October 15, 2025
This week's roundup:
- In Focus: On the Horizon: Contract Year 2027 Proposed Rule Will Provide Trump Administration First Opportunity to Reshape Medicare Advantage Program

- In Focus: ACA Marketplaces at a Crossroads: New Data Reveals Who’s Covered and What’s at Stake
- Wakely’s New Star Ratings Analysis: What’s Changing and What’s Holding Steady
- California Governor Enacts Health Care Reform Bills on Medicaid, Prior Authorization, Private Equity
- Michigan Governor Signs $81 Billion Fiscal 2026 Budget Including $29.8 Billion in Medicaid Funding
- North Carolina Hospitals Forgive $6.5 Billion in Medical Debt with Medicaid Payment Incentives
- Oregon Cancels Medicaid Reentry Initiative
- Washington Announces Updated Managed Care Rate Reductions
- CMS Issues Updated Medicare Advantage Telehealth Guidance
- Trump Announces AstraZeneca Deal to Lower Medicaid Drug Prices
In Focus
On the Horizon: Contract Year 2027 Proposed Rule Will Provide Trump Administration First Opportunity to Reshape Medicare Advantage Program
The Centers for Medicare & Medicaid Services (CMS) is preparing to release the proposed Contract Year 2027 Policy and Technical Changes to Medicare Advantage, Medicare Prescription Drug Benefit, Medicare Cost Plan, and Programs of All-Inclusive Care for the Elderly Programs. Rather than incremental tweaks, this rulemaking cycle offers CMS officials the first full opportunity to advance the Trump Administration’s policy priorities. With sweeping reforms on the horizon, Medicare Advantage (MA) plans that begin aligning their operations now will be positioned to thrive in the new environment.
These reforms arrive at a pivotal juncture for MA. Enrollment, which has climbed steadily over the past decade, is projected to decline from 34.9 million in 2025 to 34 million in 2026 as financial and regulatory pressures prompt some issuers to narrow or exit select markets. Although CMS anticipates stable average premiums and benefits next year, beneficiaries in areas with reduced competition may face fewer plan choices and marginally higher cost sharing. These market shifts are likely to influence the 2027 contract year rule.
In this article, Health Management Associates, Inc. (HMA), Medicare experts delve into the key policy areas CMS is poised to address—prior authorization reforms, coding and risk adjustment oversight, Star Ratings realignment, and expanded program integrity efforts.
Prior Authorization and Utilization Management Reforms
CMS, across multiple administrations, has viewed prior authorization (PA) as both a cost-control lever and a potential barrier to care. In the contract year 2027 policy and technical rule, CMS officials will have their first unencumbered chance to cement electronic PA standards, enforce strict turnaround timelines, and limit plan’s use of internal coverage criteria. By mandating consistent rules across the MA landscape, CMS seeks to minimize provider frustration without sacrificing utilization management.
Risk Adjustment and Coding Oversight
MA coding practices leading to elevated MA risk scores have been the subject of bipartisan concern and heightened scrutiny as these have been found to inappropriately increase federal government payments to plans. In response, the 2027 rulemaking cycle provides an opportunity for CMS officials to develop more far-reaching reforms to the MA risk adjustment model and potentially explore more transformative models that move away from reliance on Medicare fee-for-service (FFS) data. Encounter-based risk adjustment or an “inferred” CMS-driven scoring approach could narrow payment gaps and deter upcoding.
Next Phase of Star Ratings
Star Ratings will likely see the most pronounced reset under CMS’s proposed changes. Moving away from purely process measures, CMS intends to elevate health outcomes—such as fewer hospital admissions and improved functional status—and sharpen its focus on “exceptional care for all enrollees” through the Excellent Health Outcomes for All (EHO4all) reward. This framework, announced under the calendar year 2026 rate notice, revised the Health Equity Index reward. In the 2027 proposed rule, CMS could call for retiring outdated measures in favor of streamlined reporting via health IT and patient-reported outcomes. CMS has also indicated it would consider other factors for this reward program.
Oversight and Program Integrity
This rulemaking cycle affords CMS officials an opportunity to expand the agency’s oversight toolkit. Advanced analytics and AI-driven audit selection will underpin fraud, waste, and abuse detection at greater scale. Potential areas of focus include enhancing efforts to promote accuracy in MA plan payments, addressing concerns with MA coding practices, and harnessing new technology to assist CMS in its oversight and auditing functions.
Charting the Path Forward
The contract year 2027 proposed rule represents the Trump administration’s first full-cycle effort to align Medicare Advantage with its priorities. By initiating PA automation, rigorous coding compliance, outcome-driven quality enhancements, and next-generation audit preparedness now, MA plans can turn regulatory challenges into competitive advantage. Stakeholders should monitor the Office of Management and Budget’s review timetable, submit focused comments during the rulemaking window, and leverage specialized modeling support to quantify impacts. The program’s future is outcome-centered and accountability-driven. Plans that embrace this vision today will lead the market tomorrow.
Preparing for the 2027 Contract Year for Medicare Part C and D
In addition to advancing the Trump Administration’s healthcare policy priorities, market shifts are likely to influence provisions included in the 2027 contract year proposed rule.
HMA experts advise that issuers and other interested healthcare organizations consider the following potential proposals as well as the changes to help organizations prepare:
- CMS might propose to tighten standards around minimum plan offerings per county, bolster network adequacy requirements, and enhance provider directory. transparency to safeguard beneficiary access as the program evolves.
- Plans that accelerate PA digitization, embed real-time clinical decision support, and train providers on uniform criteria today will smooth their path when CMS announces the contract year 2027 final rule.
- To stay ahead, plans should launch internal coding audits, fortify provider documentation support, and pilot encounter-level data collection now.
- MA organizations must recalibrate quality programs toward these high-impact metrics, invest in digital platforms for real-time patient feedback, and forge care-management strategies that demonstrably lower acute events.
Connect with Us
HMA is closely monitoring the federal review timetable for this proposed rule. Our Medicare experts are working with healthcare organizations to prepare to submit targeted comments during the comment window, including applying specialized modeling support to quantify impacts.
The future of MA is outcome‐centered and accountability‐driven; plans that embrace this vision today will lead the market tomorrow. For details about the MA and Part D regulatory and market landscapes and approaches to position your organization for success, contact our featured experts Greg Gierer, Amy Bassano, Julie Faulhaber, and Zach Gaumer.
ACA Marketplaces at a Crossroads: New Data Reveals Who’s Covered and What’s at Stake
As we approach the end of 2025, the Affordable Care Act (ACA) Marketplaces face a pivotal moment. Enhanced Advance Premium Tax Credits (APTCs), introduced under the American Rescue Plan Act (ARPA) and extended through the Inflation Reduction Act (IRA), have driven record-breaking enrollment, with 24 million individuals now covered through the Marketplaces. Without congressional action, these subsidies will expire on December 31, 2025.
This pending policy shift makes it more urgent than ever to understand who the Marketplace serves, what enrollees receive, and how future changes could affect affordability and access.
HMA and Wakely, an HMA Company, have released a new Issue Brief that provides a comprehensive profile of Affordable Care Act Marketplace enrollees primarily based on claims data from nearly 6 million of the 24 million Marketplace enrollees. The brief answers key questions about Marketplace enrollees, including the types of health conditions they have and the types of services and prescription drugs they use.
The white paper is available on the HMA website.
Wakely’s New Star Ratings Analysis: What’s Changing and What’s Holding Steady
As Medicare Advantage and Part D plans prepare for the 2026 contract year, Wakely, an HMA Company, has published two white papers that offer critical insights into the latest developments in the Centers for Medicare & Medicaid Services’ (CMS) Star Ratings program. These analyses follow CMS’s release of the final 2026 Star Ratings, which play a pivotal role in plan performance, member retention, and bonus payments.
Why It Matters
Star Ratings reflect plan quality, member experience, and regulatory compliance. With CMS continuing to refine its methodology and cut points, understanding the nuances of these changes is essential for plans looking to maintain or improve their ratings. Wakely’s white papers provide a clear, data-driven lens into what’s new, what’s stable, and what it means for the industry.
No Major Shifts in 2026 Ratings
In the paper, Steady as They Glow: 2026 Star Ratings Show No Major Shifts, Wakely experts report that the 2026 Star Ratings show no major systemic shifts in overall scores. Wakely’s analysis finds that:
- Most plans maintained their previous ratings, with only modest movement across the board.
- CMS’s methodology updates had minimal impact on overall scores, suggesting a period of relative stability.
- The distribution of scores across contracts remains consistent with prior years, offering plans a chance to focus on incremental improvements rather than major overhauls.
A companion white paper, Pointing the Way: Summary of 2026 Star Rating Cut Points, explains the cut point adjustments that define how performance translates into Star Ratings. The analysis finds that several measures saw tightening of cut points, especially in areas like medication adherence and member experience. In addition, the paper indicates that early signals of quality improvement are emerging in certain domains, suggesting that plans are responding to CMS’s evolving expectations.
The paper offers guidance on how plans can strategically target measures most likely to influence future ratings.
Read the full papers.
HMA Roundup
California
California Governor Enacts Health Care Reform Bills on Medicaid, Prior Authorization, Private Equity. Fierce Healthcare reported on October 9, 2025, that California Governor Gavin Newsom signed a sweeping package of healthcare reforms aimed at improving access, transparency, and accountability across California’s healthcare system. Senate Bill 306 will phase out prior authorization for services with high approval rates beginning in 2028, reducing care delays and administrative burdens. Senate Bill 351, effective January 1, 2026, limits private equity and hedge fund influence over medical decision-making and bans noncompete clauses for clinicians. Assembly Bill 1312 expands hospital charity care by requiring facilities to screen uninsured and underinsured patients for discounted or free care starting July 1, 2027. Additional measures strengthen Medi-Cal access standards, improve telehealth reporting, and require medical chaperones for sensitive ultrasound procedures.
Michigan
Michigan Governor Signs $81 Billion Fiscal 2026 Budget Including $29.8 Billion in Medicaid Funding. Michigan Governor Gretchen Whitmer announced on October 7, 2025, that she has signed Michigan’s fiscal year 2026 budget, an $81 billion bipartisan plan focused on long-term infrastructure investment, tax relief, and protecting essential health and social services. The budget allocates $29.8 billion for core Medicaid services, including physical and behavioral health care, long-term services and supports, and home and community-based programs for seniors and people with disabilities. It maintains Medicaid coverage for more than 2 million individuals, funds Children’s Special Health Care Services and family health programs, and supports community behavioral health clinics, and aging services. Some key items included in the Michigan Department of Health and Human Services (MDHHS) budget are $9.3 billion for provider tax revenue that helps sustain Medicaid services, $131.75 million for substance use disorder prevention, harm reduction, treatment and recovery services through the Opioid Healing and Recovery Fund, and $5.1 million to improve access to behavioral health care.
North Carolina
North Carolina Hospitals Forgive $6.5 Billion in Medical Debt with Medicaid Payment Incentives. The Associated Press reported on October 13, 2025, that North Carolina hospitals have forgiven approximately $6.5 billion total in medical debt for 2.5 million people through a state government initiative that offers eligible hospitals extra federal Medicaid funds if they give low and middle income patients financial relief. Hospitals have also been directed to implement policies to discourage additional financial liabilities. All of about 100 eligible acute care, rural, or university-connected hospitals chose to participate in the initiative.
Oregon
Oregon Cancels Medicaid Reentry Initiative. Willamette Week reported on October 8, 2025, that the Oregon Health Authority (OHA) has cancelled its plans to implement a reentry initiative that would have provided Medicaid services to eligible incarcerated adults up to 90 days before their release. The state attributed the cancellation to limited bandwidth due to new eligibility criteria established by policies under OBBBA. OHA still plans to comply with Biden-era policies that provide Medicaid services to youth transitioning out of incarceration.
Washington
Washington Announces Updated Managed Care Rate Reductions. The Washington Health Care Authority issued on October 9, 2025, updated guidance on its managed care rate reductions that are set to begin January 1, 2026. After being directed to reduce managed care organization (MCO) rates by 1 percent in the 2025-27 biennial budget, HCA has altered the final rates for applied behavioral analysis, developmental screening, kidney dialysis, low-level mental health, hospital outlier threshold, and behavioral health non-claims benchmarking adjustment.
National
CMS Issues Updated Medicare Advantage Telehealth Guidance. The Centers for Medicare & Medicaid Services (CMS) released on October 10, 2025, updated guidance directing Medicare Advantage organizations to implement a temporary claims hold following the expiration of pandemic-era telehealth rules on October 1, 2025. In the absence of action from Congress, CMS may be unable to reimburse providers that perform certain non-covered telehealth services. Additionally, CMS notes that providers may want to consider providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.
Industry News
Trump Announces AstraZeneca Deal to Lower Medicaid Drug Prices. The New York Times reported on October 10, 2025, that President Donald Trump announced a deal with AstraZeneca to sell drugs to Medicaid at prices similar to those in Europe, following a similar agreement with Pfizer. The deals were secured after Trump threatened tariffs on imported medicines, using that leverage to push for lower prices and expanded U.S. manufacturing. In return, AstraZeneca and Pfizer received a three-year exemption from potential drug tariffs. While the White House framed the agreements as a breakthrough on affordability, experts said the impact on Medicaid spending would likely be modest, since the program already benefits from deep statutory discounts.
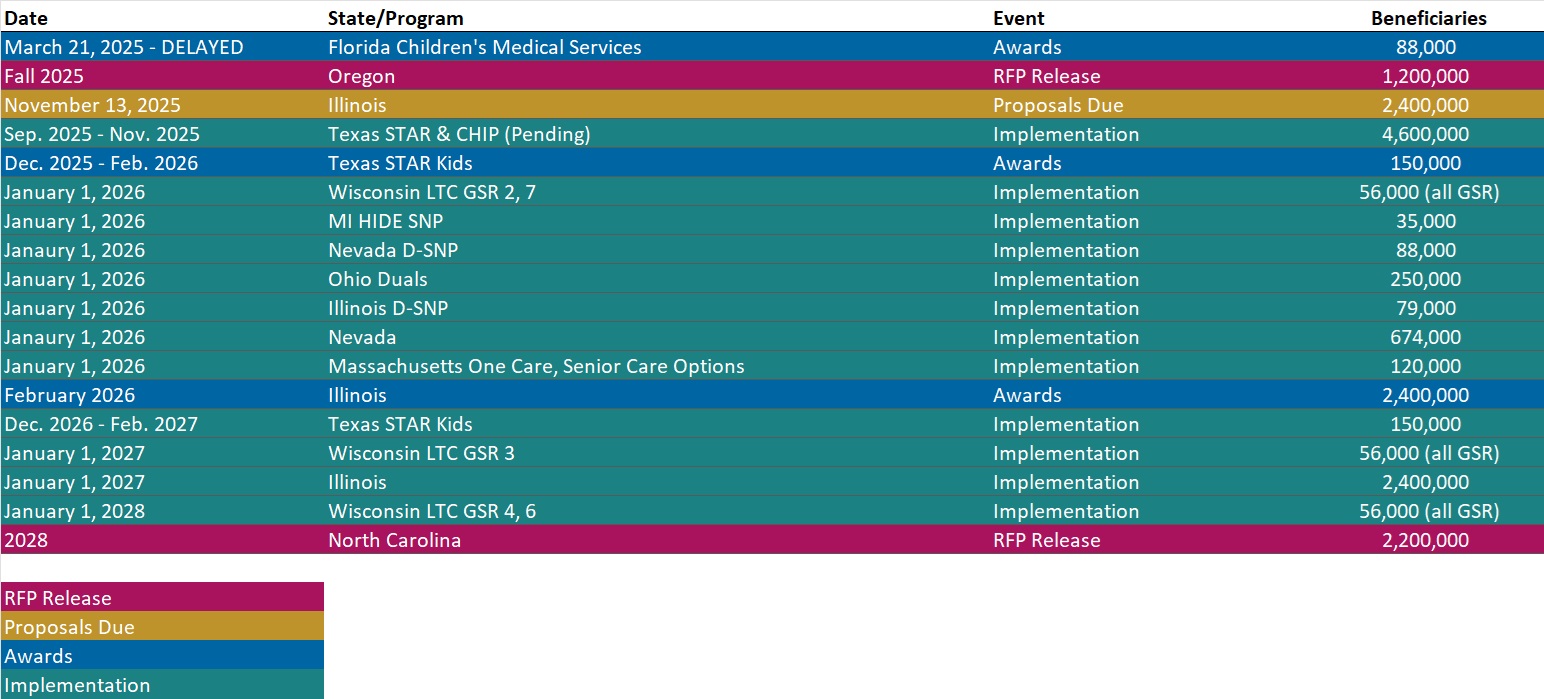
RFP Calendar
Actuaries Corner
Stable Premiums, Plan Exits: A Look at the Current State of Medicare Part D. Medicare Part D is entering 2026 with lower average premiums even as many insurers scale back or entirely exit their stand-alone plan offerings. Editor’s Note: While falling premiums may appear favorable to beneficiaries, the contraction in plan availability could limit choice and shift risk toward increased cost-sharing or narrower formularies. This underscores the need for scrutiny of benefit changes beyond just the price.
Discover other developments in the Wakely Wire here.
HMA News & Events
HMA Webinars
Medicaid 1115 Justice Involved Reentry Demonstration Opportunities: Engaging Key Stakeholders. Wednesday, October 22, 2025, 12 PM ET. This webinar will explore how states, local agencies, and community organizations can maximize Medicaid’s new 1115 demonstration authority to improve reentry outcomes for justice-involved individuals. Presenters will discuss practical strategies for assessing health and social needs, building strong collaborations with community providers, and implementing effective Medicaid enrollment processes. Attendees will gain insights into designing and operationalizing reentry programs that promote continuity of care, reduce recidivism, and support successful community reintegration. This session is ideal for State Medicaid agencies, carceral facilities, correctional healthcare companies, health plans, community-based organizations, and federally qualified health centers.
NEW THIS WEEK ON HMA INFORMATION SERVICES
(Exclusive Access for HMAIS Subscribers):
HMAIS Medicaid Market Overviews, Reports, and Data
- Updated HMA Federal Health Policy Snapshot
- New Medicaid enrollment, RFP documents, and other market intelligence resources for dozens of states
- Updated Indiana State Overview
A subscription to HMA Information Services puts a world of Medicaid information at your fingertips, dramatically simplifying market research for strategic planning in healthcare services.
If you’re interested in becoming an HMAIS subscriber, contact Andrea Maresca at [email protected].