Late 2024, HMA convened a panel of experts, including individuals with lived experience and state leaders, to spotlight the critical need for cross-system transformation. The discussion underscored the importance of centering youth and family voices, aligning placement and community-based services, and leveraging opportunities like the Family First Prevention Services Act, Medicaid waivers, and specialty managed care models. As states grapple with a behavioral health workforce crisis and insufficient foster care placements, the path forward requires bold, coordinated strategies grounded in flexibility, equity, and evidence. This brief includes key takeaways from the 2024 panel and outlines actionable insights to guide the transformation of the children’s behavioral health system.
178 Results found.

HMA helps support Section 1115 Demonstration initiatives across the country
Section 1115(a) demonstrations, informally known as 1115 waivers, are experimental, pilot, or demonstration projects that give states flexibility to design, test, and evaluate state-specific approaches to improve their healthcare programs and better serve eligible populations.
Approved by the Centers for Medicare & Medicaid Services (CMS), 1115 demonstrations provide alternative options to provide access, coverage, financing, and delivery of services under the joint federal-state funded programs Medicaid and the Children’s Health Insurance Program (CHIP). Across multiple administrations, HMA has helped state Medicaid agencies and cross-agency leaders design programs aligned with federal priorities; develop budget-neutral pathways and sustainable financing strategies; reduce operational, financial, and implementation risk; and position programs for long-term success.
Medicaid and CHIP 1115 demonstrations allow states—and their stakeholders—to test new innovations to improve the health of enrollees and advance program efficiencies. These demonstrations require careful planning, rigorous actuarial analysis, political savvy, policy knowledge, and ongoing support through the application, approval, and implementation phases. In today’s environment, 1115 programs must be responsive to the policy priorities at the federal level and grounded in solutions that work in the state. Stakeholders need aligned engagement strategies and communications plans to achieve shared goals, including monitoring that drives continuous improvements after implementation.
HMA consultants bring extensive real-world and leadership expertise from decades of working with states and federal agencies prior to joining HMA. We offer the range of services and support needed to ensure 1115 programs are financially sustainable, operationally workable, and aligned with federal and state requirements:
Strengthening healthcare safety net sustainability through financial and operational supports
Developing solutions for complex patient populations such as individuals who are justice-involved or have extensive behavioral needs including substance use disorder
Designing coverage strategies for critical social needs, such as community reintegration of vulnerable populations such as the justice involved, including when these require collaboration with agencies and programs beyond Medicaid
Supporting states in meaningful stakeholder engagement efforts, provider training and guidance, and other activities necessary for successful program implementation
Working with managed care organizations, health plans, providers, and other stakeholders to apply our expertise in implementing 1115 demonstrations
HOW HMA CAN HELP
Providing strategic and operational support to design demonstration programs
With several former state Medicaid directors and former CMS officials on staff, HMA helps states design successful new interventions to address the unique needs of their populations and ensures proposals meet CMS’ approval requirements and expectations, including aligning 1115 interventions with evolving federal priorities and objectives for the program. With HMA, states and stakeholders gain valuable insights on strategic engagement and partnerships.
Developing applications for 1115 demonstration proposals
HMA has supported a variety of 1115 initiatives in several states, including developing proposals for new, continuing, and amended 1115 demonstration programs. HMA consultants bring decades of experience in 1115 program design that covers all of the components critical to developing and operating 1115 programs – policy, actuarial and budgeting, operations, communications, project management, and IT.
Supporting federal negotiations for approval of state 1115 demonstration proposals
HMA helps states navigate the federal processes to secure approval for their 1115 initiatives. In many cases, HMA joins in active negotiations with the state agency to support federal negotiations. HMA has unique insight into federal approval parameters with former CMS officials.
Operational Support
We help stakeholders—including state agencies and their partners—manage the challenges of implementing new Medicaid or CHIP initiatives, with a focus on ensuring efficient integration and improvements in outcomes.
Evaluation and Assessment of section 1115 demonstrations
Federal regulations require evaluation of CMS-approved 1115 programs. HMA designs and conducts evaluation reports that meet federal requirements, such as hypotheses, data sources, and comparison strategies. HMA’s work on evaluation designs and evaluation reports has been held out by CMS as best practice models to other states for evaluating new policy interventions as well as for ongoing monitoring activities.
Developing materials for and supporting stakeholder engagement from design to implementation.
HMA works closely with states and their partners to engage stakeholders early in the 1115 process to ensure that communities and local organizations are involved in the planning and implementation of 1115 programs.
Project Spotlights
HMA has supported approved section 1115 demonstration programs testing new strategies for addressing substance use disorder (SUD), serious mental illness (SMI), and/or serious emotional disturbance (SED) through new flexibilities around the federal institution for mental disease (IMD) exclusion in seven states (Alabama, Colorado, Delaware, Indiana, Missouri, Ohio, and Oklahoma). In addition to initial and extension application support, HMA teams also support the evaluation and financial modeling components of 1115 demonstration development. In the last four years, we have delivered six evaluation designs, two midpoint progress assessments, two interim evaluations, and two summative evaluations approved by CMS. In general, HMA’s approved evaluation design plans use multiple evaluation methods, including a mixed-methods approach, drawing from various data sources, measures, and analytics, including quasi-experimental methods, to produce relevant and actionable study findings to conduct analyses. Additional 1115 demonstration program development activities include completing budget neutrality estimates and rate setting for new interventions proposed under demonstrations.
California is the first state in the nation to receive approval from CMS to provide detained and sentenced individuals with 90-day pre-release healthcare services and behavioral health linkages. HMA helps clients build administrative capacity, information technology, pre-release services, care management models, and Medicaid claiming infrastructure to meet their unique needs and leverage this significant state-federal demonstration opportunity. Our planning and implementation support spans the breadth of the CalAIM Justice-Involved Initiative including: the pre-release Medicaid application process, 90-day pre-release services, behavioral health links, Enhanced Care Management (ECM), and Community Supports services. In addition to California, HMA supported other states, such as Illinois and Maryland, with the design, approval, and/or implementation of justice-involved demonstrations approved by CMS. Learn more about CalAIM Justice-Involved Reentry Initiative Planning and Implementation Services.
HMA has supported multiple states in developing alternate approaches to Medicaid eligibility and enrollment tailored to their unique policy goals. For example, our consultants have worked with the Indiana Family and Social Services Administration on the program design, approval, and implementation of the Healthy Indiana Plan (HIP), Indiana’s alternative Medicaid expansion demonstration program. We also supported the Iowa Department of Health and Human services in developing the Iowa Health and Wellness Plan (IHAWP) 1115 demonstration which provides an alternative benefit design to traditional Medicaid expansion. HMA also supported the Kentucky Cabinet for Health & Family Services (CHFS) with a variety of services related to its section 1115 demonstration, Kentucky HEALTH, the first community engagement program in the nation approved by CMS.
Webinars and other resources:
- Five-part webinar series and other resources for Medicaid 1115 Waivers: creating new programs for justice-involved individuals
- Webinar replay – Navigating change: exploring the opportunities of New York’s 1115 Medicaid waiver amendment
- Behavioral health Section 1115 demonstration waivers and extensions
- The Medicaid Section 1115 demonstration landscape: past trends and anticipated shifts
Digital Quality Measurement: A Key Driver to Value
HMA Spotlight
Digital Quality Measurement: A Key Driver to Value
The healthcare industry is on the cusp of a seismic shift in how quality data are collected, analyzed and reported. Beginning in January 2027, new federal interoperability and prior authorization rules will require widespread data exchange, paving the way for full digital quality measurement (dQM) by 2030. This move toward dQM presents enormous opportunity to enhance quality outcomes, strengthen value-based arrangements, and streamline operations. However, it also requires substantial strategic, operational, and technological changes that most organizations simply cannot manage alone.
Regulatory Mandates
Organizations that delay preparing for the 2027 rule risk costly setbacks and non-compliance.
Opportunity for Transformation
dQM drives efficiency and quality improvement, supporting population health initiatives, care coordination, and value-based contracting.
Complexity and Risk
dQM implementation spans multiple departments—IT, quality improvement, analytics, legal, and more—creating a host of challenges requiring specialized expertise.
Competitive Advantage
Early adopters will have a first mover advantage. This advantage could result in revenue associated with auto-assignment, STARS bonus, value-based purchasing, reduced sanctions and fine, etc.
Why Partner with HMA?
HMA’s dQM consulting team understands the operational, clinical, and technical dimensions of transitioning to digital quality measurement. Leveraging deep expertise across health plans, provider organizations, and state and federal agencies, we help you plan, implement, and evaluate your dQM strategies at every stage.
1. Speed to Solution
- Front-Seat Knowledge: HMA, together with Leavitt Partners, an HMA Company, is actively influencing and shaping national conversations on interoperability and digital measures. Our front-line insights mean you gain rapid access to the latest best practices, regulatory updates, and strategic guidance.
- Streamlined Roadmap & Implementation: We help you develop a clear, achievable plan of action—saving you from the pitfalls of trial-and-error by fast-tracking your implementation and monitoring the results.
2. Cross-Department Coordination
- Complexity of Transformation: dQM requires alignment across IT, quality, clinical operations, and finance—often a monumental undertaking for organizations already at capacity. Robust change management & strategic planning and communications is crucial for success.
- Meet Mandated Timelines: Waiting to act can result in financial risk, stressed operations, and missed opportunities to optimize reimbursement.
- Manage Risk: Because digital quality measurement is in an emerging phase, organizations face higher levels of uncertainty. HMA mitigates risk by leveraging our extensive experience and industry partnerships.
3. Proven Expertise and Ongoing Support
- Full Project Lifecycle: From early planning and strategy development through implementation and evaluation, we stand by you every step of the way.
- Value Beyond Compliance: Our team identifies how dQM can drive broader business goals—improving population health, care coordination, and value-based contracting performance..
Ready to Transform Your Quality Measurement?
HMA’s expert consultants provide the advanced technical, business, and operational skills you need to succeed in today’s rapidly evolving regulatory landscape. Don’t let the complexity of dQM derail your strategic plans or burden your teams. With HMA as your partner, you can confidently navigate and optimize your transition to digital quality measurement.
Take the first step toward harnessing the power of digital quality measurement. Partner with HMA to position your organization for success today—and well into the future.
Contact our HMA dQM experts to discuss your organization’s goals and challenges:










Join the Call to Action to Address the Behavioral Health Workforce Crisis
The behavioral health workforce crisis, a long-standing issue worsened by the COVID-19 pandemic, threatens the ability of provider organizations to meet growing demands for behavioral health treatment services. Despite decades of efforts, challenges such as inadequate compensation, workforce shortages, lack of diversity, and high burnout persist. In fact, a 2023 survey of state Medicaid officials on behavioral health revealed that nearly every state was engaged in at least one strategy to address the workforce shortage.[1]
Since 2021, The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked to create both short and long-term solutions. Efforts have included:
- Policy papers aimed at short term solutions
- Review and crosswalk of over 400 recommendations from organizations across the country
- Creation of the Workforce Solutions JAM, begun in May 2024, a monthly webinar spreading innovation and discussing all elements of the behavioral health workforce
- Multiple convenings of technical experts and partners to discuss how to support action on the workforce
- And now a call to action.
The next step for the Workforce Solutions Partnership is to expand engagement with partners to address the workforce shortage. The Partnership believes that using the Collective Impact framework, will provide the structure to build a national strategy and cross-sector approach to shared implementation of workforce initiatives, resulting in effective and scalable solutions. We understand there are countless workforce initiatives underway across the country, many of which are demonstrating progress and innovations that can be scaled. Rather than duplicate or distract from existing efforts, the Partnership will build connections between these efforts, elevate their impact and empower emerging innovative ideas.
Initial areas of focus will include:
Community alignment: Enhancing recruitment and retention of a workforce that reflects the communities accessing behavioral health services.
Creation of efficiencies: Building a new operational and administrative model that improves access.
Technology integration: Exploring tech-enabled supports to enhance skill development and service delivery.
Career pathways and compensation: Improving access to career opportunities and using evolving payment models to increase salaries for behavioral health professionals.
The Call to Action outlines the Partnership common agenda, levers of change, and the process for developing a national platform for change. It outlines how partners can engage and is the launch of what we hope will be national action to build a sustainable workforce.
[1] Saunders, H., Guth, M., & Eckart, G. (2023). A look at strategies to address behavioral health workforce shortages: Findings from a survey of state Medicaid programs. Kaiser Family Foundation. https://www.kff.org/mental-health/issue-brief/a-look-at-strategies-to-address-behavioral-health-workforce-shortages-findings-from-a-survey-of-state-medicaid-programs/

Workforce Solutions Partnerships: Call to Action to Build a Sustainable Behavioral Health Workforce
The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked since 2021 to create both short and long-term solutions addressing the behavioral health workforce crisis. In this whitepaper, we issue a Call to Action to partners across all sectors to join us in this effort to drive pervasive change and ensure the future of behavioral health care. We need you to help us create and define the future of the workforce and envision a new system of care. This paper outlines the problem and highlights the efforts developed by our partnership, and mechanisms that can help to address the problem.
HMA Prepares Health and Human Services Assessment for the City of Watertown
On Tuesday, February 25, 2025, the Watertown City Council unanimously endorsed the recommendations of a year-long health and human services assessment prepared by HMA for the City of Watertown, Massachusetts. The report, released in November 2024, included a qualitative and quantitative assessment of the community’s health and human service needs and recommended resources to fill those gaps. As part of the project, HMA facilitated extensive community outreach and data gathering efforts in 2024 to elicit a range of community perspectives including 20 interviews, 8 focus groups, and 2 community-wide meetings resulting in 9 recommendations for organizational and program efficiencies and enhancements.
Through engagement and analysis, key community priorities emerged with a focus on programs and services relating to housing security, food security, wellness promotion, disability supports, older adult supports, communications and language access, immigrant supports, veterans’ services, public health, physical and behavioral health, and diversity, equity, and inclusion. Health and human services were considered through an intersectional lens, recognizing their overlapping qualities and characteristics that reflect how real people experience their own unique needs and seek support from a multitude of public and private supports.
Child and Teen Mental Health and the Lifting Voices initiative
Each year on March 2 we observe World Teen Mental Wellness Day, which aims to raise awareness and destigmatize mental health issues experienced by teenagers, and to expand the conversation around available resources. There is an ongoing mental health and substance use crisis in our country. Families everywhere experience difficult and challenging experiences as their loved ones are cycled in and out of a system dealing with workforce shortages and resource issues. HMA works extensively to address the opportunities and challenges inherent in our struggling behavioral health system, including substance use disorder and on child welfare and family resilience programs throughout the country. #WorldTeenMentalWellnessDay
One such program is Lifting Voices, an independent initiative developed by Heidi Arthur and Ellen Breslin, both HMA Principals, who co-founded the initiative, informed by their own family members’ experience and by their expertise in behavioral health policy and practice. As parents of children who nearly died on multiple occasions from severe behavioral health conditions, the co-founders are driven to inform the transformation of the youth behavioral healthcare system. As behavioral health professionals who found themselves struggling to navigate the many challenges facing their own children, they realized that their knowledge, desperation, and resources afforded their children access to interventions that should be available to every child and youth in need of services. Their experience of the care delivery system has also inspired their commitment to highlight the urgent improvements necessary to support struggling children and parents affected by the nation’s youth behavioral health crisis.
The co-founders published the initial Lifting Voices report in October 2023. Since then, the team has engaged multiple youth and family collaborators and state and national partners. They presented the report and their ongoing efforts at national and state conferences.
They developed a second iteration of the surveys and a website to scale the dissemination effort, with collaborators, Kelsey Engelbracht who developed the website and Sheilah Gauch who helped to develop the survey.
“We felt an imperative to lift the voices of youth and families experiencing mental health and substance use conditions,” says co-founder, Ellen Breslin.
Heidi Arthur added, “So far we’ve received just over 100 survey responses. As we reach each 100-response milestone we plan to collaborate with our network of youth and family advisors to distill key findings that we can share in order to inform improvements to the system.” They plan to release the first report in May 2025.
In February 2025, the team was invited by the Substance Abuse and Mental Health Services Administration (SAMHSA) Office of Recovery to participate in workgroups providing input into a toolkit for family and caregivers and to further define and describe SAMHSA’s framework of community-based recovery supports.
You can join national organizations and state agencies in disseminating the secure, anonymous Lifting Voices surveys by simply sharing the Lifting Voices | transform behavioral health link and inviting families and youth to participate.
Findings will be disseminated with the goal of sharing the experience that youth/young adults and parents/caregivers are having as they seek services for child and youth mental health and/or substance use.
To learn more about this project, or inquire about ways that HMA can help with other behavioral health, child welfare, or substance use disorder issues, contact a member of our behavioral health team.
Spotlight on Development of President Trump’s Children’s Health Strategy
This week, our In Focus section highlights President Trump’s Make America Healthy Again (MAHA) executive order, which is designed to address the challenges driving chronic diseases in the United States. Our article delves into the key components of the order, presents a data snapshot about the state of children’s health, and discusses implications for stakeholders seeking to prepare for and inform the transitions impacting the future of children’s health.
Presidents can use executive orders to communicate their priorities and set a framework and timelines for federal agency actions. Historically, these orders have provided strong signals for the initiatives and policy direction that federal departments and agencies will pursue. Health Management Associates (HMA), experts are monitoring the MAHA directive and several other executive orders, alongside other Trump Administration actions.
Executive Order: Making Children Healthy
On February 13, 2025, President Trump signed an executive order establishing the Make America Healthy Again Commission, chaired by US Department of Health & Human Services (HHS) Secretary Robert F. Kennedy, Jr. The commission, which builds on the Secretary’s prior work, is charged with combating “critical health challenges facing citizens, including the rising rates of mental health disorders, obesity, diabetes, and other chronic diseases.”
Initially, the commission will focus on studying and addressing childhood chronic diseases. The order directs the commission to release within 30 days an assessment that summarizes what is known about the childhood chronic disease crisis, identifies gaps in knowledge, and includes international comparisons. This report will serve as the foundation for developing a strategy to improve the health of children, which is due within 180 days of the order.
Data Snapshot: Childhood Chronic Conditions
Evaluating existing data and identifying gaps in data for children are critical initial steps toward developing a comprehensive and evidence-driven federal policy agenda. At present, 90 percent of the $4.5 trillion in annual US healthcare expenditures are used to provide services to people with chronic and mental health conditions. Many of the risk factors for developing these conditions begin in childhood and some are preventable. For example:
- Obesity affects 20 percent of children and 42 percent of adults, putting them at risk of chronic diseases such as type 2 diabetes, heart disease, and some cancers. More than one in three young adults ages 17−24 are too heavy to join the US military. The youth obesity rate from 2017−2020 was 19.7 percent, a 42 percent increase from the rate in 1999−2000. Lifestyle choices, combined with social and environmental factors like access to healthy foods and neighborhood walkability and safety can significantly reduce the risk of developing obesity.
- In 2022, diabetes and the complications associated with it accounted for $413 billion in total medical costs and lost wages in the United States. While few children have type 2 diabetes, nearly one in five adolescents (12−18 years old) have prediabetes and may develop diabetes in adulthood. Like obesity, both personal choices and adverse social and environmental factors can increase the lifetime risk of developing diabetes.
- Approximately 4.9 million children in the United States have asthma, which is incurable but can be managed. Asthma is one of the main causes for missed school days among children. Many US schools have poor indoor air quality, which can expose children to allergens, irritants, and triggers such as mold, dust, and pests. Conditions in children’s homes also can exacerbate asthma.
How Federal Programs Impact Children’s Health
Numerous federal programs directly and indirectly affect children’s health. Examples include:
- Nationally, more than 38 percent of children have Medicaid coverage, with rates exceeding 50 percent in some states and territories (e.g., Louisiana, New Mexico, Puerto Rico). Medicaid’s requirement to cover Early Periodic Screening, Diagnostic and Treatment (EPSDT) has long been the vehicle for addressing the chronic healthcare needs of children on Medicaid. For example, for children with asthma, in addition to covering medications to prevent and treat exacerbations, some states will reimburse providers for conducting home health assessments to identify and remediate triggers in the home. In addition, federal funding through both Medicaid and US Department of Education supports school nurses and school-based health centers, which can be critical resources in addressing the chronic healthcare needs of students, such as the administration of Insulin or providing inhalers to children experiencing asthma.
- To receive funding through the National School Lunch and School Breakfast programs, schools must provide meals aligned with the “meal pattern” established by US Department of Agriculture, which specifies the amount of food among various groups and an age-based maximum for calories, saturated fat, and sodium. Under current guidelines, by 2027, school meals also will be expected to comply with limits on added sugars.
- Participants in the Special Supplemental Nutrition Assistance Program for Women, Infants, and Children (WIC), which provides participants with certain foods to meet their nutritional needs, have a lower risk for preterm birth, low birthweight infants, and infant mortality.
Federal programs affect children’s home and school environment in other ways, and the health implications of those funding choices may not be explicitly recognized or prioritized. For example:
- Housing assistance programs in some cases prevent families from experiencing homelessness but may place them in living situations where exposure to environmental hazards such as mold, pests, or pollution and neighborhood factors like crime and lack of walkability may adversely affect their health.
- Some federal agriculture programs are specifically designed to make nutritious foods available (e.g., Gus Schumacher Nutrition Incentive Program, or GusNIP), while others support agriculture without specifically bringing a health lens to those programs.
Implications for Stakeholders
The President has directed that the strategy address “appropriately restructuring the Federal Government’s response to the childhood chronic disease crisis, including by ending Federal practices that exacerbate the health crisis or unsuccessfully attempt to address it, and by adding powerful new solutions that will end childhood chronic disease.” Though we do not know what the Make our Children Healthy Again Assessment and Strategy will recommend, we anticipate it will present both opportunities and risks for organizations focused on children’s health. As the commission begins its work, organizations can take the following actions:
- Consider policy opportunities: Review your organization’s strategic plan as well as your operational and policy priorities and consider how they may fit into this framework. This could be the time to suggest changes to federal grants you receive or federal regulations or requirements that negatively affect your ability to keep children healthy.
- Prepare for potential funding disruptions: It is possible that programs you rely on will have changes in scope or funding levels. Review your offerings for children with chronic conditions and identify substitutes or complements to your main priorities. Consider partners you might work with to keep work going that may not have the same level of federal support in the future.
- Be prepared to share the real-world impacts of policy changes: Begin gathering data, stories, and compelling information to share about chronic conditions affecting children that can be used in future public comment opportunities, shared with the media, and discussed with your federal, state, and local representatives. Think about how to talk about these issues in a clear and compelling way that will resonate with each of those audiences.
- Find partners and allies: As you consider the policy opportunities and risks, think about other organizations that share your interests and how you can work with them in complementary ways. It can be compelling to policymakers when stakeholders who might not naturally be aligned on other issues can unite around a specific policy area.
Connect with Us
Healthcare stakeholders with a commitment to healthy children and healthy adults have an opportunity to support the specific policies and funding opportunities that may emerge from the MAHA order. To learn more about these policy changes, the impact on your organization, and actions your organization can take, contact our one of our featured experts below.
A Closer Look at Gubernatorial Healthcare Priorities: 2025 State of the State Address Overview
This week, our In Focus section examines governors’ healthcare priorities from their 2025 State of the State addresses. This article highlights common themes in addresses delivered between January 6, 2025, and January 16, 2025, and delves into specific proposals in Georgia, Iowa, New York, and Oregon, as analyzed in the Health Management Associates (HMA), Information Services (HMAIS) interim report, 2025 State of the State Overview.
State of the States in the Current Environment
Governors use their State of the State addresses to outline their priorities for the year, giving insight into the agendas and initiatives that their executive branches may pursue independently or in collaboration with their state legislature. These priorities often are informed by the status of the state’s budget, with some governors advancing healthcare proposals that will address budget deficits and others seeking to invest in services and workforce initiatives.
Monitoring governors’ policy priorities and initiatives is especially important in 2025 given the changing federal landscape. The transition in both the administration and Congress will require state leaders to carefully consider the risks and opportunities. As detailed below, governors’ responses will unfold differently across states and markets.
Common Threads
In all, 24 governors delivered a State of the State Address between January 6, 2025, and January 16, 2025. Many gubernatorial leaders have similar areas of priority and concern, with some continuing multiyear initiatives to address unmet behavioral health needs and control healthcare costs. Table 1 identifies the themes emerging from the first group of addresses.
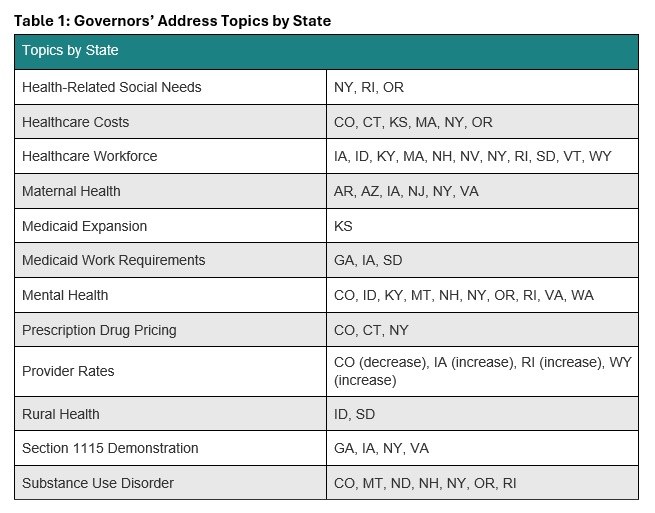
Governors also are considering possible policy changes under the new Trump Administration. For example, some governors reported that their state is looking to strengthen or add Medicaid work requirements to their programs, resuming initiatives that were initially pursued during the first Trump Administration. Though not directly related to healthcare, governors’ decisions to mirror President Trump’s Department of Government Efficiency, with Iowa as an example, could indirectly affect local programs and markets. Other states are considering the implications of possible changes to federal Medicaid funding. A deeper look into the priorities in Georgia, Iowa, New York, and Oregon follows.
Georgia
Gov. Brian Kemp delivered Georgia’s State of the State address on January 16, 2025, during which he focused his healthcare remarks on the state’s Pathways to Coverage Section 1115 demonstration. Georgia’s waiver extends Medicaid coverage to able-bodied adults who earn up to the federal poverty level if they meet certain work requirements. The governor emphasized that he intends to work with the Trump Administration to further advance innovative approaches to healthcare access.
Governor Kemp stated that his administration is making it easier to apply for Medicaid coverage and will submit an amendment to the Centers for Medicare & Medicaid Services (CMS) that would extend the Pathways demonstration for five years beyond the current expiration date of September 30, 2025. The state plans to request several changes to the demonstration, including:
- Changing the reporting requirements for qualified work activities
- Adding more activities that qualify for program eligibility
- Adding a retroactive coverage policy
- Removing premiums and Member Reports Accounts
The governor’s proposed fiscal year (FY) 2026 budget includes $324 million to fully fund projected Medicaid enrollment and utilization growth and $36 million in additional support for pharmacy benefits, including recently approved gene therapy treatments for sickle cell disease.
Iowa
Iowa Gov. Kim Reynolds delivered the Condition of the State Address on January 14, 2025, during which she called for increased Medicaid reimbursement rates for OB/GYNs and primary care physicians who provide care to people with complex pregnancy cases, as well as certified nurse midwives. The governor also said she was in favor of adding doula services as a covered Medicaid benefit. Governor Reynolds is one of several governors who have announced plans to pursue a Section 1115 demonstration for Medicaid work requirements for able-bodied adults.
Governor Reynolds’s proposed FY 2026 budget includes investing $642,000 in newly unbundled Medicaid maternal rates, and more than double investments in five existing state healthcare loan repayment programs. The governor also proposes to establish a Medicaid Graduate Medical Education enhanced payment to draw down more than $150 million in federal dollars for more residency spots in Iowa’s teaching hospitals.
New York
New York Gov. Kathy Hochul delivered her State of the State Address on January 14, 2025, at which time she also released a State of the State Book. Addressing behavioral health is one of her chief priorities, and proposals include:
- Allowing more involuntary commitments for people with severe mental illness
- Developing programs to support youth mental health through after school programs
- Expanding peer support programs
- Improving the diagnostic process for children with complex needs
- Supporting mental wellness in historically marginalized neighborhoods
- Expanding Mobile Medication Units to bring opioid treatments to underserved areas
Governor Hochul intends to expand support for the state’s healthcare safety net. This part of her agenda would provide financial assistance to struggling medical facilities and hospitals through expansion of the state’s Safety Net Transformation Program and participation in the US Food and Drug Administration’s program that allows states to import lower-cost drugs from Canada.
The governor’s proposed $252 billion budget for FY 2026 would allocate $35.4 billion for the state Health Department’s Medicaid budget—a 14 percent increase from last year. Governor Hochul plans to offset some of the spending hike with revenue from the newly approved managed care organization tax, which is expected to raise $3.7 billion to help balance the state budget over three years.
Oregon
Gov. Tina Kotek delivered Oregon’s 2025 State of the State Address on January 13, 2025. The governor has a significant focus on mental health and substance use disorder treatment, as well as housing as an HRSN. Governor Kotek wants to strengthen the behavioral health system and proposed adding new treatment beds, increasing treatment capacity, eliminating backlogs at the state’s health licensing boards to improve access to qualified counselors, improving the provider pipeline, and increasing worker retention. During her speech, the governor also called for improved frontend care coordination to decrease the overflow of people at the Oregon State Hospital.
In addition, the governor intends to work toward improving care for the civil commitment population (i.e., people who are involuntarily detained in a psychiatric hospital) by dedicating permanent supportive housing funds to expanded residences with onsite services. Governor Kotek has directed her team to develop a new intensive permanent supportive housing model to more effectively support people with serious mental health needs.
Governor Kotek’s proposed budget for the 2025−2027 biennium includes $39.6 billion for the Oregon Health Authority, representing a 10.4 percent increase from the approved budget for 2023−2025. This budget includes $29.6 billion for the state Medicaid program and $1.6 billion for the Behavioral Health Division, in addition to $732.4 million for the division from the General Fund.
Connect With Us
HMAIS has prepared a comprehensive report summarizing each State of the State Address, which is available to HMAIS subscribers. The report also examines proposed budgets, highlighting key financial commitments and allocations that underscore these priorities for the upcoming year. The first iteration of the report covers AR, AZ, CO, CT, GA, IA, ID, KS, KY, MA, MT, ND, NE, NH, NJ, NV, NY, OR, RI, SD, VA, VT, WA, and WY. The document will be updated periodically as speeches occur.
Contact our experts below for more information about the report or to connect with one of HMA’s state policy and market experts.
Major changes to Medicare Advantage and Part D proposed by CMS for 2026
This week’s In Focus section examines a comprehensive proposed rule that the Centers for Medicare & Medicaid Services (CMS) released on November 26, 2024. These highly anticipated regulations—which represent the last major Medicare regulations from the Biden Administration—include several significant and far-reaching proposals designed to strengthen plan oversight and enhance beneficiary protections for millions of Medicare beneficiaries who have coverage through Medicare Advantage and Medicare Part D plans beginning in contract year 2026. The rule also comprises proposals with fiscal and policy implications for state Medicaid programs.
Comments on the proposed rule are due by January 27, 2025, and the incoming Trump Administration could make significant changes before finalization. New administration officials may choose to delay certain provisions, scale back, or eliminate certain proposed policy changes when they finalize the regulations next year.
This article explains several of the proposed policies, considerations for healthcare stakeholders, and developments that Health Management Associates (HMA) experts will be tracking in the coming weeks.
Coverage of Anti-Obesity Medications Under Medicare Part D and Medicaid
In the proposed regulations, CMS seeks to expand coverage of anti-obesity medications (AOMs) under the Medicare Part D and Medicaid programs. Under current Medicare Part D coverage rules, medications used exclusively for weight loss are excluded from the definition of a Part D covered drug. Through the proposed change, CMS is seeking to align Medicare and Medicaid coverage policy with the prevailing medical consensus that recognizes obesity as a chronic disease.
Under the proposed reinterpretation, CMS would expand eligibility for Part D coverage of AOMs for Medicare beneficiaries with obesity. AOMs used for weight loss or chronic weight management would continue to be excluded from Part D coverage under the proposed regulation.
As it relates to Medicaid, CMS’s proposed reinterpretation would require Medicaid coverage for anti-obesity medications when used for weight loss or chronic weight management for the treatment of obesity. State Medicaid programs would continue to have discretion to use preferred drug lists and prior authorization (PA) to establish certain limitations on the coverage of these drugs, consistent with existing statutory requirements.
CMS estimates the proposal would increase federal costs by $24.8 billion as the result of expanded Part D coverage and $14.8 billion because of expanded Medicaid coverage over a 10-year period.
Key considerations: Though expanded access to innovative medications may improve access and outcomes for obese patients, these considerations may need to be balanced against the proposal’s considerable fiscal costs. In addition, key health nominees put forth by President-Elect Donald J. Trump have different views about how best to prevent and treat chronic disease, creating additional uncertainty about whether this proposed expansion will go forward.
Strengthening Prior Authorization and Utilization Management Guardrails
The proposed rule includes a series of recommendations for reforming Medicare Advantage PA, utilization management (UM), and coverage decisions, which include:
- Defining the meaning of internal coverage criteria to clarify when MA plans may apply UM
- Ensuring MA plans’ internal coverage policies are transparent and readily available to the public
- Requiring plans to inform beneficiaries of their appeal rights
- Revising the current metrics for the annual health equity analysis on the use of PA to require more detailed and granular reporting to allow CMS to determine whether MA plans disproportionately deny certain services
Key considerations: Continued scrutiny of MA plans’ PA practices and strong bipartisan support for reforms increase the likelihood that certain changes will be made to these policies within the next year.
Enhancing Medicare Plan Finder to Include Information on Plan Provider Directories
Another notable proposal would require MA plans to make provider directory data available to CMS for inclusion in Medicare Plan Finder (MPF), the online tool that allows beneficiaries to compare coverage options, including Medicare Advantage and Part D plans. At present, provider directories must be accessible on MA plans websites.
CMS seeks to enhance MPF with searchable provider information for all MA plans while requiring plans to attest to the accuracy of the provider directory data, including updating data within 30 days of receiving notification that provider information has changed. CMS would ensure compliance with this expectation by requiring plans to meet data compliance and quality checks, which will be detailed in upcoming technical guidance.
Improving Access to Behavioral Health Care
The proposed rule furthers federal policymakers’ initiatives to address the nation’s behavioral health crisis. CMS proposes to establish the following three standards to ensure that beneficiary cost sharing in Medicare Advantage is no greater than in Traditional Medicare:
- A 20 percent coinsurance or an actuarially equivalent copayment rate for mental health specialty services, psychiatric services, partial hospitalization, and outpatient substance abuse services
- No cost sharing for opioid treatment programs
- All (100 percent) of the estimated Traditional Medicare cost sharing for inpatient psychiatric services
Improve Oversight and Administration of Supplemental Benefits
MA plans may offer a variety of supplemental benefits such as vision, dental, and gym memberships, which have come under increasing scrutiny by CMS. CMS proposed several actions to reduce misuse of these benefits, including:
- Outlining proper usage by MA organizations and enrollees
- Adding disclosure rules for transparency
- Ensuring enrollees can access covered services through alternative methods
- Requiring real-time electronic links between debit cards and covered services
- Defining acceptable over-the-counter products.
Key Considerations: CMS officials in President-Elect Trump’s first administration expanded flexibility for plans to offer supplemental benefits. Incoming policy officials may seek an opportunity to fully review the Biden Administration’s proposals. Data and experience-informed comments from MA plans and stakeholders can support such discussions.
Improve Care Experience for Dual Eligibles
CMS proposed the following two new federal requirements for Dual Eligible Special Needs Plans (D-SNPs) that are applicable integrated plans (AIPs):
- AIP D-SNPs will need to have integrated member ID cards for their Medicare and Medicaid plans.
- D-SNPs will be required to conduct an integrated health risk assessment for Medicare and Medicaid, rather than separate ones for each program.
Key Considerations: These proposals further CMS’s multi-year work to advance integrated care by applying Medicare-Medicaid Plan features into D-SNP requirements. States and MA and Medicaid plans should plan for operational and policy changes if the proposals are finalized.
Formulary Inclusion and Placement of Generics and Biosimilars
CMS proposes to require Part D formularies to provide beneficiaries with broad access to generic, biosimilar, and other low-cost drugs while also ensuring that tier placement and UM practices do not limit access to these drugs as compared with more expensive brand name and reference products.
Key considerations: If finalized, the proposal would require MA-PD and Part D plans to update their approach and considerations for plan formulary development. Consumer groups and other stakeholders should consider the possibility that the proposal will improve access to lower cost products.
Other Topics in the Proposed Rule
In addition, the proposed rule calls for the following:
- Guardrails for artificial intelligence to protect access to health services, such as requiring that MA plans ensure services are provided equitably, regardless of delivery method or origin (i.e., human or automated systems)
- Changes to MA and Part D medical loss ratio (MLR) reporting to improve the meaningfulness and comparability of MLR across plan contracts
- Expanded Part D medication therapy management eligibility criteria
- Adding and updating measures addressed in this proposed rule, beginning with the 2028 Star Ratings
- Promoting community-based services and enhancing transparency of in-home service providers, including new definitions and standards for community-based organizations
- Codifying existing guidance related to implementation of the Medicare Prescription Payment Plan, which is part of the Inflation Reduction Act (IRA)
What to Watch
During the lame duck session, Congress could advance legislation related to some proposals in this rule. Specifically, PA has been an area of significant bipartisan interest, along with access to and cost of GLP-1 products. CMS will need to ensure the final MA and Part D policy and technical rule for contract year 2026 reflects approved statutory changes.
In addition, HMA is watching key appointments within the US Department of Health and Human Services, including individuals selected to lead CMS’ Medicare and Medicaid centers. These appointments will provide valuable insights on the emerging policy agenda of the incoming administration.
Connect with Us
HMA’s Medicare and Medicaid experts will continue to assess and analyze the policy and political landscape, which will determine the final policies in the MA and Part D policy and technical rule for contract year 2026. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist organizations that engage in the rulemaking process and to support implementation of final policies, including policy development, tailored analysis, and modeling capabilities, as well as quality improvement initiatives and plan benefit design.
For further analysis of the MA and Part D proposed rule and potential impact on MA and Part D plans, Medicaid programs, providers, and beneficiaries, contact our featured experts below.
Strategic Expenditure Planning: Empowering County Government Agencies to Optimize Opioid Settlement Funds
THE CLIENT
The Lake County Behavioral Health Services Department and the residents of Lake County, California.
BACKGROUND
In 2021, opioid manufacturer Janssen Pharmaceuticals along with three opioid distributors, McKesson, Amerisource Bergen, and Cardinal Health (collectively known as The Distributors) reached settlements for their roles in the opioid epidemic that amount to $26 billion. These settlements will be distributed to states that participated in the joint lawsuits. It is estimated that California will receive approximately $2.05 billion over 18 years to focus on opioid abatement activities within the state. As a participating subdivision, Lake County is set to receive a portion of California’s Abatement Fund and began receiving payments on November 15, 2022. The County will receive approximately $18 million over the course of eighteen years.
HMA was tasked with creating an expenditure plan for the opioid abatement settlement funds distributed to the Lake County Behavioral Health Services Department and the residents of Lake County. HMA facilitated community engagement to gather stakeholder feedback and align community priorities with the High Impact Abatement Activities (HIAA) and goals as defined by the California Department of Healthcare Services.
APPROACH
HMA works with state, county, and local government entities across the U.S. in collaboration with community members, engaged stakeholders, and policymakers to develop funding priorities that are designed to facilitate improvements in the quality of life of those experiencing opioid use disorder (OUD) and to prevent overdose deaths. The HMA team has worked closely with organizations in counties across the U.S. to help develop plans for OUD programs using opioid settlement funds, and does so through partnering with clients and communities, community advisory councils/boards and with local community-based organizations to co-create community engagement strategies, tools, and plans and to engage communities in the decision-making process.
For this project, HMA organized and conducted four, 4-hour, collaborative meetings with a variety of partners in Lake County, as well as analyzed the capacity, available resources, and demographic trends of the OUD population. This comprehensive data collection culminated in a final report which provides an analysis of persistent challenges, proposed actions, and desired outcomes, including identifying current efforts and best practices that are most effective in addressing OUD needs across the continuum of care (prevention, intervention, and treatment).
TESTIMONIAL
“It has been an absolute pleasure working with HMA on the Opioid Settlement Funds project. You guided us deftly through a methodical and intentional process with a clear focus on results. You have a unique ability to both diffuse and validate the tensions that typically arise whenever you bring a community together to make decisions about a big pot of money. I must admit, there was a point during the stakeholder engagement process where I was worried we might not be able to land on shared ground. At the finish line of this project I am excited and energized with a clear plan to move forward.”
Elise Jones, Director, Lake County Behavioral Health Services
RESULTS
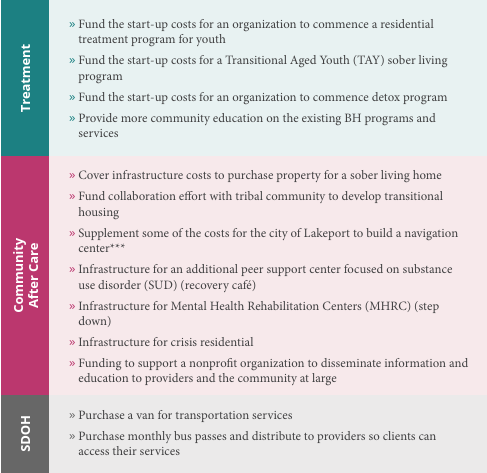
As the final deliverable, HMA developed a dynamic and actionable expenditure plan for the opioid settlement funds. Lake County was adamant that the voice of community members including, persons with lived experience, health service providers, and local partners were elevated to inform the funding priorities. The expenditure plan highlights the engagement process and input received, including the invaluable perspectives of tribal partners, older adults, children and families, and people with lived experience. The culmination of the engagement process resulted in community-wide consensus of 26 prioritized strategies, categorized into f ive themes: structural, prevention & education, treatment, aftercare & community, and social determinants of health (SDOH). The expenditure plan will serve as a manual for the use of opioid settlement funds informed not only by the state’s requirements but also by Lake County community members.
Opioid Abatement Settlement Funding Workgroup-Community Conversations Prioritized Strategies for Funding Recommendations
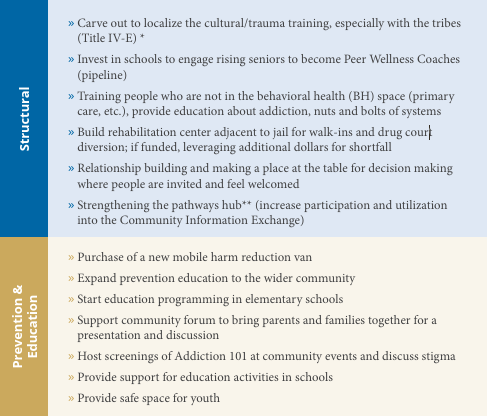
*The Title IV-E Stipend Program is the nation’s largest consortium of schools of social work and public service agencies providing support for the delivery of a specialized public child welfare curriculum and support for students committed to service in public child welfare.
**The Pathways Hub is a hub for community-based service providers to ensure the coordination of care.
***The city of Lakeport is working on creating a navigation center that will provide a variety of resources to the community, largely focusing on the unhoused population and will likely be funded through Lakeport’s opioid settlement dollars. This navigation center is still in the conceptual phase, but the intention is to serve as a hub for providers offering SUD services, housing coordination, operating mobile health clinics, and more.

Webinar Replay: How Community Care Hubs Can Enhance Family Caregiver Support Services
This webinar was held on December 3, 2024.
To better support family caregivers and the older adults who they care for, Area Agencies on Aging and other aging network agencies are creating Community Care Hubs (CCH) to address social determinants of health, integrate health and social care, and reduce care costs. In this webinar with LTSS policy experts and providers, we described the implementation of the CCH model in projects in Massachusetts and New York.
Learning Objectives:
- Describe the Community Care Hub (CCH) model for integrating health and social care
- Identify key CCH features to enhance family caregiver support services
- Illustrate the implementation of the CCH model for supporting family caregivers with projects in Massachusetts and New York
Featured Speakers:
- Kristie Kulinski, MSW, Director of Office for Network Advancement, Administration for Community Living
- Nikki Kmicinski, MS, RD, CDH, Chief Executive Officer, Western New York Integrated Care Collaborative
- Jennifer Raymond, JD, MBA, Chief Strategy Officer, AgeSpan