November 5, 2025
This week's roundup:
- In Focus: CY 2026 Physician Fee Schedule Tackles Site Neutrality, Cost-Drivers, and Alternative Payment Models

- In Focus: Cross-Sector Collaboration: Unlocking the Full Potential of Community-Based Services in a Challenging Funding Climate
- Colorado Governor Proposes Fiscal 2027 Budget with Medicaid Cost-Saving Proposals
- Kansas Audit Flags Issues in KanCare Oversight, MCO Claim Denials
- Louisiana Issues EVV Solution RFI
- HRSA Approves Eight Manufacturers to Participate in 340B Drug Pricing Pilot Program
- Trump Administration Orders States to Review Medicaid Rolls for Undocumented Immigrants
- House Lawmakers Unveil Bipartisan Framework to Extend ACA Subsidies
- EmblemHealth Launches New Pharmacy Benefit Partnership with Prime Therapeutics, Amazon Pharmacy
In Focus
CY 2026 Physician Fee Schedule Tackles Site Neutrality, Cost-Drivers, and Alternative Payment Models
On October 31, 2025, the Centers for Medicare & Medicaid Services (CMS) announced the final rule for the calendar year (CY) 2026 Medicare Physician Fee Schedule (PFS), which finalizes payment policies proposed earlier this year. The rule continues the administration’s focus on developing value-based payment strategies, enhancing care management, and developing innovative payment models. It emphasizes a shift from historical processes and methods of reimbursing clinician services, while also introducing payment policies that include a shift toward site neutrality and cost containment.
The final CY 2026 rule implements immediate policy changes and signals several areas on which CMS might focus its attention in future rulemaking. Through its responses to public comments and the rationale provided for finalized policies, CMS highlights potential shifts in priorities and emerging directions for Medicare payment policy, reflecting the views of the Trump Administration moving forward. Stakeholders should be attentive to these signals, as they provide valuable insights into where CMS could direct further reforms and adjustments in the coming years.
Health Management Associates (HMA) Medicare experts are reviewing the finalized policies and have identified the highlights outlined in this article. Stakeholders should consider the effect on payment in 2026 as well as the longer-term practice reforms, investments, and analysis that may be required to deliver high-quality services and remain sustainable.
Enhanced Care and Chronic Disease Management
CMS finalized new billing codes to support behavioral health integration and the Psychiatric Collaborative Care Model (CoCM) services delivered to patients who also receive Advanced Primary Care Management (APCM) benefits, along with an add-on code for in-home primary care to reflect added complexity. CMS also retains and repurposes the social determinants of health (SDOH) risk assessments billing code to align with the administration’s focus on addressing the root causes of chronic illness.
Takeaway: These changes are designed to support better care coordination, integration of physical and mental health services, and proactive management of patient risk factors. They indicate CMS’s intent to expand care management strategies beyond traditional settings and into future payment methodologies.
Establishing Specialty Care Models
The rule finalizes the mandatory Ambulatory Specialty Model (ASM) to test value-based payments for specialists who focus on heart failure and lower back pain. ASM adopts a framework similar to the Merit-based Incentive Payment System Value Pathways (MVP) and shares certain quality and cost measures with existing MVPs for heart disease and musculoskeletal care.
The model applies performance-based payment adjustments of up to 12 percent, covering 25 percent of Core-Based Statistical Areas (CBSAs) and metropolitan divisions, and is projected to save $177 million over its test period. ASM will run from 2027-2031, with payment adjustments applied during payment years from 2029-2033.
Takeaway: Stakeholders should plan for CMS’s continued interest in developing mandatory models and opportunities for specialists to participate in Innovation Center efforts.
Emphasis on Rebalancing the Payment System and Site Neutrality
Efficiency Adjustment
Citing the need to account for efficiencies gained in non-time-based services such as procedures, radiology services, and diagnostic tests, CMS finalized a 2.5 percent efficiency adjustment to work Relative Value Units (RVUs) for certain services and procedures, applied every three years. The agency notes it will monitor the three-year cadence and may refine the frequency in future rulemaking.
In response to public comments, CMS added several services to the exemption list in this final rule, including codes that introduced to the fee schedule in 2026, certain time-based services in physical medicine and rehabilitation, remote therapeutic monitoring (RTM), and drug administration, as well as time-based services on the CMS telehealth list.
Takeaway: The move signals a notable shift from the agency’s historical reliance on survey data provided by the American Medical Association (AMA)/Specialty Society Relative Value Scale (RVS) Update Committee (RUC) to establish practitioner time in PFS rate setting. Stakeholders should consider how CMS could build on this new approach in future rulemaking.
Site Neutrality
Site neutral policies will now use hospital outpatient data to set payment rates for certain services, including radiation oncology treatment delivery and some remote monitoring. In addition, the rule establishes the same payment rate in both physician office and hospital outpatient settings for certain supplies, including skin substitute products, and by implementing changes in the physician practice expense methodology.
By tackling practice expense reimbursement, CMS intends to recognize higher costs incurred by physicians who operate a freestanding office than by physicians who furnish care in the facility setting (i.e., indirect practice expenses). This methodology lowers practice expense payments to hospital-based physicians, resulting in double-digit cuts for many specialists in facility settings, while independent and group practice physicians generally will see increases.
Takeaway: The site neutrality changes underscore a broader long-term strategy advanced across multiple administrations to reduce payment disparities and discourage shifting care to higher-cost settings. While some providers will see payment increases and others will experience cuts, these adjustments are part of CMS’s effort to rebalance incentives and move toward value-based models. Stakeholders should recognize that this is not an isolated change, but a signal of continued policy evolution designed to align payment with efficiency and quality.
Strategies to Update PFS Practice Expense Payments
Although CMS implemented major methodology changes to allocate more indirect practice expense (PE) costs to services performed in physician offices and less to those in facility settings, the agency finalized a “status quo” approach. Specifically, the agency will continue using the existing practice expense per hour (PE/HR) values and cost share weights, despite being almost two decades out of date.
Takeaway: CMS indicates interest in revisiting practice expense data in future cycles, which may effect payment.
Positive PFS Conversion Factor Update
All providers and suppliers paid for services under the PFS will benefit from a positive update to the conversion factor, with Advanced Alternative Payment Model (APM) participants receiving a higher increase and one-time incentive payment. Specifically, under the final rule, two conversion factors will be available in CY 2026.
- CMS will pay for services furnished by providers who participate in APMs using a conversion factor of $33.5675—a 3.77 percent increase (or $1.221) from the 2025 amount of $32.3465.
- CMS will compensate providers who do not participate in a qualifying APM using conversion factor of $33.4009—a 3.26 percent ($1.0544) from CY 2025.
Both conversion factors reflect the 2.50 percent overall update required by statute, a 0.49 percent budget neutrality adjustment to account for RVU changes, and an updated factor of 0.75 percent for qualified APMs or 0.25 percent for non-qualifying APMs. CY 2026 is the final year in which eligible clinicians can receive an additional APM incentive. Qualifying clinicians will receive a one-time payment of 1.88 percent of their paid claims for covered professional services based on their performance two years earlier.
Takeaway: These updates provide short-term financial relief. The higher increase and bonus for APM participants signal CMS’s continued push toward alternative payment models, even as the incentive sunsets. Stakeholders should plan for a future in which APM participation remains a key strategy for maintaining revenue stability.
Telehealth-Related Flexibilities
CMS will implement several policy changes that will collectively extend the footprint of telehealth services in Medicare and expand access for Medicare beneficiaries. These changes directly impact Traditional Medicare beneficiaries, physicians’ offices, hospitals, and Federally Qualified Health Centers (FQHC) and Rural Health Clinics (RHC).
- All services on CMS’s Medicare telehealth coverage list are now permanently covered if they are separately payable and can be delivered via two-way audio-video.
- CMS permanently removed frequency limitations on certain telehealth services, including follow-up inpatient and nursing facility services.
- FQHCs and RHCs can serve as distant site telehealth providers for all services—not just mental health services—through December 31, 2026.
- Virtual supervision is permanently allowed for nonsurgical services conducted in real time via two-way audio-video. This policy will apply across all settings, including FQHCs and RHCs requiring an on-site supervising physician.
- Teaching physicians can be virtually present for resident services delivered in all training settings when care is provided via telehealth.
- New services added to the Medicare telehealth coverage list, including certain psychological rehabilitation services, caregiver training services, and risk assessment services.
Takeaway: These changes solidify that telehealth has become an integral part of Medicare service delivery. By eliminating the distinction between temporary and permanent coverage, removing frequency limits, and allowing virtual supervision and teaching physician presence, CMS advances telehealth as a core component of its long-term strategy to improve access, care coordination, and efficiency. In addition, the change aligns with CMS’s commitment to modernizing payment policies to support virtual care models. Stakeholders should plan for continued growth and innovation in this space in future rulemaking cycles.
Other Final Policies
- Addressing Rising Expenditures for Skin Substitutes: CMS addresses rising expenditures for skin substitute products, which are being adopted and used at a rapid rate. Specifically, the agency reclassifies most of these products as supplies billed incident-to physician services, paid at a uniform rate in both office and hospital outpatient settings rather than as Part B drugs. CMS projects that this change will save Medicare $19.6 billion in 2026 and standardize payment to providers who use these products. The policy takes effect on January 1, 2026. Accompanying these changes is the launch of a new model to test clinical review for certain services, including skin substitutes, in fee-for-service Medicare.
- Medicare Shared Savings Program: CMS finalizes its proposal to limit the amount of time an accountable care organization (ACO) can participate in an upside-only risk track, provide more flexibility on the number of beneficiaries assigned to an ACO in its early year of operation, and refine quality measures and improve beneficiary attribution to better reflect care standards.
- Drugs and Biological Products Incident-to Physician Services: The final rule addresses reimbursement for drugs paid incident-to a physician’s service, including policies related to the Inflation Reduction Act provisions, continued implementation of discarded units refund requirements, changes and clarifications to average sales price (ASP) reporting, and payment for procedures required to manufacture cell-based gene therapies.
- Coding and Payment for Technology-Based Services: CMS pays for digital mental health treatment (DMHT) devices that have Food and Drug Administration (FDA) clearance or authorization and are furnished in conjunction with professional services, including initial education and onboarding. CMS expands these payment policies for DMHT used to treat of attention deficit hyperactivity disorder when providers adhere to established billing requirements. The agency recognizes that behavioral health conditions are common chronic diseases and that the field of digital therapeutics is evolving.
Contact an HMA Medicare Expert Today
HMA policy and rate setting experts are analyzing the details and impacts of the proposed rule and will provide additional updates on key Medicare policies as they become available. Our team can support stakeholder development of policy and data-oriented comments pertaining to this rule and on any other Medicare topic of interest. Contact Amy Bassano, Rachel Kramer, and Kevin Kirby to discuss your priorities and approach.
Cross-Sector Collaboration: Unlocking the Full Potential of Community-Based Services in a Challenging Funding Climate
Lessons Learned from State-Led Transformation Efforts
As federal and state healthcare policy continues to evolve, the need for cross-sector collaboration has never been more urgent. The 2025 budget reconciliation act (OBBBA, P.L. 119-21) introduces significant changes to Medicaid eligibility and financing, prompting a shift in strategy for policymakers and advocates working to advance whole-person care and address social determinants of health (SDOH). The new policies reflect a reorientation of Medicaid financing, with a greater emphasis on state flexibility, targeted benefits, and value-based care.
In this environment, enhanced partnerships and strategic alignment across sectors will be essential to sustain community-based services and workforce investments. In this article, Health Management Associates (HMA), experts highlight key observations from multiple state transformation programs, including actionable strategies for leveraging these assets and meeting the needs of at-risk populations.
Revisiting SDOH Initiatives in a New Policy Context
Whole-person care models have long called for integrated, multidisciplinary approaches. These models—once buoyed by COVID-19 pandemic-era funding and broad federal support—must now be recalibrated to align with new federal priorities. Current federal priorities emphasize streamlined benefits, fiscal discipline, and state-led innovation, which presents both challenges and opportunities for advancing integrated care. This shift has heightened the need to clarify roles and responsibilities across clinical and community settings, focusing on how to maintain essential linkages to primary and preventive care, especially for individuals for whom access remains fragile.
In addition, the ongoing healthcare workforce crisis intensifies the need for creative approaches to whole-person care models. Solutions must go beyond traditional payment models, leveraging existing social care networks, shared hub functions, alternative payment strategies above base rates, and braided funding streams.
State and federal initiatives can be used to sustain momentum and test emerging models. For example, the Rural Health Transformation Program (RHTP) offers a critical opportunity to support these efforts. With $50 billion in funding over five years, RHTP is designed to help states implement innovative models that improve rural health outcomes, strengthen workforce capacity, and address SDOH. States will be finalizing their applications to meet the November 5 deadline. HMA is tracking how these applications align with the strategies outlined below, using the program’s baseline and performance-based funding to invest in infrastructure, workforce development, and cross-sector partnerships.
Key Lessons from State Transformation Programs
Drawing on recent transformation programs, HMA experts identified several key lessons, including:
- Prioritize Intensive, Community-Based Outreach: States and health plans should invest in community-based outreach strategies that reach populations facing the greatest SDOH barriers, including funding models that support navigation and engagement beyond traditional clinical settings and leveraging shared infrastructure to extend reach.
- Update Community Health Worker (CHW) Benefit Structure to Maximize Impact: States, in collaboration with their partners, should revisit CHW benefit design to allow for greater flexibility. Reducing reliance on clinical supervision and referral-only pathways can help CHWs operate more effectively in terms of outreach, education, and engagement.
- Strengthen Workforce Retention through Flexible Financing: Healthcare stakeholders should explore braided funding, shared hub models, and alternative payment models that go beyond base rates. These approaches can sustain staff and morale amid shifting demands and constrained budgets.
Connect with Us
The strategies in HMA’s recent report for Illinois, Medicaid Financing for Social Health: A Resource Compendium for Illinois Community-Based Organizations & Networks, can be adapted to other states and communities. By sharing lessons and adopting best practices from transformation programs nationwide, we can reinforce pathways to integrated care and ensure that populations continue to receive the support they need—even in the face of unprecedented challenges.
HMA experts are helping states, healthcare plans, and community partners adapt and thrive as federal and state policy landscapes continue evolving. HMA teams are applying their cross-sector expertise in SDOH, workforce development, and state-specific knowledge to help organizations better plan, implement, and develop programs to solve healthcare challenges in their community. For questions about the report or opportunities for your organization, reach out to Heidi Arthur and Leticia Reyes-Nash.
HMA Roundup
Colorado
Colorado Governor Proposes Fiscal 2027 Budget With Medicaid Cost-Saving Proposals. The Colorado Sun reported on October 31, 2025, that Governor Jared Polis has released his recommended budget for fiscal 2027 with significant cost saving proposals for Medicaid. Polis recommends increasing Medicaid spending by $300 million, which is less than half of what the state is projected to need to keep Medicaid at its current state. The proposal includes limiting home caregiver hours, changing rates for providers supervising people with autism, and codifying a recent executive order signed by the governor that caps some reimbursement rates and limits Medicaid dental benefits. Medicaid spending has risen by approximately 8.8 percent per year over the past decade, which is approximately double what Colorado is permitted to spend under the Taxpayer’s Bill of Rights (TABOR), causing the state to have to minimize spending in other areas.
Kansas
Kansas Audit Flags Issues in KanCare Oversight, MCO Claim Denials. The Kansas Reflector reported on October 31, 2025, that the Kansas inspector general’s office released its first audit under expanded legislative authority, identifying 17 issues within KanCare, the state’s Medicaid program. The review found that hospitals faced significant financial losses from high-value claim denials, which accounted for a disproportionate share of billions in rejected payments across the state’s three managed care organizations in 2023. It also raised potential conflict-of-interest concerns over UnitedHealthcare’s use of a proprietary billing and review system owned by one of its subsidiaries. The Kansas Department of Health and Environment (KDHE) is meeting with MCOs and the inspector general to address findings, and additional audits will examine Medicaid waivers, SNAP data-sharing, and other social service programs in 2026.
Louisiana
Louisiana Issues EVV Solution RFI. The Louisiana Department of Health (LDH) released on October 27, 2025, a request for information regarding the state’s electronic visit verification (EVV) solution used across multiple LDH programs. The department is seeking information from qualified vendors regarding data aggregator solutions that can comply with federal and state verification requirements, including system capabilities, integration options, security standards, and implementation timelines. Responses are due December 17, 2025.
National
HRSA Approves Eight Manufacturers to Participate in 340B Drug Pricing Pilot Program. Modern Healthcare reported on October 30, 2025, that the federal Health Resources and Services Administration (HRSA) approved proposals from AbbVie, Amgen, Astra Zeneca, Boehringer Ingelheim, Bristol Meyers Squibb, Johnson & Johnson, Merck, and Novo Nordisk to participate in the new 340B Drug Pricing Program rebate pilot. Under the program, participants will be able to test out paying rebates after they are purchased by qualified providers, rather than discounting drug prices up front. The program begins January 1, 2026, and will run for at least one year.
Trump Administration Orders States to Review Medicaid Rolls for Undocumented Immigrants. KFF Health News reported on November 3, 2025, that the Trump administration has directed state Medicaid agencies to review enrollee lists for undocumented immigrants. The Centers for Medicare & Medicaid Services (CMS) has sent states more than 170,000 names to investigate, citing concerns that over $1 billion in federal funds were spent on ineligible individuals. Several states, including Colorado, Illinois, and Washington, have disputed those claims, calling the figures inaccurate and politically motivated. Advocates and state officials warn the directive could cause eligible individuals to lose coverage due to administrative errors or missed verification deadlines.
House Lawmakers Unveil Bipartisan Framework to Extend ACA Subsidies. Politico reported on November 3, 2025, that a bipartisan group of House lawmakers released a statement of principles outlining a potential two-year extension of Affordable Care Act premium subsidies with an income eligibility cap between $200,000 and $400,000. The proposal, the first bipartisan health policy framework introduced since the federal shutdown began, seeks to establish common ground for extending enhanced tax credits while strengthening oversight of enrollment fraud and administrative practices. The plan is unlikely to gain support from conservative members opposed to continuing ACA subsidy enhancements.
Industry News
New York’s EmblemHealth Launches New Pharmacy Benefit Partnership with Prime Therapeutics, Amazon Pharmacy. EmblemHealth announced on October 29, 2025, a new pharmacy benefit partnership with Prime Therapeutics, Amazon Pharmacy, and Judi Health to improve drug pricing transparency and convenience for members. The collaboration introduces real-time competitive pricing for specialty medications, digital tools for cost visibility, and fast, free home delivery through Amazon Pharmacy. The initiative aims to modernize pharmacy benefit management and deliver a more transparent, accessible, and affordable experience for EmblemHealth members.
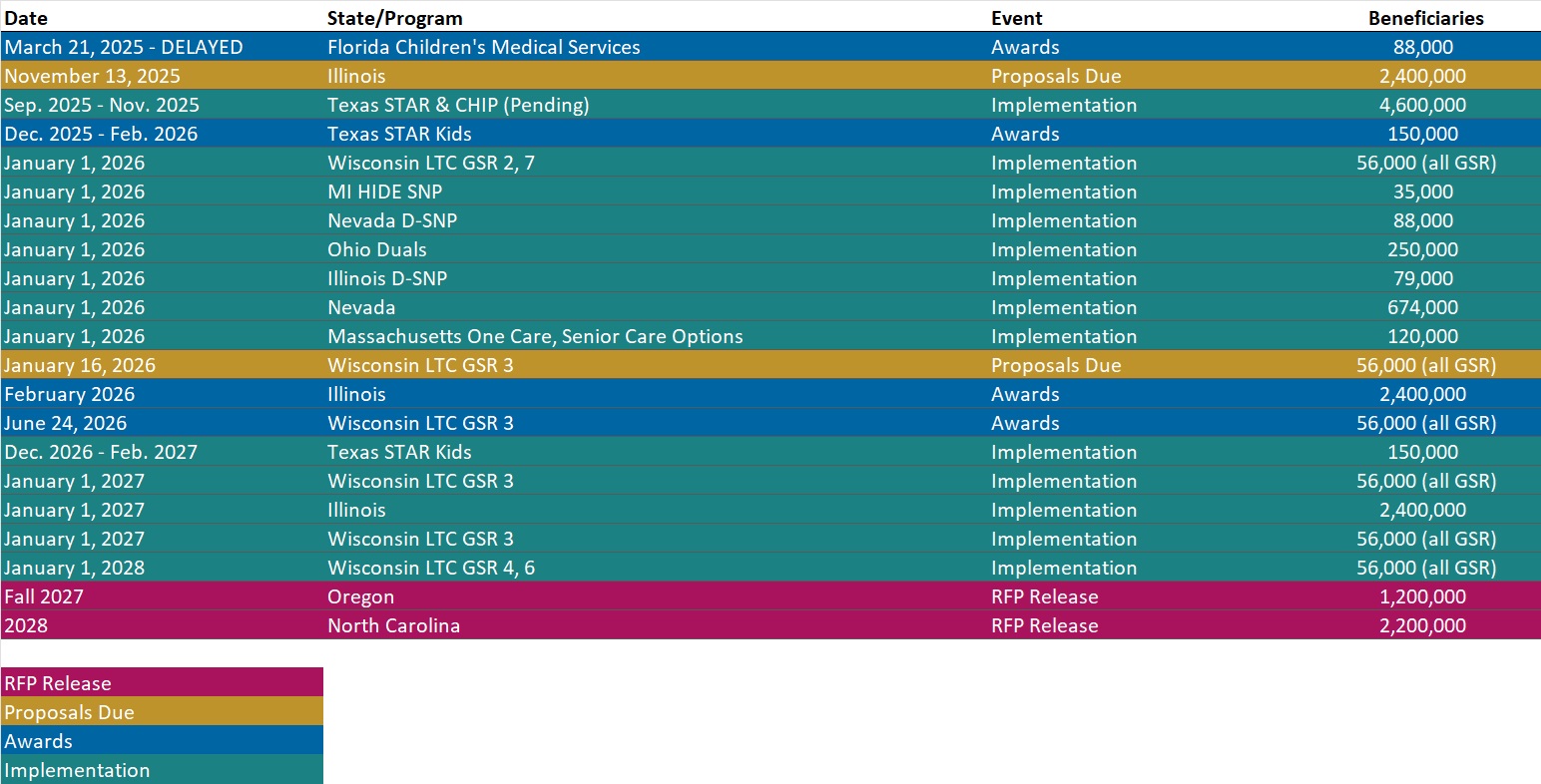
RFP Calendar
Actuaries Corner
Q3 Earnings Recap: For-Profit Hospitals’ Revenues Spike on Medicaid Supplemental Payments. Favorable shifts in patients’ source of insurance coverage played a key role in earnings increase, as did the acuity of cases and services being provided, the rates hospitals were able to demand and revenue cycle teams tasked with promptly winning claims disputes with payers. Editors Note: Funds were flowing during the third quarter, including some awaited payouts from prior periods that the companies framed as one-time items rather than recurring growth.
Discover other developments in the Wakely Wire here.
HMA News & Events
HMA Webinars
Impact Investing as Good Medicine: Prescribing Capital for Healthier Communities. Thursday, November 13, 2025, 12 PM ET. This webinar will convene investment professionals from major healthcare systems alongside leaders in impact investing to explore how strategic investments in the social drivers of health affordable housing, community infrastructure, food access and security, transportation, and local community and economic development—can both improve population health and deliver financial returns to healthcare systems and payers. Healthcare leaders will discuss how leveraging balance-sheet capital toward upstream solutions strengthens organizational sustainability, creates competitive differentiation in RFPs, builds community trust, and aligns with regulatory and value-based care incentives. Impact investing practitioners will discuss how they identify opportunities that deliver both financial performance and measurable health outcomes, and share lessons from structuring investments that balance institutional rigor with community impact. Register Here
Value Based Care Advisory Services: HMA and Wakely Put Analysis into Action. Thursday, November 20, 2025, 1 PM ET. Join experts from HMA and Wakely for an inside look at how our teams help organizations navigate and thrive in the value-based landscape. This session will highlight case studies and recent work that demonstrate a comprehensive advisory solution for any value-based entity. Attendees will gain a deeper understanding of how integrated insights across strategy, analytics, and implementation can drive measurable results in value-based care. Register Here
NEW THIS WEEK ON HMA INFORMATION SERVICES
(Exclusive Access for HMAIS Subscribers):
HMAIS Medicaid Market Overviews, Reports, and Data
- Updated Duals Integration Environmental Inventory
- Updated National Medicaid Dental Benefits Management RFP Calendar
- Updated HMA Federal Health Policy Snapshot
- New Medicaid enrollment, RFP documents, and other market intelligence resources for dozens of states
- Updated Utah and Vermont State Overviews
A subscription to HMA Information Services puts a world of Medicaid information at your fingertips, dramatically simplifying market research for strategic planning in healthcare services.
If you’re interested in becoming an HMAIS subscriber, contact Andrea Maresca at [email protected].