On December 29, 2025, The Centers for Medicare & Medicaid Services (CMS) announced the highly anticipated funding awards to states for the Rural Health Transformation Program (RHTP)—a five-year, $50 billion federal initiative designed to stabilize and transform rural health systems across the country. This new federal investment marks a pivotal moment for states and their partners to address long-standing challenges in rural healthcare while laying the foundation for broader transformation. It provides an opportunity to reimagine care delivery, strengthen infrastructure, and build sustainable models that address entrenched gaps in rural health.
Directing Resources to Rural Communities
RHTP is designed with a focus on rural communities, where residents face persistent challenges such as provider shortages, hospital closures, and limited access to care. RHTP investments will support infrastructure development, IT system implementations and trainings, workforce recruitment and retention, and innovative care models tailored to rural community needs. The long-term goal is to create lasting capacity and resilience in rural health systems and promote better health outcomes for residents.
But the vision doesn’t stop there.
Catalyzing Statewide Transformation
While rural communities are the primary beneficiaries, we believe the impact of the RHTP will extend beyond rural borders. The program’s design encourages states to develop initiatives that can serve as pilots and start-ups, creating scalable solutions that can be adopted statewide. Workforce development programs, for example, may begin by focusing on rural providers and community health workers (CHWs) and training these individuals but, over time, strengthen the healthcare workforce across entire states and regions.
Much of the federal funding will enable states and their partners to invest in technology modernization, telehealth expansion, and integrated care models. These improvements assuredly will enhance access and quality for rural residents. And these same technologies can be deployed to enhance efficiency and coordination across entire health systems, laying the groundwork for broader system transformation and health improvement. The focus on chronic care management and innovative care arrangements has the potential to improve outcomes for all populations.
Collaborative Pathways for States and Partners
States and their partners—including health systems, community-based organizations, and technology innovators—have a valuable opportunity to collaborate on initiatives. In our review of state applications and the initial wave of state driven funding solicitations, we identified efforts to tackle long-standing system challenges, including:
Data Sharing and Interoperability. States responded to the federal application with extensive technology and data interoperability related investments that have statewide benefits. Several states include information system initiatives that can scale care coordination statewide, including initiatives to build dedicated teams for analytics, data integration, and evaluation and tracking outcomes across initiatives. They have an opportunity to create the statewide backbone—starting with rural hubs and then expanding interfaces systemwide. States also will be advancing consumer-facing technology for preventive and chronic care, grounded in statewide health information exchange (HIE) and data strategy, again testing first in rural settings and accelerating statewide adoption of effective approaches.
Maternal Health & Perinatal Care. Several states proposed embedding family medicine with obstetrics fellowships, expanding doula/midwife pathways, and deploying remote prenatal monitoring with support from nursing teams. These rural pilots could help standardize practice, improve outcomes, and scale across the state. Many other state proposals explicitly include initiatives to strengthen access to maternity care, linked to broader workforce and technology investments that can be adopted in urban settings.
EMS Modernization. States also plan to develop and strengthen emergency medical services (EMS)-led preventive and complex care support in rural areas. One application, for example, formalizes such EMS-led support in rural areas, with protocols and training designed to scale broadly. Another state references mobile health and EMS integration, creating rural pilots to improve response, navigation, and handoffs that can be standardized across the emergency care system.
Looking Ahead
RHTP is more than a funding stream. It is a catalyst for innovation and collaboration, providing an important avenue to address the chronic inequities in quality, access, and outcomes that people living in our nation’s rural communities often experience. But it also could foster improvement statewide. Program evaluation and performance monitoring of the small, community-based programs and the large-scale, multi-site, multi-year initiatives will provide insights that inform strategic decision-making at the local, state and federal levels. By scaling effective rural health-focused initiatives and investing in new and feasible tools, strategies, and programs, states can create models that improve care delivery for all their residents in the future. This is a moment for states, providers, and partners to think big and design programs that deliver lasting impact.
Health Management Associates (HMA) offers support to state agencies, health systems, and community partners shaping rural-first pilots that are designed for scalability—from maternal and perinatal care networks, EMS community care models, caregiver and CHW pipelines, to telehealth modernization and behavioral health integration. Our rural expertise and our unique ability to combine expertise in clinical, operational, policy, and data reforms for care improvement are well-suited to the goals of RHTP.
With the RHTP funding advancing to state partners early in 2026 and annual recalculations of state awards tied to performance, the time to design rural pilots that become statewide programs is now.
For questions about the RHTP opportunities for your organization and the solutions HMA can tailor to meet the needs of your state, contact Kathleen Nolan and Andrea Maresca.
Connecting the Dots: A new blog series for 2026
Connecting the Dots is a monthly HMA blog series that brings together insights from our experts to examine the major policy, program, and market forces shaping healthcare coverage, delivery systems, and financing in 2026. The posts look beyond individual changes, instead connect emerging developments across programs and markets to help leaders understand what’s changing, why it matters, and how their decisions shape the path ahead.
The Centers for Medicare & Medicaid Services (CMS) has officially opened the application window for the Rural Health Transformation Program (RHTP)—a $50 billion federal initiative designed to stabilize and transform rural health systems across the country. This one-time opportunity allows states to submit a comprehensive plan that could redefine how rural communities access care, manage chronic conditions, and sustain their healthcare infrastructure.
Applications must be signed by governors and submitted by November 5, 2025, and awards are expected by December 31, 2025, providing states with a very narrow window to act.
The remainder of this article explains key aspects of the RHTP application, including the evaluation and scoring aspects. Notably, the structure of the scoring system will reward states that are already aligned with these federal priorities, as well as those willing to implement new initiatives or make state policy changes to achieve alignment.
Program Overview and Funding Structure
Created under HR.1, the 2025 Budget Reconciliation Act, the RHTP allocates $10 billion annually from federal fiscal year (FY) 2026 to FY 2030, totaling $50 billion over five years. Funding is split into two tranches:
Tranche 1 (Baseline funding): $25 billion distributed evenly across all states with approved applications.
Tranche 2 (Workload funding): $25 billion distributed based on CMS scoring criteria, which include:
The percentage of the state population in rural census tracts
The proportion of rural health facilities in the state
The financial and operational status of hospitals
Other factors explained in the RHTP application notice
States must submit a single, one-time application that covers the full five-year period. Stand-alone provider applications will be declined. Hence, states must coordinate across agencies, providers, and stakeholders to develop a unified transformation strategy.
Importantly, this award is not a grant; rather, it is a cooperative funding agreement, which means CMS will play an active role in oversight and collaboration. States must be prepared to meet higher standards of accountability, transparency, and performance monitoring. According to the RHTP application, continued funding requires states to demonstrate satisfactory progress toward implementing their plan.
Application Requirements and Strategic Priorities
To be eligible for funding, states must submit a Rural Transformation Plan that addresses eight core priorities as follows:
Within these core priorities, state plans must propose activities that address several specific issues.
Technical Factor Weighting for Workload Funding Reflects Federal Policy Priorities
CMS outlines the eligibility criteria for baseline funding and the scoring components for workload funding. Baseline funds will be distributed equally among states, while workload funding will be based on each state’s rural facility and population score as well as their technical score. Evaluators will score technical factors based on state policy actions and initiative-based plans for each state.
The technical factors, and the weighting of these factors, in the RHTP application are not just neutral scoring mechanisms; rather, they are closely linked to the Trump Administration’s health policy priorities.
Weighting Structure: The RHTP funding is split evenly between baseline funding (50%) and workload funding (50%). Although baseline funding ensures all states receive support, the workload funding is directly tied to technical scores that reflect how well a state’s plan aligns with federal objectives and demonstrates readiness to implement transformative change that furthers federal objectives.
Scoring Criteria: Technical factors, such as rural population share, facility density, hospital financial status, scope of proposed activities, administrative capacity, stakeholder engagement, evaluation framework, and especially alignment with federal priorities, all contribute to the overall score. States that have already adopted or are willing to adopt federal policy priorities are positioned to score higher and receive more funding.
Annual Recalculation: CMS will recalculate each state’s technical score and workload funding annually to incentivize ongoing alignment with federal priorities and measurable progress toward transformation goals.
Alignment with Federal Priorities: One of the explicit scoring factors is “Alignment with Federal Priorities,” which measures the degree to which a state’s plan supports CMS goals for rural health transformation and sustainability. Under the Trump Administration, these priorities may include promoting value-based payment models, encouraging technology adoption, advancing adoption of Supplemental Nutrition Assistance Program (SNAP) food restriction waivers that prohibit the purchase of non-nutritious items, availability of integrated care plans for the Medicare-Medicare dually eligible population, reporting of full Medicaid T-MSIS data, and align policies with federal guidance on short-term limited duration insurance plans.
Preparing for What Happens Next: Implications for States, Providers, and Health Plans
The RHTP offers a rare opportunity to reshape rural healthcare. But success will require strategic coordination and a commitment to long-term change. States in the short and long term should consider include:
Identifying stakeholders who will be involved: Hospitals, rural health clinics, federally qualified health centers (FQHCs), behavioral health providers, and community organizations must be part of the planning process.
Reexamining priorities: States will need to reconcile competing needs across regions and provider types, balancing infrastructure investments with service delivery redesign.
Understanding infrastructure needs to support their project: Technology, workforce, and models of care must be strengthened to support long-term transformation.
Designing evaluation frameworks: States must include robust performance monitoring and reporting mechanisms to meet CMS expectations and secure future funding.
Providers and other stakeholders should also prepare to align with state strategies. Examples include:
Participating in regional partnerships
Adopting new care models and payment arrangements
Investing in technology and workforce development
Contributing data and insights to support evaluation efforts
The scoring structure also incentivizes states that may not yet be fully aligned to implement new initiatives or make policy changes that would improve their technical scores and secure greater funding. States and their partners will need to be united on the goals and initiatives, disciplined about implementing and evaluating the plans based on data informed reports, nimble and willing to make strategic pivots based on feedback and experiences.
Connect With Us
States that are already aligned with Trump Administration priorities—such as those with established value-based payment models, short-term limited duration plan options, preferred technology infrastructure, or strong rural hospital support policies—are positioned to be rewarded in the scoring and funding process.
Health Management Associates (HMA), is actively supporting states in developing compliant and compelling RHTP applications. Our advisory services include:
Strategic assessments and stakeholder engagement
Program design and grant writing
Implementation support and technical assistance
Actuarial support
Evaluation and performance monitoring
We help clients navigate the complexities of federal funding, align transformation goals with community needs, and build sustainable models for rural care delivery. For details about the RHTP, including the HMAIS State Action Tracker, contact HMA experts below.
Earlier this month colleagues from Health Management Associates (HMA) attended the 2025 Ohio Rural Health Association Conference. The gathering brought together providers, policymakers, and advocates from across the state to discuss one of the most pressing issues of our time: the future of rural health care in an uncertain policy and financial environment.
At a moment when federal funding and regulatory debates dominate the headlines, what stood out most was the energy and commitment among local leaders to work together on practical solutions. The challenges facing rural communities are profound—hospitals and clinics strained by reimbursement shortfalls, workforce shortages threatening access, and shifting payer dynamics creating new administrative burdens. Yet the conversations throughout the conference were grounded in resilience and collaboration, demonstrating that sustainable solutions begin at the community level.
Spotlight on Collaboration
HMA was honored to contribute to this dialogue through three sessions focused on core issues shaping rural care.
Kenneth Cochran, DSc, RN, FACHE, drew on his deep leadership experience as a former Ohio hospital CEO to highlight the urgency of workforce development. With projections of a 187,000-physician shortfall by 2037, Ken outlined integrated workforce strategies—apprenticeships, housing partnerships, and a culture of continuous learning—that can help stabilize rural hospitals and strengthen community health infrastructure.
Courtney Smith, RHIT, CCS, shared two critical perspectives. First, she unpacked the growing strain of Medicare Advantage in rural communities, where reimbursement often falls short and administrative requirements delay patient care. Second, she explored the complexities of Medicaid revenue cycle management, offering actionable steps rural providers can take—from leveraging technology and analytics to streamlining wrap-around payment reconciliation—to maintain stability in an unpredictable environment.
Jennifer Shaw, Senior Consultant, co-presented on best practices for navigating payer relationships with Courtney. She underscored how rural providers can use data to strengthen negotiations and how collaboration across hospitals, clinics, and associations creates the leverage necessary to ensure fair treatment in contracting and payment.
These discussions demonstrated the value of having clinical, operational, and policy perspectives at the table. Each HMA colleague brought not only technical expertise but also a deep appreciation for the lived realities of rural providers, ensuring our sessions were rooted in practicality.
A Landscape in Flux
The national policy context reinforces the importance of this work. Recent debates in Washington over rural health funding underscore just how fragile the financial footing of many hospitals and clinics can be. While the outcome of federal policy is uncertain, what is clear is that communities cannot afford to wait.
As HMA has noted in our broader work on rural health, effective solutions hinge on collaboration across sectors and levels of government. Whether it’s building workforce pipelines, ensuring fair payment, or streamlining operations, progress requires alignment among providers, payers, policymakers, and communities themselves.
Moving Forward
The Ohio Rural Health Association conference was a reminder that even in uncertain times, there is a powerful foundation for innovation and problem-solving when rural providers work together. HMA is proud to support these efforts, bringing decades of experience in Medicaid policy, health system transformation, and rural health strategy to bear for our partners.
As we look ahead, one lesson stands out: the path forward for rural health will not be written in Washington alone. It will be forged in places like Ohio, where providers, leaders, and communities are building practical, collaborative solutions every day.
Ohio Health Policy Snapshots
Sign up for Ohio Health Policy Snapshots delivered right to your inbox
This week’s In Focus section summarizes states’ Medicaid Section 1115 demonstration priorities over the last four years and highlights predicted changes coming with a new presidential administration. In the waning days of any presidency, regardless of party, reviewing and approving pending Section 1115 applications that reflect the current administration’s key policy initiatives is a priority for officials at the Centers for Medicare & Medicaid Services (CMS).
Each administration has discretion over which Section 1115 demonstrations to encourage and approve. Though specific Medicaid priorities under the upcoming Trump Administration are still nascent, Health Management Associates, Inc. (HMA), federal, and state experts are monitoring these developments. This article describes a subset of the signature initiatives the Biden Administration permitted states to pursue in their Medicaid Section 1115 demonstrations and how the new administration could focus on different priorities, rescind existing guidance, or potentially withdraw already approved waivers.
Overview of Biden-Era Section 1115 Demonstration Initiatives
CMS-approved Section 1115 demonstrations permit alternative methods to improve the accessibility, coverage, financing, and delivery of healthcare services under joint federal-state funded programs, specifically Medicaid and the Children’s Health Insurance Program (CHIP).
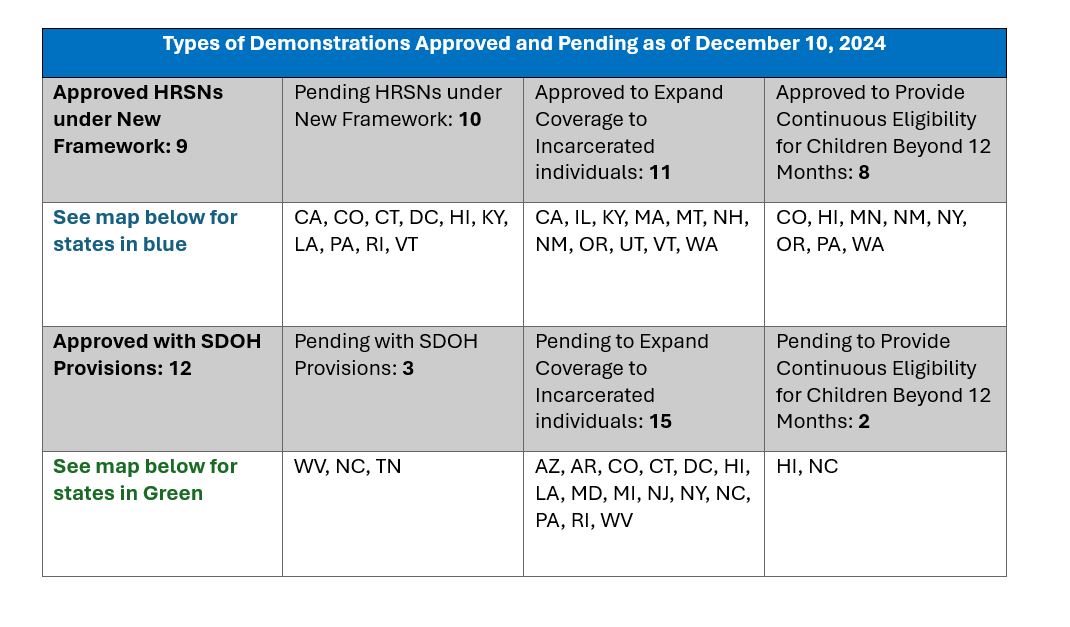
Addressing health disparities and promoting integrated care in Medicaid became a primary focus of the Biden Administration. In November 2023, CMS introduced a Medicaid and CHIP Health-Related Social Needs (HRSN) Framework, giving state Medicaid agencies the opportunity to address the broader social determinants of health (SDOH) that affect their enrollees, leading to better health outcomes. The new initiatives were not intended to replace other federal, state, and local social service programs, but rather to coordinate with those efforts. HRSN demonstration approvals to date include coverage of rent/temporary housing and utilities for up to six months and nutrition support (up to three meals per day), departing from longstanding prohibitions on payment of room and board in Medicaid.
During the present administration, CMS also has provided novel opportunities for states to adopt strategies that promote continuity of Medicaid coverage, mainly through bolstering Section 1115 demonstrations to provide multiyear continuous eligibility for children. In addition, CMS released guidance in April 2023 so states could apply for a new Section 1115 demonstration opportunity to test transition-related strategies that support community reentry for incarcerated people who would otherwise be eligible for Medicaid or CHIP.
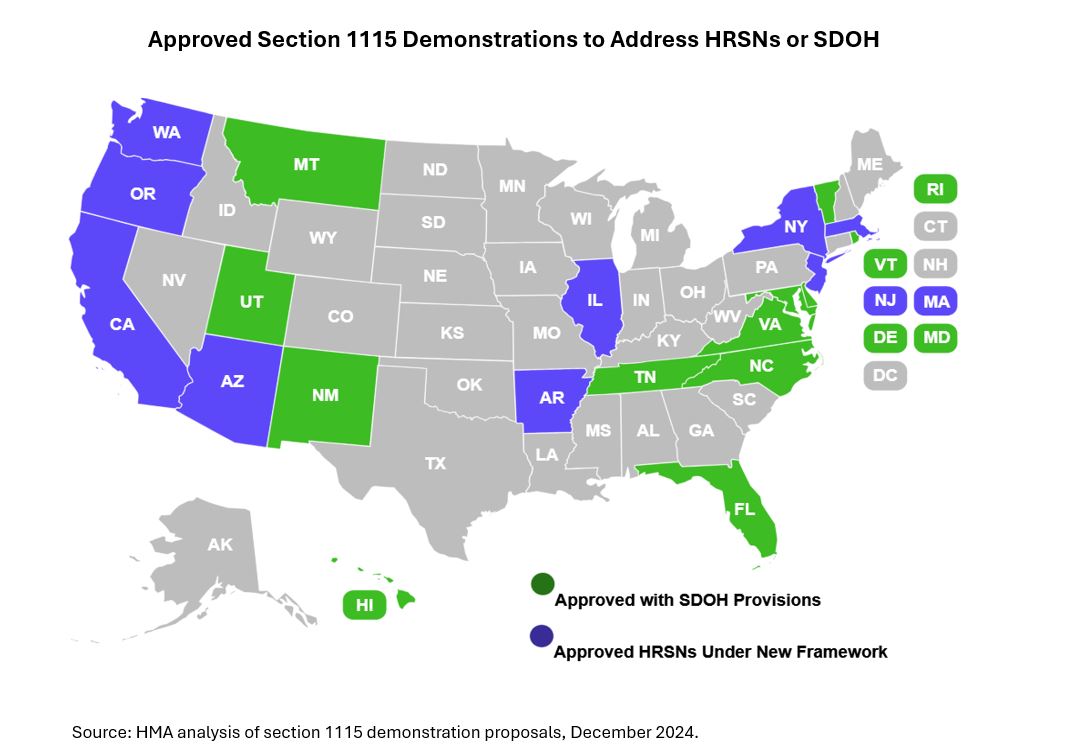
The table and map below show the types of demonstrations approved and pending to date. We anticipate that incoming administration officials will closely examine the four demonstration initiatives outlined as they determine their own Medicaid policy agenda and priorities. Under President Biden’s Administration, nine states received federal approval for HRSN demonstrations under the new framework. Another 10 states have applications pending.
Rescissions and renewals. Incoming Trump Administration officials technically could attempt to rescind some of the Section 1115 demonstrations approved during the Biden Administration. The Biden Administration unsuccessfully pursued with, a similar strategy for certain 1115 demonstration components approved during President-Elect Trump’s first term. Like the Biden Administration, the incoming Trump officials may choose not to renew demonstrations, even if the courts prevent them from rescinding approvals.
Any signature Section 1115 policy is unlikely to emerge until the new administration’s policy officials are in place. There are, however, important insights to consider based on the first Trump Administration’s priorities and areas of common ground across the Biden and first Trump administrations.
Signature 1115 initiatives. During President Trump’s first term, one signature Medicaid Section 1115 initiative allowed states to apply work requirements to some eligibility groups. CMS officials at that time also approved capped allotments for certain components of a state’s Medicaid program. Some states might consider revisiting these options with incoming administration officials. Two other key policy areas to watch following the transition include:
The first Trump Administration approved a pilot program to test interventions addressing HRSNs in North Carolina’s Medicaid 1115 demonstration program. Though the approved HRSNs were less expansive than the HRSN 1115 interventions later announced by the Biden Administration, this could be an area of common ground where the policy evolves and can be incorporated into discussions on other nascent initiatives.
Multiple administrations, including the first Trump Administration, have prioritized Medicaid policies and demonstration initiatives to address substance use disorders (SUD) and, separately, reentry. The intersection of these issues can provide another area of common ground and opportunity to continue work on state reentry initiatives, though likely with new and modified parameters.
Implementation Considerations
Federal approval of Medicaid Section 1115 demonstration proposals is a critical milestone for states. Demonstration implementation also requires significant and ongoing leadership, resources, and collaboration between states and CMS and states and their partners.
The type of state demonstration activity is expected to shift dramatically over the course of the new administration. For example, proposals may shift from expansions in coverage and benefits to reflect the new administration’s other priorities. States, too, may consider alternative approaches to Section 1115 demonstrations, such as state plan authorities like in lieu of services (ILOS), to pursue certain innovative approaches that they might otherwise have implemented with demonstration authority.
Connect with Us
HMA empowers states, providers, and other stakeholders to thrive in an ever-changing healthcare landscape. With deep expertise at every level, HMA teams support state Medicaid programs and stakeholder partners nationally to address a range of operational challenges, including designing innovative healthcare approaches to address urgent healthcare challenges, expanding coverage opportunities, and optimizing integration to address program efficiencies and improved “whole person” care.
We have expertise in all of the components critical to developing Section 1115 programs—from the policy knowledge, to actuarial/budgeting talent, to communications and project management skills, as well as the necessary IT infrastructure.
Contact our featured experts below to learn more about HMA’s capabilities and expertise.
This week, our In Focus section provides an initial overview of recent US Supreme Court rulings that reshape the landscape of national healthcare policy and operations. These decisions, ranging from redefining federal agency powers to addressing local ordinances that will affect people who are unhoused, are poised to have far-reaching implications across the federal and state governments.
The Decisions
A significant ruling came on June 29, 2024, with the Court overturning the precedent established in the 1984 Chevron v. Natural Resources Defense Council ruling. This year’s decision in LoperBright Enterprises v. Raimondo marks a pivotal shift by eliminating the deference traditionally granted to federal agencies’ interpretations of ambiguous statutes. By empowering courts to clarify vague legislation, the ruling raises fundamental questions about the future of existing regulations and may lead to a surge in litigation challenging federal agency interpretations. The Court did state this ruling would have no impact on past decisions regarding the Chevron doctrine. The decision would apply only to current, pending, and future cases. When read in conjunction with the “major questions doctrine” announced in 2022 in West Virginia v. Environmental Protection Administration, agencies now face more challenges to regulations under a legal structure that does not provide deference to the agency.
In a separate ruling that garnered attention, the Supreme Court upheld local ordinances in Grants Pass, OR, that restrict individuals experiencing homelessness from using blankets, pillows, or cardboard boxes for shelter in public spaces. The majority opinion in City of Grants Pass, Oregon v. Johnson supported the city’s stance that these ordinances, aimed at prohibiting camping on public property, do not constitute cruel and unusual punishment under the Constitution. This decision has sparked considerable debate over the balance between municipal governance and constitutional protections for people who are unhoused.
Also portending effects for the healthcare industry is the Court’s decision that defendants facing civil monetary penalties from the US Securities and Exchange Commission have a right to a jury trial. The Securities and Exchange Commission v. Jarkesy decision presents new considerations for healthcare and life sciences companies facing civil monetary penalties from the US Department of Health and Human Services.
What’s Next
The implications of these rulings are poised to reverberate throughout both federal and state governments. Stakeholders across healthcare and beyond must prepare for a period of adjustment and adaptation. Numerous questions regarding implementation and enforcement will likely emerge. The outcomes could trigger a wave of legal challenges and legislative responses as stakeholders navigate the evolving regulatory landscape.
Future In Focus sections will dive deeper into the potential impacts these decisions will have on healthcare policies and partnerships with related sectors. These insights will be pivotal in guiding strategic decisions amid the evolving legal framework.
A public health crisis is growing more acute in rural America, disproportionately impacting individuals with both Medicaid and Medicare (the “dually eligible”). Dually eligible individuals residing in rural areas represent about 5 percent of all rural residents. They reside at the intersection of a public health crisis and a fragmented Medicaid and Medicare care delivery system. As HMA wrote in Health Affairs, this small population is at risk of falling through the cracks of this crisis and suffering a steep rural mortality penalty.
With support from Arnold Ventures, HMA prepared “The Health Equity & Access for Rural Dually Eligible Individuals (HEARD) Toolkit: Raising Rural Voices from New Mexico, North Dakota, and Tennessee to Create Action. The toolkit contains eight actionable solutions for federal and state policymakers to use and tailor to states’ needs. Ellen Breslin, Samantha Di Paola, and Susan McGeehan authored the toolkit, with research contributions from Rebecca Kellenberg and Andrea Maresca.
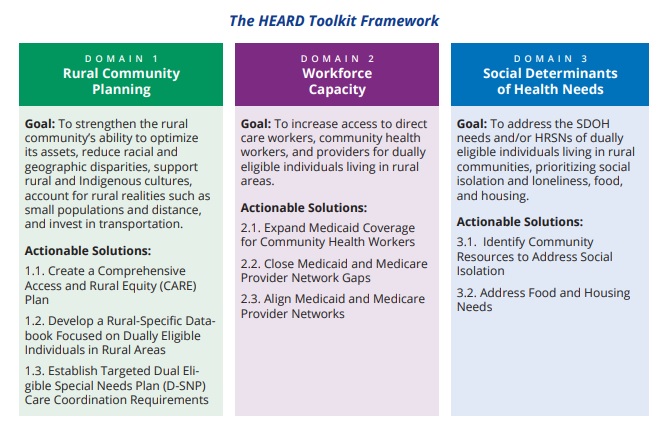
In 2022, HMA convened stakeholder roundtables in three states – including New Mexico, North Dakota, and Tennessee to identify the challenges facing dually eligible individuals living in rural areas and to propose solutions to these challenges. Informed by this process, HMA developed the Health Equity & Access for Rural Dually Eligible Individuals (HEARD) Toolkit.
The toolkit is structured around three domains used to organize eight solutions. For each solution, HMA provides a description of the rural access challenge, the proposed solution, and the proposed tool. Each tool is powered by some type of lever available to the federal and state government. We anticipate that policymakers will build upon this toolkit through continued dialogue with rural communities. The toolkit’s framework, goals, and actionable solutions are summarized in the figure below.
HMA Principal Ellen Breslin, Consultant Samantha Di Paola, and Senior Consultant Susan McGeehan authored the toolkit, with research contributions from HMA Principals Rebecca Kellenberg and Andrea Maresca. Download the toolkit.
On February 2, 2023, HMA will hosted a webinar on the HEARD toolkit. During this webinar, HMA experts and panelists including Dr. Kevin Bennett (USC-SOM Columbia, SC CRPH), Dennis Heaphy (DPC), Pam Parker (SNP Alliance), and Tallie Tolen (New Mexico Medicaid) will summarized and discussed the toolkit’s actionable solutions for improving rural dually eligible individuals’ health and social outcomes.
This week, our In Focus section highlights the Health Affairs article, Advancing Health Equity and Integrated Care for Rural Dual Eligibles, authored by Ellen Breslin, Samantha Di Paola, Susan McGeehan, Rebecca Kellenberg, and Andrea Maresca, Health Management Associates.
A public health crisis is growing more acute in rural America, disproportionately impacting individuals with both Medicaid and Medicare (the “dually eligible”). The rural health crisis is a health equity concern that affects all rural residents, including dually eligible individuals. There are 47 to 60 million people residing in rural areas. Twenty-one percent of dually eligible individuals live in rural areas—that’s about 2.6 million people. Based on these numbers, the authors calculate that the dual eligible population residing in rural communities accounts for about 5 percent of the total rural population. Dually eligible individuals living in rural areas are at risk of falling through the cracks.
Dually eligible individuals lack access to adequate medical, behavioral health, home-and community-based services (HCBS) and other social services; those living in rural areas face even steeper challenges. Since dually eligible individuals are among the poorest of all individuals covered under Medicare, they are at significant risk of paying a steep rural mortality penalty.
With these challenges there are opportunities for innovation for the dually eligible population living in rural communities. The US can reverse the mortality-disparity rate trajectory. Public and private entities are interested in revitalizing rural America, confronting the rural health crisis, and harnessing the power of rural communities. Investment in the rural health care sector is essential given it is a major economic driver of rural communities.
HMA is creating a toolkit with actionable solutions to improve access to services and integrated care and health equity for individuals dually eligible for Medicare and Medicaid who live in rural areas across the country. This project is a follow-on project to a previous HMA project supported by Arnold Ventures. In 2021, HMA prepared a brief, Medicare-Medicaid Integration: Essential Elements for Integrated Care Programs for Dually Eligible Individuals, to increase and promote enrollment in integrated care programs (ICPs) meeting dually eligible individuals’ needs and preferences. Interviewees including dually eligible individuals helped HMA to identify “access to needed services in rural areas” as an essential element of ICPs. In response, HMA started a new project to create a toolkit with actionable strategies to improve access to needed services and improve integrated care opportunities, specific to dually eligible rural residents’ needs.
HMA designed the toolkit around four values: 1) rural health equity is an imperative for dually eligible individuals, 2) actionable solutions and innovations must come from the community, 3) there is no single pathway to integration, and 4) Medicare and Medicaid flexibilities are critical to inspiring innovations to advance health equity, access, and integration. The toolkit will provide actionable solutions for states with and without integrated care programs for dually eligible individuals to increase access to needed supports and services, care coordination, and integrated care programs. We expect that states and rural communities will use the toolkit as a foundation for mapping a holistic plan to advance access to care coordination and integrated programs for dually eligible individuals residing in rural communities. Other states may employ contractual tools listed in the toolkit to expand access to providers and new services; strengthen partnerships among entities serving the community such as community-based organizations, providers, and health plans; and increase community-wide accountability for meeting dually eligible individuals’ whole person-centered needs. The toolkit is scheduled for an early 2023 release.
Today’s blog is the next in our series highlighting significant developments in the Medicare program. In our first article we covered the Centers for Medicare and Medicaid Services’ (CMS) calendar year 2023 Medicare Physician Fee Schedule (MPFS) proposed rule. This week we are highlighting a few key policy developments in the proposed rule that governs payment levels and policy updates for hospital outpatient departments and ambulatory surgical centers (ASCs).
As we discussed last week, this is a pivotal moment for the Biden Administration’s Medicare policy agenda. Because the rulemaking cycle takes about 18 months, CMS needs to begin the process of collecting input on new proposals this year if it intends to finalize proposals before the end of the President’s first term. Additionally, the CY2023 rule represents an important transition year for CMS as it navigates the COVID-19 related anomalies in the data used to calculate payment levels.
Health care plans, providers, and facilities are continuing to transition to value based payment strategies, making it increasingly important to assess the entire environment of Medicare payment rules as these payment systems are the basis of financial benchmarks, quality incentives, and other key components of value-based payments. In addition, these payment rules provide insight into the cost pressures, incentives, and areas of misalignment throughout the health care system.
HMA experts are analyzing and closely tracking several issues in the CY 2023 hospital outpatient prospective payment system (OPPS) proposed rule. A brief summary of some of the most important proposed policy changes for the outpatient hospital setting are included below and highlight many of the Administration’s top health care priorities.
Policies to sustain access and address health disparities in rural communities.
Enhancing Medicare’s behavioral health payment and access policies beyond the COVID-19 public health emergency.
Uncertainty in the hospital outpatient prospective payment system (OPPS) rate increase due to future implementation of changes in 340B payment.
Increasing transparency of consolidation and mergers in the marketplace to help advance quality and affordability.
The remainder of our post delves into these issues and other notable proposals. Our post also includes analysis of the implications of these policies for stakeholders deserving.
Key Action Items for Stakeholders
The CY 2023 OPPS Proposed Rule was published on July 15, 2022, and all comments from stakeholders are due to CMS by September 13, 2022. We anticipate CMS will release their Final Rule in late fall 2022, before the new rules are implemented January 1, 2023.
The public comment period is also an important window of opportunity during which stakeholders can analyze the impact of CMS’s proposed policies, assess the proposals against other applicable pending federal and state payment policies, and consider how the proposals may impact business decisions. Further, the public comment period is essential for CMS to deepen its understanding of the impact of its policies on stakeholders. The agency benefits from hearing stakeholder’s perspectives, viewing their quantitative and legal analyses, and understanding the general stakeholder environment.
Rural Emergency Hospitals: Definition and Payment
The Consolidated Appropriations Act of 2021 (CAA) established a new provider type called Rural Emergency Hospitals (REHs) beginning in 2023. REHs are facilities that convert from either a critical access hospital (CAH) or a rural hospital with less than 50 beds, by choosing to close their inpatient capacity. Instead, these facilities provide emergency department services, outpatient services, post-hospital extended care services, and other defined services.
While the statute specifies many foundational aspects of REHs, CMS was given the authority to further define REH eligibility status and to specify the unique reimbursement mechanisms for REHs. All of these components will be vital to a provider or entity’s decision to pursue REH status.
On June 30, CMS released the first component: Conditions of Participation (CoPs) for REHs, which defined REH status within the Medicare program. Within the CY 2023 OPPS Proposed Rule CMS proposed to define reimbursement and several other key components of REHs. Below we detail the key elements of REH reimbursement. In HMA’s blog next week we will offer greater detail on the COP and reimbursement policies.
REH policies proposed in the CY 2023 OPPS Proposed Rule:
REHs will receive a monthly facility payment of approximately $268,000 (or more than $3 million per year) beginning in CY 2023.
REHs will receive a 5 percent payment increase for all services covered under the Medicare OPPS.
REHs may provide outpatient services that are not otherwise paid under the OPPS (e.g., the Clinical Lab Fee Schedule) as well as post-hospital extended care services furnished in a unit of the facility that is a distinct part of the facility licensed as a skilled nursing facility (SNF).
Beneficiaries served at REHs will not be charged a copayment on the additional 5 percent OPPS payments, but standard OPPS cost-sharing requirements would still apply.
REHs must comply with all applicable provider enrollment provisions in order to enroll in Medicare.
REHs will have a unique quality reporting program distinct to REHs, in order to reduce reporting burden on these smaller facilities. CMS seeks feedback from stakeholders on the measures used for the REH quality reporting program.
REHs will be provided an exception from the Physician Self-Referral Law (commonly known as the “Stark Law”).
Takeaway: The creation of REHs is both a significant change for the Medicare program and potentially a unique opportunity for small rural hospitals and health systems which own/operate rural hospitals. The Congress and CMS believe this model will address access to care concerns and health disparities present in rural communities. Many assert that under the REH approach, hospitals and health system providers serving rural communities may have greater flexibility to support the rural communities they serve.
Look for our additional analysis of the set of proposed REH policies next week.
Mental Health Services Furnished Remotely by Hospital Staff
For CY 2023, CMS proposes several updates to its remote services policy to plan for a transition from temporary policies enacted during the PHE to when the PHE is declared over. CMS proposes to:
Allow clinical staff of a hospital to conduct remote mental health and substance abuse services and to designate these services as hospital outpatient department services for purposes of reimbursement. Patients will be permitted to be in the homes and hospital clinical staff must conduct the service from inside the hospital facility. Further, CMS proposes new hospital outpatient codes for these services, and CMS will not permit these outpatient services to be conducted (and billed) in tandem with physician fee schedule services.
The agency will require an in-person service within 6 months prior to the initiation of the remote service and then every 12 months thereafter. CMS will allow exceptions to the in-person visit requirement based on beneficiary circumstances.
The agency is also proposing that audio-only interactive telecommunications systems may be used to furnish these services when the beneficiary is not capable of, or does not consent to, the use of two-way, audio/video technology.
Takeaway: As CMS wrote in the proposed rule, many beneficiaries may be receiving mental health services in their homes from hospital or critical access hospital staff during the COVID-19 PHE. The policy update could help minimize disruptions in continuity of care that might otherwise occur following the end of the PHE. The proposals also reflect CMS’ desire to adapt to changing beneficiary preferences and new methods of providing services that have evolved during the COVID-19 PHE.
Hospitals and health systems may benefit from these proposals because it will maintain and expand patient-provider access points and care coordination after the patient has left the hospital. Stakeholders will need to continue to assess beneficiary utilization of services furnished remotely, potential staffing changes to support these services, and community-specific access needs for remote mental health services. Stakeholders may have important perspectives to offer CMS through the regulatory comment proceed as the agency determines whether to finalize a requirement that hospital clinical staff be physically located in the hospital when furnishing services remotely using communications technology.
Payment Policies
CMS is proposing to update OPPS payment rates for hospitals and ASCs that meet their respective applicable quality reporting requirements by 2.7 percent. This update reflects the following factors:
Projected hospital market basket percentage increase of 3.1 percent; and
A 0.4 percentage point reduction for projected multifactor productivity.
In the context of the OPPS, CMS proposes to increase the OPPS conversation factor by 2.7 percent from CY 2022 to CY 2023, from $84.18 to $86.79. CMS estimates this will increase OPPS payments to providers from CY 2022 to CY 2023 by $1.8 billion.
In the context of ASCs, CMS estimates a proposed increase to the ASC conversation factor by 2.7 percent from CY 2022 to CY 2023, from $49.91 to $51.31. CMS estimates this change will increase industry-wide payments from CY 2022 to CY 2023 by $130 million. In addition, CY 2023 is the final year in which CMS will apply the productivity-adjusted hospital market basket update to ASC payment system rates for an interim period of 5 years (CY 2019 through CY 2023).
Consistent with CMS’s methods for updating other Medicare prospective payment systems during the 2023 regulatory cycle, the agency proposes to use claims data from CY 2021 and hospital cost report data from the June 2020 Healthcare Cost Report Information System (HCRIS) to update payment rates for CY 2023. Some stakeholders have expressed concern during this regulatory cycle that claims data continue to include anomalous trends influenced by covid cases and the cost data do not accurately reflect covid-related costs because the data primarily are associated with pre-COVID time period.
340B Payment Policy
CMS’s proposed rule acknowledges the recent Supreme Court decision in American Hospital Association v. Becerra (No. 20-1114, 2022 WL 2135490), which will have a significant impact on the 340B program. However, given the recency of this decision the agency formally proposed to maintain the current payment rate of Average Sale Price (ASP) minus 22.5 percent for drugs and biologics acquired through the 340B program.
In response to the decision, CMS stated that the agency will adjust 340B payment rates within the CY 2023 final rule. In its recent ruling, the Supreme Court held that HHS may not vary payment rates for drugs and biologicals among groups of hospitals without having surveyed hospitals’ acquisition costs. The decision relates to payment rates for CYs 2018 and 2019 but has implications for the CY 2023 rates.
CMS also stated that it anticipates applying a 340B payment rate of ASP plus 6 percent for specified drugs and biologics in the CY 2023 final rule. This would likely result in a budget neutrality reduction approaching 5% in the OPPS conversion factor.
Takeaway: Hospitals and federally qualified health centers (FQHCs) receiving 340B reimbursements will view the court ruling and potential increase to 340B payment rates as positive. However, it remains unclear at what exact level 340B payments will be set. Therefore, stakeholders may want to comment on the CY2023 policy options CMS is considering. Additionally, stakeholders should plan for CMS to conduct a survey of acquisition costs as it considers newly proposing changes to the payment rates. It remains possible that CMS will continue to apply the 340B cut for 2023 in light of a 2020 survey of hospital acquisition cost that it conducted. Future budget neutrality adjustments may also be necessary for any payments that are returned to hospitals due to the overturning of the 340B cut for 2018 and 2019.
Additional Issues for Stakeholder Consideration
In addition to the financing and policy issues discussed above, the wide-ranging rule contains numerous other policy proposals with direct and indirect implications on Medicare providers, beneficiaries, and other stakeholders. Table 1 provides a snapshot of some of the issues that warrant further consideration.
Table 1. Other Notable Proposed Changes Impacting Health Care Providers and Stakeholders
Topic
Summary
Provider Transparency
CMS issues a request for information linked to the President’s July 2021 Executive Order (E.O.) on Promoting Competition in the American Economy. CMS currently manages a database of nursing homeowners and operators, and the agency has begun to leverage that data to support hospital and nursing home patients and their families. The agency solicits feedback on whether it should release additional data that is already being collected “to help identify the impact of provider mergers, acquisitions, consolidations, and changes in ownership on the affordability and availability of medical care.” CMS also invites comments on whether the agency should release similar data for other types of providers. The solicitation represents the next phase in CMS’ expansive portfolio of work to address the impact of market consolidation on health care prices, consumer costs, and quality in the healthcare industry writ large. Medicare providers and stakeholders should be tracking how federal health care regulators, including CMS, are working to respond to the E.O. There is a strong likelihood that CMS will begin to include data on other types of providers and stakeholders will need to understand this shifting landscape and how it could impact their current and potential future business decisions.
SaaS
CMS discusses its desire to address the novel and evolving nature of Software as a medical Service (Saas) procedures. The agency is seeking comments on the specific payment approach we might use for these services under the OPPS as SaaS-type technology becomes more widespread. We are also concerned about the potential for bias in algorithms and predictive modeling, and are seeking comments on how we could encourage software developers to prevent or mitigate the possibility of bias in new applications of this technology.
Inpatient Only List
Removes ten services from the Inpatient Only (IPO) list.While the IPO list has previously been targeted for major reforms, this year’s narrower set of proposed changes signal CMS’ is deprioritizing IPO list reform.
Payment for surgical N95 Respirators
CMS recognizes that hospitals may incur additional costs when purchasing domestic NIOSH-approved surgical N95 respirators. CMS is proposing payment adjustments under the IPPS and OPPS that would reflect, and offset, the additional marginal resource costs that hospitals face in procuring domestically made NIOSH-approved surgical N95 respirators. Under this proposal, these payments would be provided biweekly as interim lump-sum payments to the hospital and would be reconciled at cost report settlement. The rule outlines the information providers need to include on the cost report to determine payments for cost reporting periods beginning on or after January 1, 2023.
Ambulatory Surgery Centers
CMS requests stakeholder feedback on methods that could be implemented to collect cost data from ASCs that minimize reporting burden.This could be the beginning of a process to implement cost reports for ASCs.
The HMA Medicare team will continue to analyze these proposed changes. We have the depth and breadth of expertise to assist with tailored analysis, to model policy impacts, and to support the drafting of comment letters to this rule.
On June 30, 2022, the Centers for Medicare & Medicaid Services (CMS) released a proposed regulation establishing the Conditions of Participation (CoPs) for a new hospital provider type, Rural Emergency Hospitals (REHs). The REH concept was first developed by the Medicare Payment Advisory Commission (MedPAC) and subsequently mandated by Congress through the Consolidated Appropriations Act (CAA) of 2021 to address the growing concern over closures of rural hospitals.
REHs provide an opportunity for Critical Access Hospitals (CAHs) and rural hospitals to improve the way care is delivered in their communities, maintain access, and avert potential closure by choosing to focus on the service offerings that are most essential to their communities, such as emergency services, observation care, and additional medical, behavioral, and maternal outpatient services. Importantly, the REH concept enables facilities to maintain a hospital designation absent inpatient capacity thereby ensuring that rural communities retain access to services. This proposed regulation is a significant milestone in CMS’ work to implement the REH designation and their novel payment methodology by their mandated start date of January 1, 2023.
The REH concept is expected to help address the observed health inequities that arise when rural communities lack access to hospitals and other providers. Obtaining an REH designation could be an opportunity for many independent hospitals and delivery systems to strategically reshape themselves in line with their community’s needs while receiving payments from Medicare for doing so.
Within CMS’ proposed regulation, the agency proposes to establish a novel set of REH CoPs which will define the parameters of the REH designation. The REH CoPs closely align with the current CAH CoPs in most cases, while considering the uniqueness of REHs and the statutory requirements. In some instances, the proposed REH policies closely align to the current hospital and ambulatory surgical center standards, such as the polices for outpatient services’ requirements and life safety code, respectively.
As a part of this proposed regulation, CMS seeks input from the rural community on a few key aspects of the REH designation, including:
The specific proposed REH standards, including the ability of an REH to provide low-risk childbirth-related labor and delivery services and whether the agency should require REHs to provide outpatient surgical services in the event that surgical labor and delivery intervention is necessary.
Whether it is appropriate for an REH to allow a physician, physician associate, nurse practitioner, or clinical nurse specialist, with training or experience in emergency medicine, to be on call and immediately available by telephone or radio contact and available on site within specified timeframes.
Updates to CoPs for Critical Access Hospitals
Also within this draft regulation CMS proposes to update the CoPs for CAHs by: (1) adding a definition of primary roads to the location and distance requirements; (2) establishing a patient’s rights CoP; and (3) allowing CAHs that are a part of a larger health system (containing other hospitals and/or CAHs) to unify and integrate their infection control and prevention and antibiotic stewardship programs, medical staff, and quality assessment and performance improvement programs (known as QAPI) to ensure consistent and safe care.
What’s Next
CMS is accepting comments on this rule until August 29, 2022. CMS intends to propose additional policies related to Medicare enrollment, payment, and quality reporting in the upcoming Calendar Year 2023 Outpatient Prospective Payment System/Ambulatory Surgery Center proposed rule. CMS will develop final policies for this program later this year.
For more information about this proposed regulation including how to submit comments and how the REH concept may impact the hospital industry and patients in rural communities please contact our Medicare team who have knowledge in Congressional, MedPAC and CMS policy and operations featured below.