Implementation of Medications for Opioid Use Disorder (MOUD) and Medication Assisted Treatment (MAT) Programs in County Justice Systems and State Departments of Correction
CONTEXT: THE PROBLEM
A significant percentage of individuals in American jails and prisons have a substance use disorder (SUD), with those with opioid use disorder (OUD) at especially high risk of death due to overdose upon release from incarceration.1 At the same time, overdose deaths during incarceration continue to increase.2,3
Medications for opioid use disorder (MOUD) and medication assisted treatment (MAT) programs reduce in-jail overdose death by 50% and the risk of overdose death after release by 60%. MAT programs also redress substantial racial and ethnic health disparities4. Despite these proven benefits, most incarcerated Americans do not have access to this treatment. Barriers to MAT implementation include lack of resources such as money, trained staff, and leadership; stigma toward both SUD and MOUD; and limited system ability to support adaptive change.
KEY MODEL ELEMENTS AND PROMISING RESULTS
Health Management Associates (HMA), a national research and consulting firm focusing on publicly funded healthcare, developed a MAT implementation support model working with dozens of jails and prisons across the United States, rapidly scaling access to MOUD/MAT during incarceration. This implementation support model fosters both technical and adaptive change using a learning collaborative structure and adult-learning theory. The model also acknowledges the unique environment of each jail and prison and the challenges of providing healthcare services for a complex condition like OUD in a correctional setting. This model program is straightforward, documented, proven, and readily replicated.
The model provides participating jail and prisons teams with access to robust individualized technical assistance and coaching; peer-to-peer support and learning; training; and collaborative educational sessions. This approach recognizes that multidisciplinary teams inclusive of custody/security staff; medical personnel; behavioral health providers; and others must be convened and supported as a cohesive unit to effectively implement MOUD and MAT programs in jails, prisons, and the justice and addiction ecosystems. This ecosystem view incorporates the critical partners and pathways outside the jail and prison to support effective re-entry to the community following incarceration to support recovery. A change management and continuous quality improvement framework is foundational to the model.
In the California, Illinois and Michigan county jail team learning collaboratives, county teams receive implementation grants or stipends. Over the course of the projects these amounts have ranged from $15,000 to over $100,000 per county, which were included in the project budget from the funding source (State Opioid Response in CA and IL; state general funds in CA). Offering this “seed money” serves as an incentive to help counties engage in the learning collaborative. HMA has managed all aspects of these implementation grants/stipends.
Evaluation
Collection and analysis of data informs ongoing technical assistance and demonstrates the rapid scaling and positive impact of the program. In the state learning collaborative programs, deidentified data is collected from county jail teams and analyzed and compiled to reflect trends and progress in the implementation effort. Where HMA supports state departments of correction with MOUD and MAT implementation, HMA assists the prison system with identifying and using key data points to inform a continuous quality improvement process.
Funding
The MOUD and MAT county jail implementation model was initiated in 2018 in California’s MAT in Jails and Drug Courts program with demonstrated impact for expanding access to MAT in the state’s county jails. The project was funded with federal State Opioid Response dollars administered by the California Department of Health Care Services (DHCS) through September 2022. The California legislature approved state general funds to support continuation of the program from October 2022 through June 2025.
Illinois’ Department of Health Services Substance Use Prevention and Recovery (SUPR) sponsored implementation of that state’s learning collaborative beginning in 2021 with federal State Opioid Response Dollars. It is currently funded through June 2024 with plans to extend the learning collaborative under a new SOR funding cycle.
Michigan Department of Health and Human Services elected to implement the county jail learning collaborative in late 2023, funding it with state opioid settlement funds for continuation through November 2026.
HealthCare Access Maryland in support of the Maryland Governor’s Office of Crime Prevention, Youth, and Victim Services deployed this model for a limited three-month period with HMA to increase access to MOUD for incarcerated persons. The impetus for this project was the OUD Examinations and Treatment Act, which requires local jails/jurisdictions in Maryland to offer all forms of MOUD.
Michigan Department of Corrections has engaged HMA for years as its contracted third-party health care evaluator. HMA supported the DOC’s MAT implementation across multiple sites in the Michigan prison system with state general funds from 2020-2022.
HMA supported the Alaska Department of Corrections with widescale MAT implementation under a contract through state general funds 2022-2023.
RESULTS
HMA’s successful model incorporates strategies that overcome typical barriers to MOUD/MAT implementation in corrections settings.
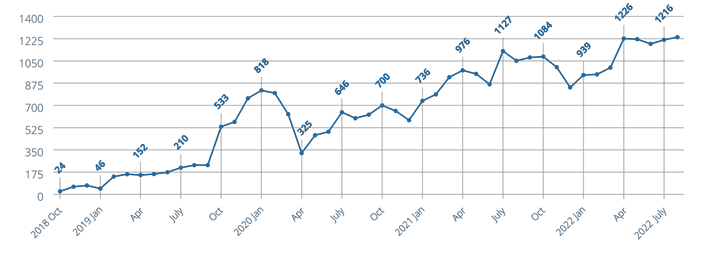
In the California learning collaborative, HMA has engaged 41 county jails over four years resulting in 35,000 person-months5 of individuals on MAT with counties participating representing almost 90 percent of the state’s total population.
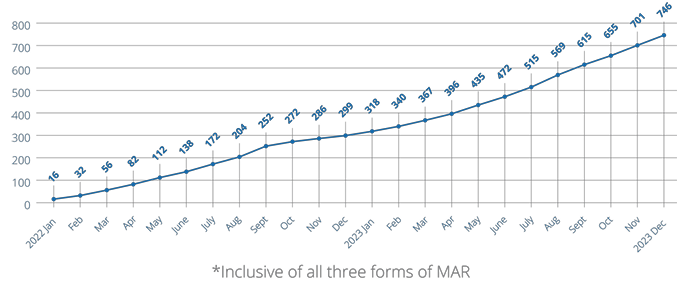
In the Illinois learning collaborative, HMA has engaged 28 counties over three years resulting in over 720 unique individuals receiving MAT in jails with participating counties representing 64 percent of the state’s population (Cook County is excluded because of an evolved MAT program prior to inception of Illinois’ county learning collaborative).
Figure 1. Running total of unique individuals who have received MAR in Jail in Illinois from inception of data collection from counties through December 2023. (MAR is medication assisted recovery – the term used for medication assisted treatment in Illinois.)
Figure 2. Running total of person-months individuals who have received MAT in jail in California participating jails from program inception through August 2022
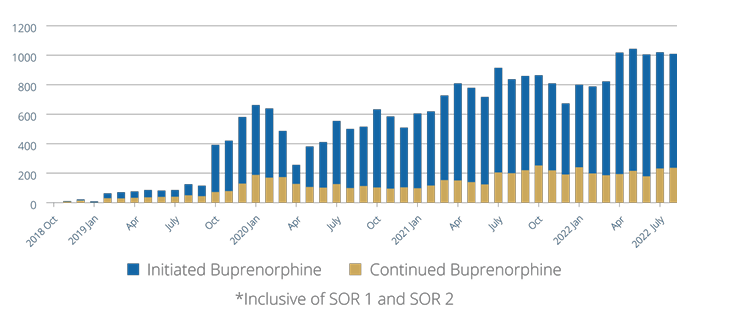
Figure 3. Running total of person-months individuals were initiated or continued on buprenorphine in California participating jails from program inception through August 2022
STRATEGY/APPROACH/INTERVENTIONS
HMA coaches and subject matter experts (SMEs) understand and respond to the unique regulatory oversight, policies, and procedures in jail and prison operations, requiring customized approaches to introduce and expand MOUD and MAT access. Both adaptive and technical change strategies are deployed to assist jails and prisons in changing their culture and operations to treat SUD like other chronic, treatable diseases. HMA coaches and SMEs stay deeply involved with implementation teams to initiate and support change over time.
County jail teams in the learning collaborative and DOC site teams are assigned an HMA coach who understands and supports their individualized operations, resource capacity, and goals. The coach convenes an in person-team meeting and initial facility walk-through to jump start the initiative and inform ongoing team implementation goals and activities. The coach assists the team in establishing and executing goals and action steps that align with the overarching goals of the learning collaborative or DOC system.
All county teams are regularly convened for collaborative learning sessions to support their implementation plan on an ongoing basis. These sessions include fundamental information on MAT/MOUD and related components of evidencebased SUD treatment in corrections settings. Coaches identify challenges and barriers at their sites and these themes inform sessions at additional learning collaborative convenings. These identified themes are also targeted with training and hands-on coaching support (e.g., biases against MAT among providers and custody staff; custody concerns about diversion of medications; payment mechanisms for the medications; and sufficient staff capacity to offer the treatment).
Critical elements of the change effort include:
Improved SUD screening, assessment, treatment options, and planning to include at least two forms of MAT are core themes and goals of the learning collaborative. This messaging and expectation accelerate implementation by “setting a bar” for teams’ efforts while providing them with individualized assistance to overcome challenges in meeting their goals.
Engagement across the treatment ecosystem including advisors from state associations of counties, sheriff departments, treatment providers, and the state prison system connects the counties with emerging policy and best practices from their professional peers.
Multidisciplinary teams: MAT in jails and drug courts requires an integrated approach inclusive of medical and behavioral health care staff, custody/security and other justice professionals, and county providers and leadership.
This implementation model drives rapid, systemic change that would likely not be possible with individual site efforts. Scaling is accelerated by the learning collaborative model in which barriers that are identified by multiple county or DOC site teams, such as regulations for methadone access to incarcerated individuals or practice of a healthcare vendor serving multiple sites, are addressed at the levels of state policy or corporate leadership and addressed in group learning opportunities.
Lessons Learned
The approach needs to be tailored to each jail and county – and for departments of correction, each DOC site – who have resources, concerns, and goals unique to them. For example, a DOC reception center will have different security and programming requirements and workflows than a general detention center. A rural county with an average daily population of 15 and intermittent nursing and provider access has different resources than a suburban jail with an average daily population of 500. The technical assistance must incorporate this understanding and meet each site where they are to be effective.
The aim – improved SUD treatment systemwide including transitions when individuals enter the corrections system and again at release – needs to be addressed as a countywide problem that needs a comprehensive ecosystem solution. Or, in the cases of departments of corrections, system and statewide perspective and strategies are required.
Implementation of MAT in jails should be sponsored by the sheriff, and key partners from probation, jail custody, jail healthcare, drug courts, local county drug treatment programs, and the county administrator’s office must be included in planning and implementation. Implementation of MAT in departments of corrections must be endorsed and actively supported by the highest levels of leadership in the system and at each prison location.
Do not underestimate the prevalence and impact of stigma. There is an ongoing need for broader education about substance use disorders and treatment including about MAT and MOUD. All stakeholders and those impacted by opioid use disorder need to understand that substance use disorder is a chronic brain-based disease and that MAT/MOUD is effective treatment – not use of a substance that is problematic, i.e. “MAT is just replacing a drug with another drug.”
It is important to build supportable, sustainable implementation plans. If teams are not given sufficient support and opportunity to evolve in their understanding and development of the implementation program they may fail. At the same time a sense of urgency is important because people are dying due to lack of access to needed treatment.
ABOUT HMA
HMA is a leading independent research and consulting firm with more than 500 consultants with expertise across all domains of publicly funded healthcare and human services. HMA has distinguished itself from other consulting companies with our decades-long tradition of hiring senior-level policymakers, healthcare system leaders, and other experts with hands-on experience.
1 National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services.
5 “Person-months” is defined as the number of persons receiving MAT (any of the three forms of MOUD) in the reporting month, per jail, aggregated.
CONTEXT: THE PROBLEM
A significant percentage of individuals in American jails and prisons have a substance use disorder (SUD), with those with opioid use disorder (OUD) at especially high risk of death due to overdose upon release from incarceration.1 At the same time, overdose deaths during incarceration continue to increase.2,3
Medications for opioid use disorder (MOUD) and medication assisted treatment (MAT) programs reduce in-jail overdose death by 50% and the risk of overdose death after release by 60%. MAT programs also redress substantial racial and ethnic health disparities4. Despite these proven benefits, most incarcerated Americans do not have access to this treatment. Barriers to MAT implementation include lack of resources such as money, trained staff, and leadership; stigma toward both SUD and MOUD; and limited system ability to support adaptive change.
KEY MODEL ELEMENTS AND PROMISING RESULTS
Health Management Associates (HMA), a national research and consulting firm focusing on publicly funded healthcare, developed a MAT implementation support model working with dozens of jails and prisons across the United States, rapidly scaling access to MOUD/MAT during incarceration. This implementation support model fosters both technical and adaptive change using a learning collaborative structure and adult-learning theory. The model also acknowledges the unique environment of each jail and prison and the challenges of providing healthcare services for a complex condition like OUD in a correctional setting. This model program is straightforward, documented, proven, and readily replicated.
The model provides participating jail and prisons teams with access to robust individualized technical assistance and coaching; peer-to-peer support and learning; training; and collaborative educational sessions. This approach recognizes that multidisciplinary teams inclusive of custody/security staff; medical personnel; behavioral health providers; and others must be convened and supported as a cohesive unit to effectively implement MOUD and MAT programs in jails, prisons, and the justice and addiction ecosystems. This ecosystem view incorporates the critical partners and pathways outside the jail and prison to support effective re-entry to the community following incarceration to support recovery. A change management and continuous quality improvement framework is foundational to the model.
In the California, Illinois and Michigan county jail team learning collaboratives, county teams receive implementation grants or stipends. Over the course of the projects these amounts have ranged from $15,000 to over $100,000 per county, which were included in the project budget from the funding source (State Opioid Response in CA and IL; state general funds in CA). Offering this “seed money” serves as an incentive to help counties engage in the learning collaborative. HMA has managed all aspects of these implementation grants/stipends.
Evaluation
Collection and analysis of data informs ongoing technical assistance and demonstrates the rapid scaling and positive impact of the program. In the state learning collaborative programs, deidentified data is collected from county jail teams and analyzed and compiled to reflect trends and progress in the implementation effort. Where HMA supports state departments of correction with MOUD and MAT implementation, HMA assists the prison system with identifying and using key data points to inform a continuous quality improvement process.
Funding
The MOUD and MAT county jail implementation model was initiated in 2018 in California’s MAT in Jails and Drug Courts program with demonstrated impact for expanding access to MAT in the state’s county jails. The project was funded with federal State Opioid Response dollars administered by the California Department of Health Care Services (DHCS) through September 2022. The California legislature approved state general funds to support continuation of the program from October 2022 through June 2025.
Illinois’ Department of Health Services Substance Use Prevention and Recovery (SUPR) sponsored implementation of that state’s learning collaborative beginning in 2021 with federal State Opioid Response Dollars. It is currently funded through June 2024 with plans to extend the learning collaborative under a new SOR funding cycle.
Michigan Department of Health and Human Services elected to implement the county jail learning collaborative in late 2023, funding it with state opioid settlement funds for continuation through November 2026.
HealthCare Access Maryland in support of the Maryland Governor’s Office of Crime Prevention, Youth, and Victim Services deployed this model for a limited three-month period with HMA to increase access to MOUD for incarcerated persons. The impetus for this project was the OUD Examinations and Treatment Act, which requires local jails/jurisdictions in Maryland to offer all forms of MOUD.
Michigan Department of Corrections has engaged HMA for years as its contracted third-party health care evaluator. HMA supported the DOC’s MAT implementation across multiple sites in the Michigan prison system with state general funds from 2020-2022.
HMA supported the Alaska Department of Corrections with widescale MAT implementation under a contract through state general funds 2022-2023.
RESULTS
HMA’s successful model incorporates strategies that overcome typical barriers to MOUD/MAT implementation in corrections settings.
In the California learning collaborative, HMA has engaged 41 county jails over four years resulting in 35,000 person-months5 of individuals on MAT with counties participating representing almost 90 percent of the state’s total population.
In the Illinois learning collaborative, HMA has engaged 28 counties over three years resulting in over 720 unique individuals receiving MAT in jails with participating counties representing 64 percent of the state’s population (Cook County is excluded because of an evolved MAT program prior to inception of Illinois’ county learning collaborative).
Figure 1. Running total of unique individuals who have received MAR in Jail in Illinois from inception of data collection from counties through December 2023. (MAR is medication assisted recovery – the term used for medication assisted treatment in Illinois.)
Figure 2. Running total of person-months individuals who have received MAT in jail in California participating jails from program inception through August 2022
Figure 3. Running total of person-months individuals were initiated or continued on buprenorphine in California participating jails from program inception through August 2022
STRATEGY/APPROACH/INTERVENTIONS
HMA coaches and subject matter experts (SMEs) understand and respond to the unique regulatory oversight, policies, and procedures in jail and prison operations, requiring customized approaches to introduce and expand MOUD and MAT access. Both adaptive and technical change strategies are deployed to assist jails and prisons in changing their culture and operations to treat SUD like other chronic, treatable diseases. HMA coaches and SMEs stay deeply involved with implementation teams to initiate and support change over time.
County jail teams in the learning collaborative and DOC site teams are assigned an HMA coach who understands and supports their individualized operations, resource capacity, and goals. The coach convenes an in person-team meeting and initial facility walk-through to jump start the initiative and inform ongoing team implementation goals and activities. The coach assists the team in establishing and executing goals and action steps that align with the overarching goals of the learning collaborative or DOC system.
All county teams are regularly convened for collaborative learning sessions to support their implementation plan on an ongoing basis. These sessions include fundamental information on MAT/MOUD and related components of evidencebased SUD treatment in corrections settings. Coaches identify challenges and barriers at their sites and these themes inform sessions at additional learning collaborative convenings. These identified themes are also targeted with training and hands-on coaching support (e.g., biases against MAT among providers and custody staff; custody concerns about diversion of medications; payment mechanisms for the medications; and sufficient staff capacity to offer the treatment).
Critical elements of the change effort include:
Improved SUD screening, assessment, treatment options, and planning to include at least two forms of MAT are core themes and goals of the learning collaborative. This messaging and expectation accelerate implementation by “setting a bar” for teams’ efforts while providing them with individualized assistance to overcome challenges in meeting their goals.
Engagement across the treatment ecosystem including advisors from state associations of counties, sheriff departments, treatment providers, and the state prison system connects the counties with emerging policy and best practices from their professional peers.
Multidisciplinary teams: MAT in jails and drug courts requires an integrated approach inclusive of medical and behavioral health care staff, custody/security and other justice professionals, and county providers and leadership.
This implementation model drives rapid, systemic change that would likely not be possible with individual site efforts. Scaling is accelerated by the learning collaborative model in which barriers that are identified by multiple county or DOC site teams, such as regulations for methadone access to incarcerated individuals or practice of a healthcare vendor serving multiple sites, are addressed at the levels of state policy or corporate leadership and addressed in group learning opportunities.
Lessons Learned
The approach needs to be tailored to each jail and county – and for departments of correction, each DOC site – who have resources, concerns, and goals unique to them. For example, a DOC reception center will have different security and programming requirements and workflows than a general detention center. A rural county with an average daily population of 15 and intermittent nursing and provider access has different resources than a suburban jail with an average daily population of 500. The technical assistance must incorporate this understanding and meet each site where they are to be effective.
The aim – improved SUD treatment systemwide including transitions when individuals enter the corrections system and again at release – needs to be addressed as a countywide problem that needs a comprehensive ecosystem solution. Or, in the cases of departments of corrections, system and statewide perspective and strategies are required.
Implementation of MAT in jails should be sponsored by the sheriff, and key partners from probation, jail custody, jail healthcare, drug courts, local county drug treatment programs, and the county administrator’s office must be included in planning and implementation. Implementation of MAT in departments of corrections must be endorsed and actively supported by the highest levels of leadership in the system and at each prison location.
Do not underestimate the prevalence and impact of stigma. There is an ongoing need for broader education about substance use disorders and treatment including about MAT and MOUD. All stakeholders and those impacted by opioid use disorder need to understand that substance use disorder is a chronic brain-based disease and that MAT/MOUD is effective treatment – not use of a substance that is problematic, i.e. “MAT is just replacing a drug with another drug.”
It is important to build supportable, sustainable implementation plans. If teams are not given sufficient support and opportunity to evolve in their understanding and development of the implementation program they may fail. At the same time a sense of urgency is important because people are dying due to lack of access to needed treatment.
ABOUT HMA
HMA is a leading independent research and consulting firm with more than 500 consultants with expertise across all domains of publicly funded healthcare and human services. HMA has distinguished itself from other consulting companies with our decades-long tradition of hiring senior-level policymakers, healthcare system leaders, and other experts with hands-on experience.
1 National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services.