1300 Results found.

Digital innovation to be a featured topic at 2023 HMA fall conference
Advancements in digital health and data technology have made for rapid and remarkable transformation of the healthcare landscape. From wearable devices to mobile health apps to telemedicine platforms, the integration of digital solutions and patient data is disrupting every facet of healthcare – to say nothing of the AI revolution that has only just begun. While this innovation is exciting and meaningful, it still has runway to truly deliver “better, cheaper, faster” for patients. These innovations and others will be featured at Health Management Associates annual fall conference, being held October 30-31, 2023.
Digital innovation has graduated from its “experimentation/compliance” phase and is now in its “expectation of results” phase. Healthcare payers and providers should incorporate digital into core payment and delivery strategies to deliver better outcomes and a better care experience at a most efficient cost. Health data management is creating more efficient platforms to provide the right care at the right time to the right patient. Federal policy programs like the 21st Century Cures Act, and CMS Interoperability and Patient Access rule have opened the door for providers, payers, and applications to make better use of health information, with patients more in control.
While this level of innovation is exciting anywhere, it is particularly exciting to see how it is enabling improvements in publicly funded healthcare programs to deliver more effective care. HMA consultants are leading conversations and presentations on how digital innovation is driving change in Medicare, Medicaid, and state marketplaces.
Key Sessions (full agenda and panelists here)
The Dynamic World of Publicly Sponsored Health Care: Trends and Innovations: Learn about new payment models, quality and equity initiatives, new products and services, workforce, likely policy initiatives, and new ways of reaching and serving members. (Monday 9:15-10:30am plenary session)
Digital Health, Interoperability, and Information Sharing: From Compliance to Innovation: Discover how early adopters will show how they have moved from compliance to innovation by embracing data sharing, FHIR APIs, and third-party applications using real-time data. (Monday 1:30-3:00pm breakout session)
The Pitch: Innovative and Potentially Disruptive Models in Care Delivery: Hear the latest innovations in care delivery models and will also gain an understanding of how to best approach managed care partners when considering value-based contracting or other network arrangements. (Monday 3:30-5:00pm breakout session)
Behavioral Health System Redesign: Learn why federal and state governments and the healthcare delivery system must collaborate in new and innovative ways to meet the rapidly growing demand for a more integrated behavioral health system (Sunday preconference, this session and others running 1pm – 5pm)
To learn more about HMA’s work in the digital innovation space or digital health work, please contact our experts below.

Webinar replay: Behavioral health: moving access to care and network adequacy into the 21st century
This webinar was held on September 7, 2023.
States, counties, health plans, and providers are asking how to meet the growing demand for behavioral health (BH) services. HMA teamed with experts to discuss these challenges at our recent Quality Conference where we crowdsourced ideas for how to redefine and measure network adequacy, examining provider selection, community need, and measurement.
This webinar reconvened those panelists to continue this critical conversation, shared feedback on factors that lead to “adequate” provider capacity, and discussed the impact of new federal network adequacy standards.
The conversation won’t stop with this webinar. We’ll use our continuously crowdsourced information and material for our BH workshop on Oct. 29, (the day prior to the start of the 2023 HMA Conference), making the connection between how large system reform in BH will shape how we think about network adequacy. We hope you’ll join us.
Learning Objectives
- Understand widely varying state standards for BH network adequacy and metrics — and validity concerns about how provider volume is assessed.
- Consider the true impact of BH provider shortage on care. (Reality check: we do not have enough BH providers and will not catch up at the current rate of training.)
- Learn about treatment engagement challenges and the need to establish criteria for discharge or discontinuation of treatment.
- Understand how extending BH workforce capacity with peer networks might ease shortage concerns.
- Hear about Delaware’s challenges and innovations to build an end-to-end ecosystem of care, shifting toward a journey rather than an episode of care.
- Learn about recent federal reform and new standards around network adequacy.
Speakers
Nazlim Hagmann, MD, MPH
Senior Vice President and Associate Chief Medical Officer, Commonwealth Care Alliance
Rhonda Robinson Beale, MD
Senior Vice President and Deputy Chief Medical Officer, UnitedHealth Group
Claire Wang, MD, ScD
Associate Deputy Director, Division of Substance Abuse and Mental Health, Delaware State Department of Health and Social Services
CMS rolls out new initiatives: key updates to watch this fall
In this week’s In Focus, we continue our review of Medicare developments from this summer and look ahead at Centers for Medicare & Medicaid Services (CMS) activities to watch for this fall.
CMS ACO Strategy Update
In a July 31, 2023, Health Affairs Forefront blog, CMS leaders outlined the agency’s plan to further accelerate the growth and accessibility of accountable care organizations (ACOs), especially for beneficiaries in rural and underserved areas. The article signals the agency’s continued commitment to increasing participation in ACOs and future policy and model initiatives that CMS could undertake to achieve those goals.
In particular, the CMS Innovation Center is considering testing models and features to support Medicare Shared Savings Program (MSSP) ACOs in increasing investments in primary care. This initiative might include piloting ACO-based primary care models that provide prospective payments in an effort to reduce reliance on fee-for-service (FFS), support innovations in care delivery, and increase access to advanced primary care in underserved communities.
CMS leaders point to a second component of its ACO strategy in the calendar year (CY) 2024 proposed Medicare Physician Fee Schedule (PFS) rule. The proposed PFS includes technical updates to the Advance Investment Payment (AIP), which provides financial support for providers who participate in the MSSP. The proposed PFS rule also includes several opportunities for the public to inform CMS’s ongoing ACO work, including considerations for adding higher-risk participation options in the MSSP, ways to better support collaboration between ACOs and community-based organizations to meet health-related social needs, and other initiatives. HMA discussed the PFS changes in an earlier In Focus.
CMS also announced refinements to the ACO Realizing Equity, Access, and Community Health (REACH) Model on August 18. The agency’s three goals in making these changes are to:
- Increase predictability for model participants (e.g., policies to change certain beneficiary alignment requirements and refinements to eligibility criteria for high-need ACOs
- Protect against inappropriate risk score growth (e.g., revisions to the risk-adjustment methodology)
- Advance health equity (e.g., revisions and expansions to the health equity benchmark adjustment)
These topics are of importance to CMS across its model portfolio and are, in part, based on experience the agency has gained in running the ACO REACH model. Below is a summary of several key policy changes that will take effect in 2024. The entire list can be found on the CMS website.
Finally, CMS released the request for applications (RFA) for the Innovation Center’s Making Care Primary (MCP) model previously announced in June. This voluntary model is scheduled to begin in June 2024 and run for 10.5 years. It will have three participation tracks that build upon previous Innovation Center primary care initiatives.
The MCP model is designed to improve care for beneficiaries by supporting the delivery of advanced primary care services. This framework provides a pathway for primary care clinicians who have varying levels of experience with value-based care to gradually adopt prospective, population-based payments while building the infrastructure to improve behavioral health and specialty integration and drive more equitable access to care. CMS is working with Medicaid agencies in eight states—Colorado, North Carolina, New Jersey, New Mexico, New York, Minnesota, Massachusetts, and Washington—to engage in full care transformation across payers, with plans to engage private payers in the coming months.
The RFA provides additional details about the model’s payment, care delivery, quality, and other policies. The application period opens September 4, 2023, and closes November 30, 2023. CMS plans to select participants in winter 2024. Onboarding for participants will take place April−July 2024.
The HMA team continues to review the RFA and is available to assist clients in determining whether this model may be a good fit as well as with assistance in submitting the application.
What to Watch
Comments on the Medicare CY payment rules (home health, end stage renal disease, physician, and outpatient hospital) are due in early fall. CMS will review the comments on each of the proposals and finalize each rule by November 1. Some stakeholders, such as physicians and home health suppliers, may seek congressional action to mitigate payment cuts that CMS has proposed.
In addition, CMS is expected to continue implementing the drug pricing related provisions of the Inflation Reduction Act (IRA). The agency already has released several guidance documents about the process. The list of the first 10 drugs to be negotiated is due to be published September 1, 2023, and manufacturers of selected drugs will have one month to sign agreements to participate in negotiations and provide information for CMS’s consideration in the negotiation process.
The HMA team will continue to evaluate Innovation Center opportunities, CMS payment regulations, and IRA implementation. If you have questions about these topics, contact our experts below.

Health Equity and Equity-Centered Strategic Approaches
There is significant and increasing demand across health and human services to address health inequities and eliminate disparities in service delivery and positive health outcomes. Organizations are asked to provide healthcare in holistic ways that recognize both individual and population-level needs.

Three areas of activity in this space include:
Diversity, Equity, and Inclusion (DEI) work to address inequities within organizations
Equitable access to care and service delivery to improve outcomes and eliminate health disparities
Community wellness and population health outcome improvement
Recent changes in federal and state policy and financing are driving equity advancement, chiefly: Executive Order 13985 to Advance Racial Equity and Support for Underserved Communities Through the Federal Government, which paves the way for the nation’s first racial equity blueprint for federal agencies; and the Centers for Medicare and Medicaid Services’ (CMS) strategic pillar on health equity, including an equity framework for payment policy through 2032. In addition, current and pending 1115 waivers from several states pay significant attention to equity by addressing social determinants of health and health related social needs.

HMA can help organizations across the health and human service spectrum operationalize health and racial equity.
We acknowledge that to improve health and social service outcomes at individual and community levels, we need to work across sectors and enterprises. We believe embedding equity practices and strategies throughout health and human services will deliver results and develop new innovative partnerships.
OUR TEAM CAN HELP YOU:
Assess organizational climate, policies, practices, and impacts
Establish equity as a critical foundation of your organizational culture in a way that is apparent and transparent to staff and clients
Identify priorities to infuse equity throughout the organization
Create plans for ongoing feedback and organizational action responsive to staff and client needs
Apply population health management approaches to delivery system redesign grounded in addressing social determinants of health and health-related social needs
Strategic planning
Training
Technical assistance
Implementation
Ongoing guidance
Align organizational strategy with an actionable equity agenda
Work with leadership and staff to ensure that your organization’s activities are designed and implemented in a way that supports an equity agenda for both staff and clients
Facilitate equity workshops and build organizational capacity
Design and facilitate equity workshops to build organizational competencies, including: Equity principles and fundamentals, Equitable practice strategies, metrics, and continuous quality improvement, Cultural humility and community engagement approaches
Plan, convene, and facilitate forums for large and small groups within a workplace or system ensuring buy-in from involved parties and leadership
Establish a framework for mutual support and information sharing while integrating insights through continued learning and dialogue.
Our Services
Assessment, mitigation, and remediation
Community engagement
Equitable access and service delivery design
Stakeholder engagement and facilitation
Organizational assessment
Change management
Strategic planning and implementation
Training and technical assistance
HEALTH EQUITY IMPACT ASSESSMENT SERVICES
A Health Equity Impact Assessment (HEIA) can help organizations understand the potential impact, positive and/or negative, that a change to the delivery system may have on a facility’s existing patients and the health and wellbeing of the surrounding community.
Pivotal to any HEIA is meaningful stakeholder engagement, the format of which may vary depending on the project, and high‐quality data analysis.

HMA colleagues routinely:
Design and program online surveys
Conduct key informant interviews
Facilitate focus groups and public deliberations
Synthesize stakeholder feedback
Conduct community health needs assessments
Analyze health indicators and incidence rates in populations
Contact our experts:

Leticia Reyes-Nash
Regional Director

Charles Robbins
Principal

Madeleine (Maddy) Shea
Principal
Arizona releases Medicaid ALTCS-EPD Program RFP
This week, our In Focus section reviews the Arizona Long Term Care System (ALTCS) Elderly and Physically Disabled (EPD) Program request for proposals (RFP), which the Arizona Health Care Cost Containment System (AHCCCS) released on August 1, 2023. The ALTCS-EPD program covers 26,000 individuals, representing approximately 38 percent of the ALTCS managed care population. The remaining ALTCS members are covered under a state-run model through the Department of Economic Security, Division of Developmental Disabilities (DES/DDD) health plans, which provide long-term care (LTC) to individuals with intellectual/developmental disabilities. Contracts for ALTCS-EPD are worth approximately $1.6 billion and will take effect October 1, 2024.
Background
ALTCS is one of the oldest Medicaid managed long-term services and supports (MLTSS) programs in the country, providing integrated physical health, behavioral health, and LTSS to individuals who are 65 years of age or older or who have a disability and require nursing facility level care. Beneficiaries may live in assisted living facilities or receive in-home services. The ALTCS-EPD program covers nearly all Arizonans who are dually eligible for Medicaid and Medicare statewide. Winning managed care organizations (MCOs) also will be required to implement companion Medicare Advantage Fully Integrated D-SNPs (FIDE SNPs) effective January 1, 2025.
Market
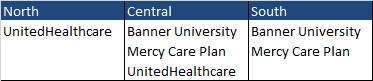
Members receive coverage through Banner-University Family Care, Mercy Care Plan, and UnitedHealthcare, depending on their geographic service area (GSA). MCOs will bid on all three GSAs and indicate their order of preference to be awarded. AHCCCS will not award the South GSA only or the North GSA only. At present, in the South region, Mercy Care Plan serves Pima County only. Under the new RFP, AHCCCS will not make an award specific to Pima County; rather the MCO will serve all seven counties within the South GSA.
Together, the plans cover 25,973 individuals (see below).
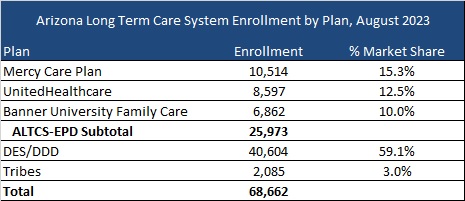
(United and Mercy administer DDD plans.)
Timeline
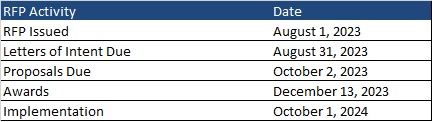
Intent to bid forms are due by August 31. Proposals are due October 2, and awards are expected to be announced December 13. As noted previously, implementation is scheduled to begin October 1, 2024.
Learning the invaluable lessons of value-based care at 2023 HMA conference
If you search the term “value-based care” on the internet you will find over 2.5 million hits on that term alone. No one would disagree with the need to provide value to patients and purchasers, but how we define value differs based on where we sit. Value is paying for outcomes, not volume of services. Value is ensuring that patients get the right care at the right time. Value is ensuring that purchasers pay a reasonable cost for the highest possible quality. Value is ensuring that healthcare is provided equitably and sustainably. Implementing value is even trickier than defining it, given the complexity of who pays for care and the challenges of measuring the outcomes we seek to reward.
From the top office of HHS to the back office of a health center and everywhere in between, HMA leaders have been part of our collective journey to value: advancing policy and regulatory change, calculating risk and setting prices, crafting alternative payment models, integrating social services and behavioral health, and coaching industry leaders to make important changes to their business models to adapt to a more sustainable approach to American healthcare. These experiences – both successes and challenges – provide a unique perspective from which to advise clients on transformation of healthcare.
The HMA 2023 fall conference, scheduled for October 30-31, 2023, has thoughtfully curated several discussions to educate, enlighten and motivate attendees on industry standards and navigating the practicality of providing value in care, coverage, and patient experience in publicly funded healthcare:
Leading the Charge on Value, Equity and Growth: The Future of Publicly Sponsored Healthcare: Discuss how these public programs came to be the industry standard bearers and what this shift means for outcomes, affordability, policy, and the overall direction of U.S. healthcare.
Positive Change and the Growing Importance of Managed Care in Publicly Sponsored Healthcare: Discuss the future of publicly sponsored healthcare, outline promising initiatives aimed at improving coverage and care, and address key concerns over funding, policy, equity, and coordination between government, plans, providers, and members.
The Future of Delivery Systems: Achieving Operational and Financial Sustainability: Discuss a wide range of practical approaches to prepare for the future, including managing cash flow, optimizing the workforce, developing long-term reimbursement plans, improving operational efficiency, and addressing changes in government policy.
Real Talk from the Trenches of Value-based Payments: Learn about the advantages and pitfalls of value-based payments, with important insights from organizations that have made it work.
Navigating Change in Medicare Advantage: A Roadmap for Success: Discuss what Medicare Advantage plans must do to meet the demanding, new requirements – all against a backdrop of continued efforts to improve equity, access, outcomes, and cost.
In addition, a pre-conference workshop on behavioral health will be held the afternoon of October 29th, prior to the official start of the conference. This workshop will highlight the integral role of behavioral healthcare in improving patient outcomes across the continuum of publicly sponsored healthcare programs.
We are excited to engage with industry experts throughout these discussions about value-based care and forge a better path forward toward a more sustainable and equitable system of care.
Webinar replay: Medicare policy changes impacting behavioral health services workforce and population health
This webinar was held on September 12, 2023.
Continuing our discussion from Part 1 of this series, recent rule changes proposed by the Centers for Medicare and Medicaid Services (CMS) will enable regulatory and statutory expansion of behavioral health services and providers. This webinar focused on how those changes will impact the already strained workforce, and the corresponding impacts on population health, value-based care, and the needs of special populations. Experts dove deeper into approaches health systems may adopt to handle workforce shortages while expanding access.
Learning Objectives:
- Understand how CMS rule updates on behavioral health services will help expand needed care for Medicare recipients and dual eligible populations.
- Create strategies for addressing the 2023 CMS rule updates to benefit employers and delivery systems toward improving whole health outcomes and reducing behavioral health workforce shortages.
CMS finalizes 2024 hospital inpatient rule with mixed reimbursement changes
This week, our In Focus section continues analysis and insights from Health Management Associates (HMA) and its affiliate The Moran Company on recent Medicare payment and policy developments. Today, we review the policy changes that the Centers for Medicare & Medicaid Services (CMS) released August 1, 2023, for the fiscal year (FY) 2024 Medicare Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Acute Care Hospital (LTCH) final rule (CMS-1788-F).
This year’s IPPS final rule includes several important policy changes that will alter hospital margins and change administrative procedures beginning October 1, 2023. More specifically, the IPPS rule increases payments to hospitals, enhances the wage index policy for rural hospitals, reduces Medicare disproportionate share payments, and modifies the New Technology Add-on Payment (NTAP) program.
Key provisions of the FY 2024 Hospital IPPS and LTCH Final Rule
We highlight four policies that will significantly affect Medicare beneficiaries, hospitals, health systems, payers, and manufacturers:
- The annual inpatient payment update
- Medicare disproportionate share hospital (DSH) payments
- Hospital wage index adjustments
- NTAP policy changes
Hospital market basket update and the inpatient standardized amount
CMS’s Medicare 2024 IPPS final rule will increase payments to acute care hospitals by an estimated $2.2 billion from 2023. The primary driver of this increase is CMS’s 3.1 percent increase in the annual update to inpatient operating payment rates. The update is the sum of the hospital market basket update of 3.3 percent and a statutorily required 0.2 percentage point reduction for productivity growth.
HMA/Moran analysis: Between the time CMS released the 2024 proposed IPPS rule and the final rule, the inpatient payment update for 2024 increased to 3.1 percent from 2.8 percent. This spike occurred because of the effects of an increase in estimated inflation on the cost of a standard basket of hospital goods (hospital market basket) throughout 2022 and 2023. Although economy-wide inflation slowed in mid-2023, inflation was higher in late 2022 and early 2023—the period in which the market basket is measured for the final rule.
For beneficiaries, increasing payment rates eventually will lead to a higher Medicare inpatient deductible and greater out-of-pocket costs for many other services. For hospitals and healthcare systems, payers, and manufacturers, a payment increase of 3.1 percent falls below economy-wide inflation (5−6 percent in recent months).
Despite the publicized 3.1 percent payment update for 2024, after factoring in various policy adjustments the actual change between 2023 and 2024 to inpatient payments per case will be roughly 2 percent. The primary reason per-case payments will increase only 2 percent is a budget-neutrality adjustment that CMS finalized for 2024 to account for hospital wage index reclassifications. This adjustment will reduce payments to all hospitals by more than 1 percent to neutralize the added program spending associated with payments to hospitals that choose to reclassify into higher paying wage index areas. The final rule states, “[T]he geographic reclassification budget neutrality adjustment is significantly larger than in prior years.”
Medicare Disproportionate Share Hospital Payments
CMS finalized two Medicare disproportionate share hospital (DSH)-related policies for 2024. First, DSH payments and Medicare uncompensated care payments combined will decrease in FY 2024 by approximately $957 million. Second, CMS finalized its proposal to limit the number of patient days included in the Medicare DSH calculation to only those days when the patient’s Medicaid Section 1115 Demonstration health insurance covers inpatient hospital services or the patient’s premium assistance program covers 100 percent of the premium cost for patients who buy health insurance that covers inpatient hospital services, if the patient is ineligible for Medicare Part A.
HMA/Moran analysis: CMS’s $957 million reduction in DSH and uncompensated care payments stems from the agency’s estimate of the percentage of individuals without insurance in the United States. Between the 2024 proposed and final rules, CMS estimates the percentage of individuals without insurance will decline from 9.3 percent to 7.7 percent in 2023 and from 9.2 percent to 8.5 percent in 2024. As a result, the pool of uncompensated care dollars available to hospitals for 2024 was reduced from roughly $6.7 billion to $5.9 billion.
CMS’s estimated decline in the rate of uninsured beneficiaries is somewhat surprising given the common projection that Medicaid enrollment will drop following the end of Medicaid’s COVID-19 related continuous coverage policy. However, HMA/Moran colleagues believe state-level Medicaid enrollment changes will vary in the year ahead. Consequently, hospitals located in states where levels of Medicaid enrollment are sustained will benefit from CMS’s uninsured rate estimates and hospitals in states where Medicaid enrollment drops will not.
With regard to the Section 1115 demonstration related DSH policy, hospitals located in states that have not expanded Medicaid under the Accountable Care Act and instead rely on Section 1115 Demonstrations to expand health coverage, are likely to receive lower DSH payments. In addition to the Medicare DSH payment adjustments, reductions in the Medicaid DSH program are scheduled to begin October 1, 2023. The $8 billion reduction in FY 2024 is the first time CMS has planned to make cuts in the program.
Hospital Wage Index Adjustments
CMS finalized two wage index policies for FY 2024. First, CMS will extend the low-wage index hospital policy, which boosts the wage index of hospitals in geographic areas with low wages relative to other areas. Second, CMS finalized a policy to begin including labor data from urban hospitals that choose to reclassify as providers in rural areas to maximize their payment into the calculation of rural wage index areas.
HMA/Moran analysis: These two wage index policies for FY 2024 will increase payment to rural hospitals. Under the first policy, hospitals with wage indexes below 0.8667 (the 25th percentile across all hospitals) will automatically receive an increase in their wage index and therefore their payment rates for inpatient cases. Under the second policy, the inclusion of labor data for geographically urban hospitals that choose to reclassify into rural wage index areas within the calculation of state-level rural wage indexes and the state-level rural floor will increase payments to rural hospitals in many states. The overall impact of both proposed wage index policy changes for FY 2024 will be an increase in inpatient payment rates for rural hospitals.
New Technology Add-On Payments (NTAP)
Citing the increased number of applications for NTAP over the past several years and noting the need for CMS staff to have time to review and analyze the applications, CMS finalized two changes to the NTAP application requirements. First, CMS will require that all applicants have a complete and active U.S. Food and Drug Administration (FDA) market authorization request in place at the time of NTAP application submission, if not already FDA approved. The FDA’s acceptance letter will serve as proof of a full and complete application. In addition, CMS proposes to move the FDA approval deadline from July 1 to May 1, beginning with applications for FY 2025.
HMA/Moran analysis: The stated aim of these CMS policy changes is to “increase transparency, facilitate public input, and improve the review process.” As a result of these modifications, products will need to be on the market longer before the NTAP payment begins, and fewer products will be eligible for the three full years of NTAP payments. Taken together, hospitals will have a shorter NTAP payment window for most products. The further tightening of FDA application and approval requirements runs counter to the efforts of various stakeholders to establish more flexible or additional NTAP application windows.
HMA and The Moran Company collaborate to monitor legislative and regulatory developments in the inpatient hospital space and assess the impact of inpatient policy changes on the hospital sector. HMA’s Medicare experts interpret and model inpatient policy proposals and use these analyses to help clients develop their strategic plans and their comments on proposed regulations. Moran replicates the methodologies CMS uses in setting hospital payments and models alternative payment policies to help support stakeholder comment letters and strategies. Moran also assists clients with modeling diagnosis-related group reassignment requests and to support innovative NTAP applications.
For more information or questions about the policies described above, contact our experts below.

August 9, 2023
CMS Finalizes Mix of Reimbursement Reductions and Increases in 2024 Hospital Inpatient Final Rule