This week, our In Focus section reviews highlights and shares key takeaways from the 21st annual Medicaid Budget Survey conducted by The Kaiser Family Foundation (KFF) and Health Management Associates (HMA). Survey results were released on October 27, 2021, in two new reports: States Respond to COVID-19 Challenges but Also Take Advantage of New Opportunities to Address Long-Standing Issues: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2021 and 2022 and Medicaid Enrollment & Spending Growth: FY 2021 & 2022. The report was prepared by Kathleen Gifford, Aimee Lashbrook, and Sarah Barth from HMA; Mike Nardone; and by Elizabeth Hinton, Madeline Guth, Lina Stolyar, and Robin Rudowitz from the Kaiser Family Foundation. The survey was conducted in collaboration with the National Association of Medicaid Directors (NAMD).
This survey reports on trends in Medicaid spending, enrollment, and policy for FY 2021 and FY 2022, highlighting state experiences with policies adopted in response to the COVID-19 pandemic. The conclusions are based on information provided by the nation’s state Medicaid Directors.
Key Report Highlights
In the following sections, we highlight a few of the major findings from the reports. This is a fraction of what is covered in the 50-state survey reports, which include significant detail and findings on policy changes and initiatives related to eligibility and enrollment, delivery systems, benefits/telehealth, social determinants of health, provider rates/taxes, and pharmacy. The reports also look at the key issues and challenges now facing Medicaid programs.
Medicaid Enrollment and Spending Growth
The COVID-19 pandemic created significant implications for Medicaid. During this time, the primary drivers of Medicaid enrollment and spending trends have been due to the Families First Coronavirus Response Act (FFCRA), enacted in March 2020, which authorized a 6.2 percentage point increase in the federal match rate, or Federal Medical Assistance Percentage (FMAP), retroactive to January 1, 2020, and until the Public Health Emergency (PHE) ends. The increase was available to states that meet certain “maintenance of eligibility” (MOE) requirements.
Medicaid enrollment increased sharply in FY 2021 (10.3 percent) due to the MOE requirements and the pandemic’s economic effects. Responding states expect Medicaid enrollment growth to slow to 4.5 percent in FY 2022, based largely on the assumption that the PHE and the related FFCRA MOE requirements will end in FY 2022 (most states assume mid-way through FY 2022). Since the survey, the PHE was extended to mid-January 2022, which would affect these projections and possibly delay anticipated effects of slowing enrollment and spending currently assumed in state budgets for FY 2022. However, states also identified challenges to resuming normal eligibility operations such as the need for system changes, staffing shortages, and the volume of new applications and redeterminations.
In FY 2021, total Medicaid spending increased to a peak of 11.4 percent. This was primarily due to enrollment growth, as half of states reported pandemic-related utilization decreases for non-COVID care. State Medicaid spending growth increased to 4 percent. In FY 2022, most states expect a full rebound in acute care services utilization. State budgets for FY 2022 expect total Medicaid spending growth to slow to 7.3 percent. Over a third of states expect enrollment to become a downward pressure in FY 2022, assuming that the MOE requirements end midway through FY 2022. Regardless of when the PHE ends, most states will start to prepare for the eventual unwinding of their MOE policies and procedures, as resuming Medicaid eligibility renewals will be a large administrative task for states. Guidance from CMS gives states 12 months to complete renewals and redeterminations following the end of the PHE. State Medicaid spending growth is expected to increase to 14 percent in FY 2022.
Figure 1 – Percent Change in Medicaid Spending and Enrollment, 1998-2022
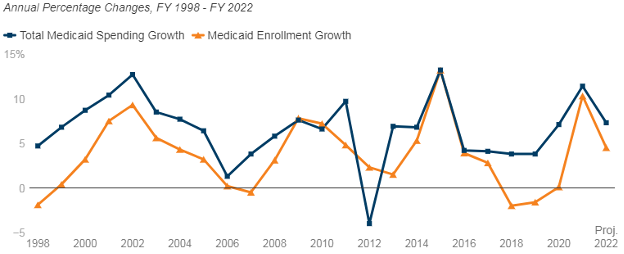
SOURCE: FY 2021-2022 spending data and FY 2022 enrollment data are derived from the KFF survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, October 2021. Historic data reflects growth across all 50 states and DC and comes from various sources.
Delivery Systems
Figure 2 – MCO Managed Care Penetration Rates for Select Groups of Medicaid Beneficiaries as of July 1, 2021
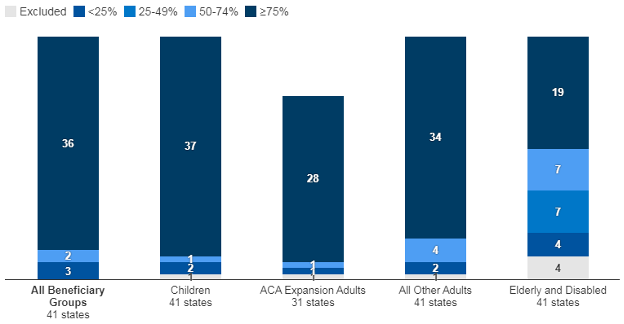
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
Medicaid Managed Care Changes
Benefits and Telehealth
- During the COVID-19 pandemic, most states used Medicaid emergency authorities to temporarily adopt new benefits, adjust existing benefits, and/or waive prior authorization requirements. Some states indicated plans to permanently extend these emergency benefit changes past the public health emergency (PHE) period.
- Excluding temporary changes adopted via emergency authorities in response to the COVID-19 pandemic but including any emergency changes that have or will become permanent, 22 states reported new or enhanced benefits in FY 2021, and 29 states are adding or enhancing benefits in FY 2022. Three states reported benefit cuts or limitations in FY 2021 and two states reported benefit cuts or limitations in FY 2022.
Figure 3 – Select Categories of Benefit Enhancements or Additions
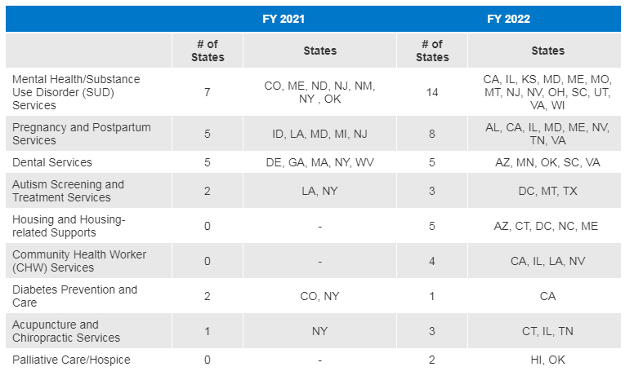
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- Nearly all responding states reported covering a range of fee-for-service (FFS) services delivered via audio-visual telehealth, with slightly fewer states reporting audio-only coverage for each service. Thirty-three states with MCOs (out of 36 responding) report requiring MCOs to cover the same services via telehealth as covered in FFS; one MCO state indicated requiring MCOs to cover the same services “in part.”All responding states ensure payment parity between telehealth and in-person delivery of FFS services, and most states require MCOs to maintain these same payment parity policies.
- Thirty-one states (out of 45 responding) reported that telehealth had particular value in maintaining or improving access to behavioral health services.
- Post-pandemic telehealth coverage and reimbursement policies are under consideration in most states, with states weighing expanded access against quality concerns especially for audio-only telehealth. Key factors include evaluation of telehealth access, utilization, and outcomes; quality assurances and clinical appropriateness; coordination with policies in other states, from other payers, and at the federal level; and costs of expanded telehealth.
- Commonly reported challenges associated with telehealth include access to internet and technology, as well as needs for education/outreach and quality assurances.
Social Determinants of Health
- The vast majority of responding states that contract with MCOs (33 of 37) reported leveraging MCO contracts to promote strategies to address the social determinants of health in FY 2021. More than half of responding MCO states reported the following requirements were in place in FY 2021: screening enrollees for behavioral health needs, providing referrals to social services, partnering with community-based organizations (CBOs), and screening enrollees for social needs.
Figure 4 – State MCO Contract Requirements Related to Social Determinants of Health, FYs 2021 – 2022
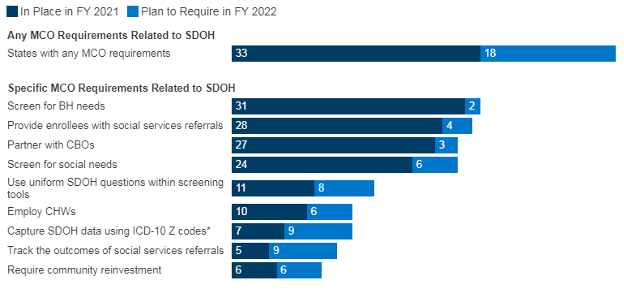
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- States also reported efforts to expand the number Community Health Workers (CHWs), address disparities in health care by race and ethnicity in Medicaid, and a variety of MCO activities aimed at promoting the take-up of COVID-19 vaccination.
Provider Rates and Taxes
Figure 5 – FFS Provider Rate Changes Implemented in FY 2021 and Adopted for FY 2022
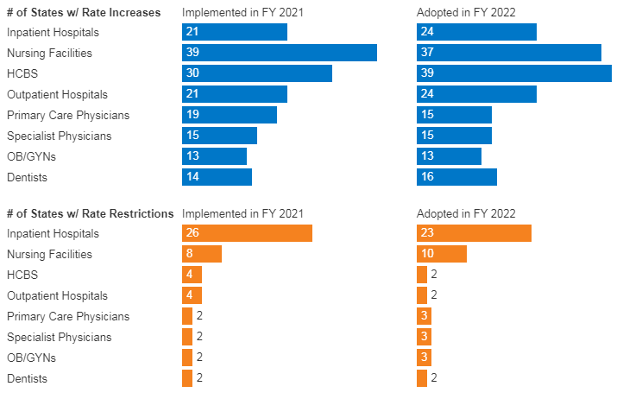
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- More than half of states that contract with MCOs always require MCOs to pay remittances when minimum medical loss ratio (MLR) requirements are not met.
- Twenty-one states reported that they always require MCOs to pay remittances, while nine indicated they sometimes require MCOs to pay remittances.
Figure 6 – Medicaid MCO Minimum Medical Loss Ratio (MLR) Remittance Requirements
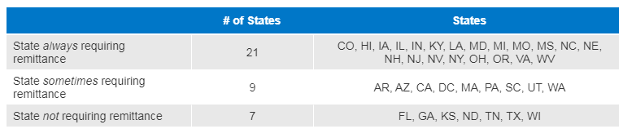
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- Twenty-one states reported imposing risk corridors in their MCO contracts for all or part of FY 2020 or FY 2021 in response to the COVID-19 pandemic.
Figure 7 – States Imposing MCO Risk Corridors in FY 2020 and/or FY 2021 in Response to the COVID-19 Pandemic
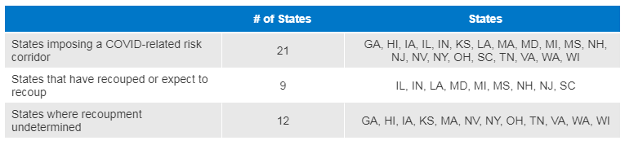
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- In FY 2021, more than one-third of responding MCO states (13 of 37) implemented new provider payment and/or pass-through requirements on MCOs in response to the COVID-19 emergency.
- Thirty-four states reported having three or more provider taxes in place in FY 2021.
- The most common Medicaid provider taxes in place in FY 2021 were taxes on nursing facilities (45 states), followed by taxes on hospitals (44 states), intermediate care facilities for individuals with intellectual disabilities (33 states) and MCOs (17 states).
- Four states reported plans to add new taxes in FY 2022. Only one state, Maryland, reported plans to eliminate a tax in FY 2022.
- Eleven states reported planned increases to one or more provider taxes in FY 2022, while two states reported planned decreases.
Pharmacy
- Most states that contract with MCOs report that the pharmacy benefit is carved into managed care (35 out of 41 states that contract with MCOs). Five states (Missouri, North Dakota, Tennessee, Wisconsin, and West Virginia) report that pharmacy benefits are carved out of MCO contracts as of July 1, 2021. Three states report plans to carve out pharmacy from MCO contracts in state FY 2022 or later (California, New York, and Ohio).
- In FY 2022, Kentucky began contracting with a single PBM for the managed care population.
- Louisiana reports that it will require MCOs to contract with a single PBM designated by the state in FY 2022.
- Thirty of the 37 responding states that contract with MCOs report adoption of at least one financial risk mitigation strategy in MCO contracts. Drug carve-outs and risk corridors (global and pharmacy-only) are the most common risk mitigation strategies reported.
Figure 8 – Risk Mitigation Strategies Used in MCO Pharmacy Contracts as of July 1, 2021
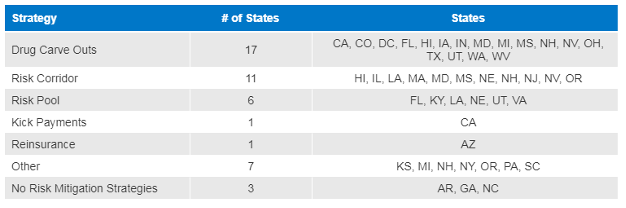
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2021.
- Specialty and high-cost drugs remain the biggest cost driver of pharmacy spending growth in most states. A majority of states reported newly implementing or expanding upon at least one initiative to contain costs in the area of prescription drugs in both FY 2021 and FY 2022.
Key Priorities and Challenges in FY 2022 and Beyond
When asked to identify the top priorities, issues, and challenges for FY 2022 and beyond, Medicaid directors listed the following:
- The unwinding of PHE emergency measures, especially the need to complete eligibility redeterminations within federally prescribed timelines.
- Promoting health equity.
- Focusing on non-emergency initiatives, especially efforts to better align payment with quality, improve health outcomes, and implement information technology (IT) systems.
Some states have also indicated that lessons learned from the pandemic are opportunities, including for improved relationships with providers and expanded access for enrollees. The evaluation of PHE-related utilization data, including telehealth utilization, could inform efforts to sustain and expand access post-pandemic. States identified ongoing efforts to advance delivery system reforms and to address health disparities and social determinants of health as areas of promise to build on in the future.
