD and withdrawal management services provided to Medicaid beneficiaries ages 21 to 64 who have at least one SUD diagnosis and reside in an eligible Institution for Mental Diseases (IMD). The letter also highlighted an update to medical loss ratio remittances for expansion populations.
Industry News
UnitedHealthcare CEO Brian Thompson Fatally Shot Ahead of Investor Meeting. Modern Healthcare reported on December 4, 2024, that UnitedHealthcare chief executive Brian Thompson was fatally shot the morning of an annual investor conference. Thompson had been CEO since 2021. Previously, he served as CEO of the government programs division, overseeing the company’s Medicaid and Medicare plans. Thompson had been with United since 2004.
CMS Revises Centene, UnitedHealth Medicare Advantage Star Ratings. Modern Healthcare reported on December 2, 2024, that the Centers for Medicare & Medicaid Services (CMS) has revised and increased the Medicare Advantage star ratings for seven Centene contracts and 12 UnitedHealthcare contracts. In November, a U.S. District Court in Texas ordered CMS to redo UnitedHealthcare’s scores after the payer sued the agency over its use of secret shopper phone calls when calculating ratings. Centene and Humana filed similar lawsuits, which are both still pending.
Addus HomeCare Acquires Gentiva for $350 Million. Modern Healthcare reported on December 3, 2024, that Texas-based Addus HomeCare has finalized its $350 million acquisition of Gentiva’s home care business. Addus will gain 16,000 daily customers across Arizona, Arkansas, California, Missouri, North Carolina, Tennessee, and Texas through the acquisition.
Kaiser Permanente Subsidiary Risant Health Acquires Cone Health. Modern Healthcare reported on December 3, 2024, that Kaiser Permanente-owned Risant Health acquired North Carolina-based Cone Health. Cone Health will operate independently and maintain its name, and Risant has pledged a minimum investment of $1 billion to Cone over the next five years to support facility investments and other capital projects. Cone Health has four acute care hospitals and more than 150 outpatient sites in North Carolina.
CareSource Acquires Radiant Alliance. CareSource announced on November 26, 2024, that it has acquired Radiant Alliance for an undisclosed amount. Radiant Alliance—a nonprofit coalition of organizations focused on disease management, housing, and end of life care—includes Genacross Lutheran Services, Metta Healthcare, and United Church Homes.
Centene Cuts Certain Medicare Advantage Broker Commissions in New York, Washington. Modern Healthcare reported on November 25, 2024, that Centene will no longer compensate health insurance brokers for signing up enrollees to eight Medicare Advantage plans sold in New York and Washington. The company previously suspended commissions for all standalone Part D prescription drug plan sign-ups. CVS/Aetna, Cigna, and Elevance Health have also halted commissions for some Medicare plans.
Community Health Systems, WoodBridge Healthcare Abandon Hospital Sale. Modern Healthcare reported on November 26, 2024, that Community Health Systems has abandoned a $120 million deal to sell three Pennsylvania hospitals and related facilities to WoodBridge Healthcare. Community Health Systems and WoodBridge mutually decided to dissolve the agreement due to WoodBridge’s inability to satisfy funding requirements.
Community Health Systems to Sell ShorePoint Health System to AdventHealth. Modern Healthcare reported on November 22, 2024, that Community Health Systems signed a definitive agreement to sell Florida-based ShorePoint Health System to Florida-based AdventHealth for $265 million. The agreement includes ShorePoint Health Port Charlotte, certain assets of ShorePoint Health Punta Gorda, and ancillary businesses such as physician clinics, outpatient services and a freestanding emergency department. The deal is expected to close in the first quarter of 2025 and is subject to regulatory approvals.
RFP Calendar

HMA News & Events
HMA Podcasts
Has Medicare’s Drug Policy Struck the Right Balance Between Access and Cost? Kevin Kirby, managing director at Health Management Associates, gives a closer look at the evolution of Medicare’s drug coverage and the policies that have transformed patient access and affordability. From Clinton era ideas, to the launch of the Medicare Modernization Act and then the Affordable Care Act, Kevin has advised clients as these significant milestones have shaped and reshaped Medicare’s drug benefits. He discusses the implications of the Inflation Reduction Act, raising important questions about sustainability and cost control. The episode will explore how these pivotal policies will impact access to treatment and the sustainability of Medicare in a rapidly changing healthcare landscape. Listen Here
NEW THIS WEEK ON HMA INFORMATION SERVICES
(Exclusive Access for HMAIS Subscribers):
HMAIS Reports
- Updated HMAIS State Medicaid Agency Contracts (SMACs) Inventory
- Updated Florida State Overview
- Updated Hawaii State Overview
- Updated Michigan State Overview
- HMA Federal Health Policy Quick Takes
Medicaid Data
Medicaid Enrollment and Financials:
- District of Columbia Medicaid Managed Care Enrollment is Down 3.8%, Nov-24 Data
- MLRs Average 89.9% at Hawaii Medicaid MCOs, 2023 Data
- Indiana Medicaid Managed Care Enrollment Is Up 3.6%, Sep-24 Data
- Kentucky Medicaid Managed Care Enrollment is Down 7.3%, Nov-24 Data
- Louisiana Medicaid Managed Care Enrollment is Down 11.1%, Oct-24 Data
- Maryland Medicaid Managed Care Enrollment Is Down 7%, Oct-24 Data
- Michigan Medicaid Managed Care Enrollment is Down 12.8%, Sep-24 Data
- MLRs Average 85.1% at Michigan Medicaid MCOs, 2023 Data
- Missouri Medicaid Managed Care Enrollment is Down 10.8%, Sep-24 Data
- New Jersey Medicaid Managed Care Enrollment Is Down 14.8%, Sep-24 Data
- New Jersey Medicaid Fee for Service vs. Managed Care Penetration, 2014-23
- MLRs Average 85.1% at New Jersey Medicaid MCOs, 2023 Data
- MLRs Average 79.4% at Ohio Medicaid MCOs, 2023 Data
- MLRs Average 93.3% at Pennsylvania Medicaid MCOs , 2023 Data
- Rhode Island Medicaid Managed Care Enrollment is Down 9.6%, Sep-24 Data
- MLRs Average 82.4% at Tennessee Medicaid MCOs, 2023 Data
- Washington Medicaid Managed Care Enrollment is Down 4.8%, Sep-24 Data
- MLRs at West Virginia Medicaid MCOs Average 82.8%, 2023 Data
- West Virginia Medicaid Managed Care Enrollment is Down 7.3%, Aug-24 Data
Public Documents:
Medicaid RFPs, RFIs, and Contracts:
- Alaska MMIS Service Authorization Solution RFI, Nov-24
- Georgia Medicaid Care Management RFP, Awards, and Scoring, 2023-24
- Illinois Pharmacy Benefits Management System RFP and Contract, 2012-24
- Kentucky Medicare Advantage D-SNP Contracts, 2025
- Oregon MES System Integration RFI, Nov-24
- Oregon State-Based Marketplace Vendor RFP and Attachments, Nov-24
- Pennsylvania Children’s Health Insurance Plan (CHIP) RFA and Related Documents, 2024
- Pennsylvania Section 1115 Demonstration Keystones of Health HRSN Implementation Program Administrator RFI and Responses, 2024
- Washington Third-Party Administrator of Reentry Services RFP and Attachments, Nov-24
Medicaid Program Reports, Data, and Updates:
- Arizona AHCCCS Section 1115 Waiver Documents, 2020-24
- Florida Medicaid Managed Care Pre-Implementation Rate Certifications and Related Documents, SFY 2024-25
- Florida CHIP Annual Reports to CMS, 2017-23
- Maryland HealthChoice Evaluations, 2009-24
- Maryland HealthChoices 1115 Medicaid Waiver Documents, 2016-24
- North Dakota Medicaid Quality Strategy Draft, 2025-27
- Pennyslvania MLTSS Subcommittee Meeting Materials, Nov-24
- Texas HHS Ombudsman Annual Reports, 2023-24
- Utah Medicaid Reform 1115 Demonstration Waiver Documents, 2016-24
- Vermont EQRO Annual Technical Reports, 2015-24
- Wisconsin Medicaid HMO Quality Guides, 2023-25
- Wyoming Medicaid PMPM Expenditures and Utilization Reports, SFY 2015-23
A subscription to HMA Information Services puts a world of Medicaid information at your fingertips, dramatically simplifying market research for strategic planning in healthcare services. An HMAIS subscription includes:
- State-by-state overviews and analysis of latest data for enrollment, market share, financial performance, utilization metrics and RFPs
- Downloadable ready-to-use charts and graphs
- Excel data packages
- RFP calendar
If you’re interested in becoming an HMAIS subscriber, contact Andrea Maresca at [email protected].