HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
The integration of behavioral health and medical care has emerged as a crucial method for improving health and reducing the cost of care. Integrated care offers solutions and advancements in healthcare delivery by improving access to behavioral healthcare, including scarce psychiatric resources, reducing stigma, and enhancing behavior change in everyday life.
As an emerging standard of care, policy makers, payers, and leaders are expecting organizations to develop evidence based approaches to team based care that can demonstrate health outcomes and cost savings. HMA can help your organization navigate this important culture change. Our multidisciplinary team includes clinical, finance and payment, and policy experts with hands-on experience in integrated care service delivery.
Our integration experts can help your team with:
Readiness assessment
Evidence based policy, finance, and model design
Technical assistance, training, team based care
Operational changes including billing, HIE, credentialing
Measurement based care metrics and evaluation
Cultural change and leadership
We are working with an array of clients on integration
Health plan integration
State departments & statewide implementation
Integrated delivery systems
Hospital based providers
PCMH & FQHC primary care providers
Accountable care organizations
Certified community behavioral health clinics and other BH providers
Department of corrections
For more information, contact our featured experts below.
The healthcare industry is constantly evolving and requires a workforce that is responsive and able to lead and adapt to changes. Healthcare professionals are continually asked to incorporate new services, care models, quality measures, and process improvements into daily work.
While clinical innovations and operational improvements are promising, there is growing recognition of the gap between plans to implement them and actual implementation.
HMA has extensive leadership, operational, and clinical expertise working directly with health systems, health plans, providers, foundations, community-based organizations, and associations adopt implementation science informed approaches for successful change.
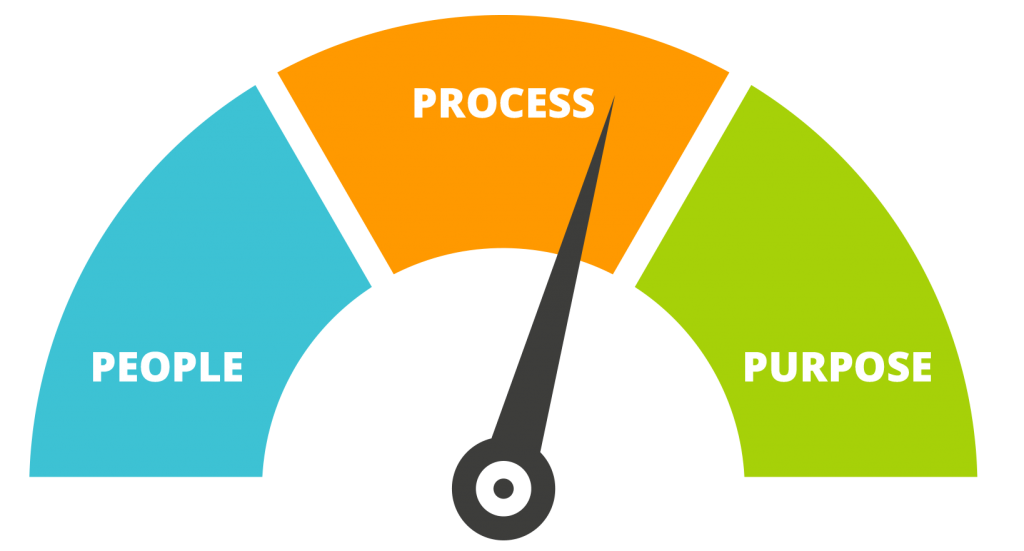
Drawing on this experience, we developed the HMA Implementation Accelerator, a leadership development framework that utilizes implementation science to address on-the-ground challenges and lead successful implementation efforts.
“The importance of leadership is noted in just about every discussion of implementation. The absence of leadership support is a well-documented barrier, and success is attributed to the presence of leadership support.”
– Active Implementation Research Network
HMA Implementation Accelerator
PEOPLE
Leadership development
Build knowledge, skills, and abilities and apply them to implementation
Change agent engagement and development
Identify formal and informal leaders to inform, support and influence engagement
Implementation approach training
Build knowledge and skills critical to successful implementation
PROCESS
Project management
Develop or enhance structures and approach to guide implementation
Continuous improvement and critical feedback
Integrate structures and practices that facilitate continuous improvement, sustain momentum, and highlight critical adaptation
Communication planning
Plan and deploy intentional, pro-active communication strategies to effectively guide and support implementation
Tool development
Identify, develop, and deploy tools that support effective implementation and create efficiencies for implementation teams
Sustainability planning
Pro-actively plan for sustainability from outset
PURPOSE
Executive sponsorship
Engage and activate sponsorships for critical support and resources
Align implementation with mission
Connect implementation efforts to a larger “why” in alignment with mission
What’s included
Conceptual framework to guide implementation process
Strategies to develop effective sponsorship at the executive or senior leadership level to mitigate barriers and resource effort
Leadership skill development at the level of implementation
Processes to enhance effective ownership and commitment at all levels
Prioritization of change initiatives
Clear accountability of actions in implementation
Continuous quality improvement as part of implementation
Sustainability planning from the start
Research shows that successful leadership development occurs when the learning can be directly applied to active work processes, which aligns with how adults learn most effectively.
Through the Implementation Accelerator, we use a combination of interactive training, peer learning, and coaching to support hands-on learning. The integration of leadership development and implementation science provides a robust opportunity to develop and sustain leadership skills and develop an organizational methodology to guide both current and future implementation efforts.
For more information, contact our featured experts below.
HMA’s team of over 50 behavioral health experts have direct experience in behavioral health policy, clinical program design and delivery, quality improvement and financing. Our breadth of expertise, including authors of NCQA’s Behavioral Health Quality Framework to Promote Joint Accountability, positions us well to support the design, delivery and payment of high quality behavioral health care.
We help clients demonstrate the value of their behavioral health care through:
Accreditation Readiness
Meet accreditation standards and demonstrate compliance
Analyze and use behavioral health-specific HEDIS, CAHPS/ECHO, HOS, ASAM/CARF to inform QI
Use key data sources to drive performance improvement plans
Use of Behavioral Health Quality Tools
Behavioral health network adequacy and equitable access
Integration of behavioral health, physical health and social needs
Measurement-based care
Patient outcomes
Cohesive Strategy Development
Behavioral health quality strategy planning aligned with organizational mission and vision
Standardized performance metrics
Value-based care and payment incentives
Pragmatic regulatory tools and policies
HMA is positioned to support
State and municipal departments of health and public health
Health plans & Managed Care Organizations
Health systems
Provider organizations
Community-based organizations
Certified community behavioral health clinics
Correctional health
Accreditation Readiness
Meet accreditation standards and demonstrate compliance
Analyze and use behavioral health-specific HEDIS, CAHPS/ECHO, HOS, ASAM/CARF to inform QI
Use key data sources to drive performance improvement plans
Use of Behavioral Health Quality Tools
Behavioral health network adequacy and equitable access
Integration of behavioral health, physical health and social needs
Measurement-based care
Patient outcomes
Cohesive Behavioral Health Quality Strategy Development
Behavioral health quality strategy planning aligned with organizational mission and vision
Standardized performance metrics
Value-based care and payment incentives
Pragmatic regulatory tools and policies
HMA is positioned to support
State and municipal departments of health and public health
Health plans & Managed Care Organizations
Health systems
Provider organizations
Community-based organizations
Certified community behavioral health clinics
Correctional health
For more information, contact our featured experts below.
The current youth behavioral health system is under-resourced, underfunded and often not well coordinated. Historic approaches that minimally adapt adult models to children and youth have led to insufficient child and youth specific strategic design of effective systems. Recent investments and policies offer a tremendous opportunity to redesign strategies, payment, and the delivery system to enhance access and achieve better outcomes, equity, and satisfaction of children and families. Health Management Associates (HMA) understand the levers and impacts across the system from state and local policy makers to payers, providers, schools, and communities. Our multidisciplinary teams will partner with you to identify challenges and solutions to advance and sustain the system of care.
What Makes HMA Unique?
HMA’s cross sectoral, multidisciplinary team is comprised of more than 20 dedicated children and youth behavioral health experts with rich backgrounds in government, community-based providers and payers. Our approach includes a deep understanding of policy, clinical, operations and fiscal systems, providing our clients with fundamental tools to design and implement sustainable solutions.
Our expertise spans multiple specialty areas impacted by children’s behavioral health:
Juvenile justice and justice-involved
Child welfare and foster care
Children’s behavioral health – primary care and social services, children with serious behavioral health issues (SMI, including co-occurring issues)
Youth crisis and mobile services, crisis stabilization unit design (CSU) services
School-based wellness centers, community schools
Certified community behavioral health clinics (CCBHCs)
Suicide prevention
State policy and system redesign, evidence-based practices and strategic planning including the intersection of Medicaid and child welfare
Telehealth for children and adolescents
Tech-enabled care
Mental health first aid
Our team is advancing the design, integration, and quality of children’s behavioral health across states and the continuum of care.
Examples of our work include:
Policy and system design for behavioral health services, foster care, and the intersection of Medicaid and child welfare
Maternal and child health programing and 2Gen approaches
Managed Care Organizations (MCO) reviews, strategy ad program design
Health system emergency department boarding and health system and community intervention design
Mobile Crisis Response (MCR) design and implementation
Implementation of school-based wellness centers and building connections to the health system
Services across the healthcare spectrum.
With a deep understanding of current and emerging shifts in care and policy, our behavioral health consultants are well equipped to provide specialized services for a range of clients.
Mental health and substance use treatment organizations struggle to meet the increase in demand for services, due in large part to a national workforce shortage. This challenge has been exacerbated due to the Covid-19 pandemic. Demand for behavioral health organizations’ services has continued to increase. At the same time, organizations are having trouble recruiting and retaining employees, and patient waitlists continue to grow. Competition for behavioral health workforce has only grown with new opportunities in telehealth and the entrance of private equity into the behavioral health market. The safety net providers are the most impacted and often have the least flexibility to address underlying factors leading to the shortages in large part due to regulation and administrative burden and underfunded payment models.
HMA, in partnership with the National Council for Mental Wellbeing (NatCon), developed a series of issue briefs outlining state policy and provider steps that can help to address the critical shortage.
HMA is also working with NatCon and the College for Behavioral Health Leadership (CBHL) to engage national partners using a collective impact framework to provide backbone support for organizations to work together in a more structured and action-oriented approach and to leverage various implementers (policy, regulatory, payers, providers, educators, etc.) to move recommendations to action.
Behavioral Health Workforce is a National Crisis: Immediate Policy Actions for States
HMA can help state policy makers and provider organizations with workforce support and problem solving, workforce assessment, strategy and policy design.
Our team of experts includes clinicians with on-the-ground experience as well as previous policy makers. We’ve worked within the certified community behavioral health clinic (CCBHC) model and provide technical assistance to organizations planning for its adoption. We have experience in extending it beyond the demonstration utilizing Medicaid state plan amendments (SPA) or 1115 waivers to enhance the workforce.
HMA capabilities
Identifying effective workforce strategies including training and maximizing of multi-disciplinary teams (e.g., peers, behavioral health providers, nurses, licensed health care providers).
Policy and system design for behavioral health services and workforce expansion
Managed Care Organizations (MCO) strategy and program design as well as strategies to enhance the provider network
Conducting certified community behavioral health clinic (CCBHC) readiness and implementation support.
Maximizing virtual and technology interventions.
Convening stakeholders and building partnerships across sectors.
HMA is positioned to support
State Medicaid agencies
State and local departments of health, public health, behavioral health, and child welfare
Health plans & Managed Care Organizations
Hospitals & health systems
Provider organizations
Community-based organizations
Foundations & advocacy organizations
Certified community behavioral health clinics
School-based behavioral health
Correctional health & juvenile justice systems
For more information, contact our featured experts below.
With the planning and implementation of 988 and mobile crisis teams, as well as co-responder models, state policy makers are working rapidly to advance effective approaches to systemically and effectively address the needs of individuals and families who are experiencing behavioral health crises.
Central to effective implementation is attention to specific community needs. States are working to partner with local communities to build capacity, leverage the knowledge and expertise of local partners, and gain an understanding of how new benefits and system changes fit into existing community frameworks. This local approach is particularly important for rural and frontier communities, and for tailoring models to meet specific priority populations’ needs, while building trust and ensuring crisis services are grounded in equitable access and culturally responsive care.
With more than 25 years of crisis system development, HMA colleagues stand ready to support crisis system community partners in advancing their crisis systems and services.
With our finger on the pulse of the science-backed research and approaches necessary to create integrated and comprehensive systems, we can help identify barriers and explore and implement solutions.
Our HMA crisis system team supports community partners with:
Partnership development
Stakeholder engagement
Crisis system needs assessment – strengths and gaps analysis
Program design and implementation
Crisis service development
Cross-system protocols
Cost modeling and sustainable reimbursement approaches
Distilling and meeting regulations
For more information, contact our featured expert below.
A significant percentage of individuals in American jails and prisons have a substance use disorder (SUD), with those with opioid use disorder (OUD) at especially high risk of death due to overdose upon release from incarceration.1 At the same time, overdose deaths during incarceration continue to increase.2,3
Medications for opioid use disorder (MOUD) and medication assisted treatment (MAT) programs reduce in-jail overdose death by 50% and the risk of overdose death after release by 60%. MAT programs also redress substantial racial and ethnic health disparities4. Despite these proven benefits, most incarcerated Americans do not have access to this treatment. Barriers to MAT implementation include lack of resources such as money, trained staff, and leadership; stigma toward both SUD and MOUD; and limited system ability to support adaptive change.
KEY MODEL ELEMENTS AND PROMISING RESULTS
Health Management Associates (HMA), a national research and consulting firm focusing on publicly funded healthcare, developed a MAT implementation support model working with dozens of jails and prisons across the United States, rapidly scaling access to MOUD/MAT during incarceration. This implementation support model fosters both technical and adaptive change using a learning collaborative structure and adult-learning theory. The model also acknowledges the unique environment of each jail and prison and the challenges of providing healthcare services for a complex condition like OUD in a correctional setting. This model program is straightforward, documented, proven, and readily replicated.
The model provides participating jail and prisons teams with access to robust individualized technical assistance and coaching; peer-to-peer support and learning; training; and collaborative educational sessions. This approach recognizes that multidisciplinary teams inclusive of custody/security staff; medical personnel; behavioral health providers; and others must be convened and supported as a cohesive unit to effectively implement MOUD and MAT programs in jails, prisons, and the justice and addiction ecosystems. This ecosystem view incorporates the critical partners and pathways outside the jail and prison to support effective re-entry to the community following incarceration to support recovery. A change management and continuous quality improvement framework is foundational to the model.
In the California, Illinois and Michigan county jail team learning collaboratives, county teams receive implementation grants or stipends. Over the course of the projects these amounts have ranged from $15,000 to over $100,000 per county, which were included in the project budget from the funding source (State Opioid Response in CA and IL; state general funds in CA). Offering this “seed money” serves as an incentive to help counties engage in the learning collaborative. HMA has managed all aspects of these implementation grants/stipends.
Evaluation
Collection and analysis of data informs ongoing technical assistance and demonstrates the rapid scaling and positive impact of the program. In the state learning collaborative programs, deidentified data is collected from county jail teams and analyzed and compiled to reflect trends and progress in the implementation effort. Where HMA supports state departments of correction with MOUD and MAT implementation, HMA assists the prison system with identifying and using key data points to inform a continuous quality improvement process.
Funding
The MOUD and MAT county jail implementation model was initiated in 2018 in California’s MAT in Jails and Drug Courts program with demonstrated impact for expanding access to MAT in the state’s county jails. The project was funded with federal State Opioid Response dollars administered by the California Department of Health Care Services (DHCS) through September 2022. The California legislature approved state general funds to support continuation of the program from October 2022 through June 2025.
Illinois’ Department of Health Services Substance Use Prevention and Recovery (SUPR) sponsored implementation of that state’s learning collaborative beginning in 2021 with federal State Opioid Response Dollars. It is currently funded through June 2024 with plans to extend the learning collaborative under a new SOR funding cycle.
Michigan Department of Health and Human Services elected to implement the county jail learning collaborative in late 2023, funding it with state opioid settlement funds for continuation through November 2026.
HealthCare Access Maryland in support of the Maryland Governor’s Office of Crime Prevention, Youth, and Victim Services deployed this model for a limited three-month period with HMA to increase access to MOUD for incarcerated persons. The impetus for this project was the OUD Examinations and Treatment Act, which requires local jails/jurisdictions in Maryland to offer all forms of MOUD.
Michigan Department of Corrections has engaged HMA for years as its contracted third-party health care evaluator. HMA supported the DOC’s MAT implementation across multiple sites in the Michigan prison system with state general funds from 2020-2022.
HMA supported the Alaska Department of Corrections with widescale MAT implementation under a contract through state general funds 2022-2023.
RESULTS
HMA’s successful model incorporates strategies that overcome typical barriers to MOUD/MAT implementation in corrections settings.
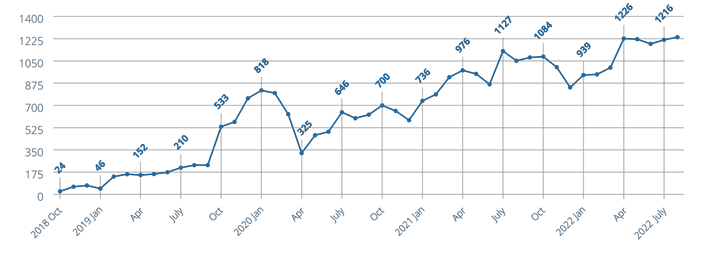
In the California learning collaborative, HMA has engaged 41 county jails over four years resulting in 35,000 person-months5 of individuals on MAT with counties participating representing almost 90 percent of the state’s total population.
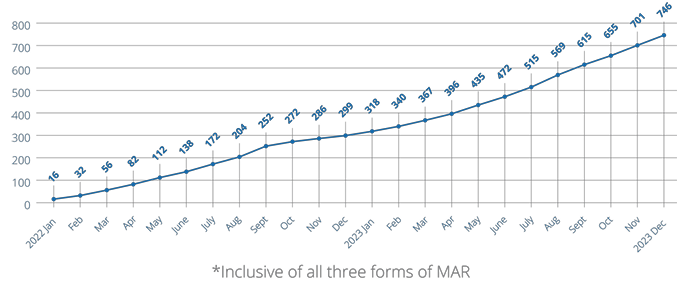
In the Illinois learning collaborative, HMA has engaged 28 counties over three years resulting in over 720 unique individuals receiving MAT in jails with participating counties representing 64 percent of the state’s population (Cook County is excluded because of an evolved MAT program prior to inception of Illinois’ county learning collaborative).
Figure 1. Running total of unique individuals who have received MAR in Jail in Illinois from inception of data collection from counties through December 2023. (MAR is medication assisted recovery – the term used for medication assisted treatment in Illinois.)
Figure 2. Running total of person-months individuals who have received MAT in jail in California participating jails from program inception through August 2022
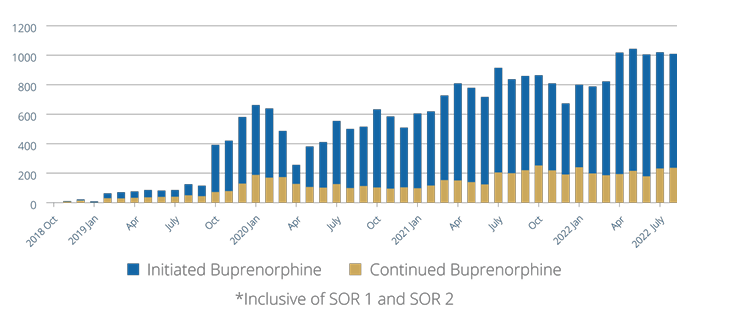
Figure 3. Running total of person-months individuals were initiated or continued on buprenorphine in California participating jails from program inception through August 2022
STRATEGY/APPROACH/INTERVENTIONS
HMA coaches and subject matter experts (SMEs) understand and respond to the unique regulatory oversight, policies, and procedures in jail and prison operations, requiring customized approaches to introduce and expand MOUD and MAT access. Both adaptive and technical change strategies are deployed to assist jails and prisons in changing their culture and operations to treat SUD like other chronic, treatable diseases. HMA coaches and SMEs stay deeply involved with implementation teams to initiate and support change over time.
County jail teams in the learning collaborative and DOC site teams are assigned an HMA coach who understands and supports their individualized operations, resource capacity, and goals. The coach convenes an in person-team meeting and initial facility walk-through to jump start the initiative and inform ongoing team implementation goals and activities. The coach assists the team in establishing and executing goals and action steps that align with the overarching goals of the learning collaborative or DOC system.
All county teams are regularly convened for collaborative learning sessions to support their implementation plan on an ongoing basis. These sessions include fundamental information on MAT/MOUD and related components of evidencebased SUD treatment in corrections settings. Coaches identify challenges and barriers at their sites and these themes inform sessions at additional learning collaborative convenings. These identified themes are also targeted with training and hands-on coaching support (e.g., biases against MAT among providers and custody staff; custody concerns about diversion of medications; payment mechanisms for the medications; and sufficient staff capacity to offer the treatment).
Critical elements of the change effort include:
Improved SUD screening, assessment, treatment options, and planning to include at least two forms of MAT are core themes and goals of the learning collaborative. This messaging and expectation accelerate implementation by “setting a bar” for teams’ efforts while providing them with individualized assistance to overcome challenges in meeting their goals.
Engagement across the treatment ecosystem including advisors from state associations of counties, sheriff departments, treatment providers, and the state prison system connects the counties with emerging policy and best practices from their professional peers.
Multidisciplinary teams: MAT in jails and drug courts requires an integrated approach inclusive of medical and behavioral health care staff, custody/security and other justice professionals, and county providers and leadership.
This implementation model drives rapid, systemic change that would likely not be possible with individual site efforts. Scaling is accelerated by the learning collaborative model in which barriers that are identified by multiple county or DOC site teams, such as regulations for methadone access to incarcerated individuals or practice of a healthcare vendor serving multiple sites, are addressed at the levels of state policy or corporate leadership and addressed in group learning opportunities.
Lessons Learned
The approach needs to be tailored to each jail and county – and for departments of correction, each DOC site – who have resources, concerns, and goals unique to them. For example, a DOC reception center will have different security and programming requirements and workflows than a general detention center. A rural county with an average daily population of 15 and intermittent nursing and provider access has different resources than a suburban jail with an average daily population of 500. The technical assistance must incorporate this understanding and meet each site where they are to be effective.
The aim – improved SUD treatment systemwide including transitions when individuals enter the corrections system and again at release – needs to be addressed as a countywide problem that needs a comprehensive ecosystem solution. Or, in the cases of departments of corrections, system and statewide perspective and strategies are required.
Implementation of MAT in jails should be sponsored by the sheriff, and key partners from probation, jail custody, jail healthcare, drug courts, local county drug treatment programs, and the county administrator’s office must be included in planning and implementation. Implementation of MAT in departments of corrections must be endorsed and actively supported by the highest levels of leadership in the system and at each prison location.
Do not underestimate the prevalence and impact of stigma. There is an ongoing need for broader education about substance use disorders and treatment including about MAT and MOUD. All stakeholders and those impacted by opioid use disorder need to understand that substance use disorder is a chronic brain-based disease and that MAT/MOUD is effective treatment – not use of a substance that is problematic, i.e. “MAT is just replacing a drug with another drug.”
It is important to build supportable, sustainable implementation plans. If teams are not given sufficient support and opportunity to evolve in their understanding and development of the implementation program they may fail. At the same time a sense of urgency is important because people are dying due to lack of access to needed treatment.
ABOUT HMA
HMA is a leading independent research and consulting firm with more than 500 consultants with expertise across all domains of publicly funded healthcare and human services. HMA has distinguished itself from other consulting companies with our decades-long tradition of hiring senior-level policymakers, healthcare system leaders, and other experts with hands-on experience.
1 National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services.
Health Management Associates (HMA) is a national leader in supporting states with the design, development, negotiation and implementation of Section 1115 demonstration waivers and waiver extensions. HMA has assisted more than 20 Medicaid departments directly with their state plan amendments, waivers, and other demonstration projects – and most recently supported Alaska, Colorado, Delaware, Indiana, Missouri, and Oklahoma.
HMA’s behavioral health team is currently working with multiple Medicaid agencies on the development of substance use disorder (SUD), serious mental illness (SMI), and serious emotional disturbance (SED) specific 1115 waivers.
We pair our behavioral health and Medicaid subject matter experts to support states with:
Developing and applying for SMI/SED and SUD Section 1115 demonstration waivers.
Providing an assessment of the requirements under the Section 1115 demonstration waiver and Medicaid managed care “in lieu of” authorities, including requirements for average length of stay, provider oversight, and monitoring, as well as other considerations.
Reviewing managed care contract requirements and providing applicable Medicaid managed care contract language for states that are utilizing “in lieu of” authority to provide reimbursement for inpatient or residential stays in IMDs.
Technical assistance with developing administrative infrastructure to monitor utilization, including adherence to length of stay requirements under the waiver and “in lieu of” options. CMS’ SMI Section 1115 demonstration waiver guidance prohibits states from receiving Federal Financial Participation (FFP) for any IMD stays that exceed 60 days. In cases where states do not meet this metric, CMS can reduce this maximum length of stay (LOS) to 45 days or less. HMA understands it is important for states to have utilization management (UM) strategies in place to identify these instances and minimize the state’s financial risk, and can therefore provide examples of state UM strategies, as well as incentives to manage inpatient and residential LOS while maintaining access to medically necessary services.
Supporting design of data capture and reporting functions for meeting wavier requirements.
Serving as the independent evaluator for approved SUD and/or SMI/SED 1115 waiver demonstrations.
For more information, contact our featured experts below.
This week our In Focus section reviews President Joseph R. Biden’s 2023 State of the Union Address (SOTU) to Congress. The President highlighted specific actions that Congress, and the Administration have taken over the last two years to advance his health care priorities.
During his first SOTU address in 2022, President Biden announced the creation of a “Unity Agenda”, which included priority policy areas with potential for bi-partisan support. The President highlighted several steps the Administration has taken to advance the “Unity Agenda” including:
The bipartisan effort to enact the Mainstreaming Addiction Treatment (MAT) Act, which removed the federal requirement for practitioners to have a waiver (known as the X-waiver) to prescribe medications, like buprenorphine, for the treatment of opioid use disorder
The Cancer Moonshot announcements for almost 30 new programs, policies, and resources to close the screening gap, tackle environmental exposure, decrease preventable cancers, advance cutting-edge research, support patients and caregivers, and more.
Addressing mental health needs through the expansion of Certified Community Behavioral Health Clinics and launch of the 988-suicide prevention hotline.
In his SOTU and accompanying White House materials, the President also proposed new policies and initiatives to further advance his health care agenda. These actions include a combination of issues that would require Congressional approval as well as actions regulatory agencies can already advance. Congress and the Administration are expected to build on previous bipartisan achievements to tackle the nation’s dual crises with addiction and mental health.
Notably, the policies outlined in the SOTU foreshadow an active regulatory agenda over the next 18 months as the Administration seeks to solidify key aspects of the President’s health care agenda ahead of the next Presidential election.
The Administration’s planned actions include the following:
Opioids
Calling on Congress to pass legislation to permanently schedule all illicitly produced fentanyl-related substances into Schedule I.
SAMHSA will provide enhanced technical assistance to states who have existing State Opioid Response funds, and will host peer learning forums, national policy academies, and convenings with organizations distributing naloxone beginning this spring.
By this summer, the Federal Bureau of Prisons will ensure that each of their 122 facilities are equipped and trained to provide in-house medication-assisted treatment (MAT).
This spring CMS will provide guidance to states on the use of federal Medicaid funding to provide health care services—including treatment for people with substance use disorder—to individuals in state and local jails and prisons prior to their release. California is the first state to receive approval for a similar initiative.
Mental Health
CDC plans to launch a new campaign to provide a hub of mental health and resiliency resources to health care organizations in better supporting their workforce.
The Department of Education (ED) will announce more than $280 million in grants to increase the number of mental health care professionals in high-need districts and strengthen the school-based mental health profession pipeline.
HHS and ED will issue guidance and propose a rule to make it easier for schools to provide health care to students and more easily bill Medicaid for these services.
The Administration is scheduled to propose new mental health parity rules this spring.
HHS will improve the capacity of the 988 Lifeline by investing in an expansion of the crisis care workforce; scaling mobile crisis intervention services; and developing additional guidance on best practices in crisis response.
HHS also plans to promote interstate license reciprocity for delivery of mental health services across state lines.
HHS intends to increase funding to recruit future mental health professionals from Historically Black Colleges and Universities and to expand the Minority Fellowship Program.
The Department of Veterans Affairs (VA), working with HHS and Defense, will launch a program for states, territories, Tribes and Tribal organizations to develop and implement proposals to reduce suicides in the military and among veterans.
VA will also increase the number of peer specialists working across VA medical centers to meet mental health needs
Cancer Moonshot
The President called on Congress to reauthorize the National Cancer Act to overhaul cancer research and to extend the funding for biomedical research established in the 21st Century Cures Act.
The Administration will take steps to ensure that patient navigation services are covered by insurance. This could require legislation depending on which type on insurance an individual has.
Health care costs
Urging Congress to pass legislation to cap insulin prices in all health care markets. Expanding the $35 insulin cap to commercial markets will require the 60 votes in the Senate.
Home and community services
Working with Congress to approve legislation to ensure seniors and people with disabilities can access home care services and to provide support to caregivers.
HMA and HMA companies are closely monitoring these federal policy developments. We can assist healthcare stakeholders in responding to the immediate opportunities and challenges that arise and contextualize these actions for longer-term strategic business and operational decisions.
If you have questions about these or other federal policy issues and how they will impact your organization, please contact our experts below.
At HMA, our subject matter experts get questions every day from people working in state agencies, counties, health plans and provider groups about how to “right size” the behavioral health continuum to obtain equitable access for growing behavioral health demand. From legislatures to providers, improving access to mental health services is critical to improving overall health outcomes. It is time for behavioral health to create a specific definition of network adequacy that accounts for the complexity and nuance of access to mental health and substance use care. It is time to identify and define the factors that lead to “adequate” provider capacity, to ensure that the right level of care is available to individuals when they need care. Network adequacy in behavioral health needs an overhaul to meet the complexity that is driving access challenges.
Together let’s re-define what “adequate” means in behavioral health to ensure we build systems that meet the needs of communities. At HMA’s quality conference on March 6 in Chicago, the “Developing a Behavioral Health Quality Strategy” working session will engage participants in an in-depth discussion on identifying factors to inform a more accurate definition of behavioral health network adequacy. Speakers will outline some of the core challenges in network adequacy and innovations they have used. Attendees will work collaboratively in a structured exercise on three knotty challenges within network adequacy to identify factors that could improve measurement for states, plans and providers. The goal is for participants to walk away with tangible actions they can implement in their work on behavioral health access.
Please join our HMA experts and our featured panelists:
And follow #HMAtalksQuality on Twitter and LinkedIn for more updates on behavioral health quality efforts throughout the year. View the full agenda and register for HMA’s first annual quality conference on March 6 in Chicago. Registration closes on February 21, 2023.