April 16, 2025
This week's roundup:
- In Focus: FY 2026 Medicare Hospital Inpatient Proposed Regulation Signals Several Changes Lie Ahead for the Hospital Industry and Beneficiaries

- In Focus: The Medicare Advantage VBID Program Is Ending: Here’s What All Plans Can Do to Prepare for What’s Next
- Arizona Submits Section 1115 Demonstration Amendment for Medicaid Work Requirements, Lifetime Coverage Limits
- Arkansas Legislature Advances Bill to Increase ARHOME Medicaid Expansion MLR, Add Work Requirements
- California Governor Signs $2.8 Billion Bill to Close Medi-Cal Gap, Maintain Coverage Through June
- Indiana Governor Signs Multiple Executive Orders Aligned with Make America Healthy Again Initiative
- Iowa Submits Section 1115 Demonstration Application to Impose Medicaid Expansion Work Requirements
- Oregon Submits Extension Request for SUD Section 1115 Demonstration
- Trump Signs Executive Order on Drug Price Negotiations, Hospital Payments
- CMS Releases FY 2026 SNF Payment Proposed Rule with 2.8 Percent Rate Increase
- CMS Issues RFI on Potential Changes to Medicare Regulations
- More News Here
In Focus
FY 2026 Medicare Hospital Inpatient Proposed Regulation Signals Several Changes Lie Ahead for the Hospital Industry and Beneficiaries
This week, our In Focus section reviews the policy changes that the Centers for Medicare & Medicaid Services (CMS) proposes to make in the Fiscal Year (FY) 2026 Medicare Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Acute Care Hospital (LTCH) Proposed Rule (CMS-1833-P). The IPPS proposed rule, released April 11, 2025, includes several important policy changes that will alter hospital margins and change administrative procedures, beginning as soon as October 1, 2025.
Key Provisions of the FY 2026 Hospital IPPS and LTCH Proposed Rule
For FY 2026, CMS proposes to modify several hospital inpatient payment policies. We highlight and interpret six of these proposed policies that may be among the most impactful for Medicare beneficiaries, hospitals and health systems, payers, and manufacturers, as follows:
- Annual inpatient market basket update
- Labor share reduction
- Medicare Advantage (MA) data integration in measuring hospital readmissions
- New Technology Add-on Payment (NTAP) program growth
- Transforming Episode Accountability Model (TEAM) modifications
- Uncompensated care payment increase for disproportionate share hospitals (DSHs)
Annual Inpatient Market Basket Update
Proposed Rule: CMS’s FY 2026 Medicare IPPS Proposed Rule will increase payments to acute care hospitals overall by 2.4 percent from FY 2025, amounting to an estimated $4 billion increase in reimbursement. This update is based on a hospital market basket increase of 3.2 percent and a 0.8 percent reduction for total factor productivity.
HMA Analysis: CMS’s 2.4 percent increase results from the estimated rate of increase in the cost of a standard basket of hospital goods—the hospital market basket. For beneficiaries, this payment increase will lead to a slightly higher standard Medicare inpatient deductible and an increase in out-of-pocket costs. For hospitals and health systems, payers, and manufacturers, the proposed payment increase (2.4 percent) is consistent with economy-wide inflation over the past year (2.4 percent) and below the amount that MA plans will receive for 2026 (5 percent).[1], [2] Although the published payment update for FY 2026 is 2.4 percent, other policy changes result in the average change in inpatient payments totaling slightly more than 3 percent. We anticipate the proposed 2.4 percent increase will increase somewhat by the time CMS finalizes these rates later in the year.
Labor Share Reduction
Proposed Rule: CMS proposes to modify the hospital labor share used to reimburse hospitals for inpatient services. Using 2023 hospital cost report data CMS proposed a national labor‑related share of 66.0 percent, a decrease from the labor share of 67.6 percent.
HMA Analysis: Every five years, CMS recalculates the hospital market basket and the hospital labor share using updated cost data from the hospital cost reports. For FY 2026, CMS conducted its routine rebasing calculation using 2023 cost report data, replacing the 2018 cost data currently used. As a result, CMS calculated that the cost of labor accounts for a slightly smaller share of total hospital costs in 2023 than in 2018. The labor share is used within the IPPS to identify the proportion of payments that are affected by the hospital wage index in an effort to adjust payments for geographic variation in labor costs. The consequence of a lower hospital labor share is that a slightly smaller share of hospital inpatient payments will be adjusted by the hospital wage index. The subtle impact of this change is that hospitals with higher wage index values may experience reductions in payment. Further, this downward revision of the labor share signals that hospital wages, salaries, and employee benefits account for a smaller share of total costs in the post-pandemic environment. This change may come to a surprise to some, as hospital labor costs have been a subject of concern since the COVID-19 public health emergency.
Medicare Advantage Data Integration in Measuring Hospital Readmissions
Proposed Rule: CMS proposed to make several modifications to the Hospital Readmissions Reduction Program (HRRP), including:
- Refining all six readmission measures to add MA patient data
- Removing the COVID-19 patient denominator exclusion from measures
- Reducing the applicable period from three years to two
- Modifying the DRG payment ratios in the payment adjustment formula to include MA beneficiaries
- Clarifying that CMS has the discretion to grant an extension to hospitals under the extraordinary circumstances exception (ECE)
CMS also proposed to include MA data in other measures included in the Hospital Value-Based Purchasing (VBP) program and the Inpatient Quality Reporting (IQR) program.
HMA Analysis: The inclusion of MA data in the HRRP may have significant payment implications for many hospitals because it will alter their readmission rates in unanticipated ways, particularly if hospitals’ MA patients differ substantially from traditional Medicare beneficiaries. Importantly, the inclusion of MA data in the HRRP measures, and also within the VBP program and the IQR program, signals that CMS is moving toward broader integration of MA data into Medicare fee-for-service reimbursement systems.
New Technology Add-on Payment Program Growth
Proposed Rule: CMS proposed to continue NTAP status for 26 products because they continue to meet the newness criteria required under this program. In addition, within the proposed rule CMS discusses new NTAP applications for 43 additional products. Among these applications, 29 were submitted under the alternative pathways for breakthrough devices and qualified infectious disease products (QIDP).
HMA Analysis: The overall number of products with NTAPs is on par with other recent years, but the number of NTAP applications has blossomed in FY 2026 as the result of the alternative breakthrough application pathway. This alternative pathway allows breakthrough devices and certain antibiotic and antimicrobial drugs to apply for NTAP using an abbreviated application process.
Transforming Episode Accountability Model Modifications
Proposed Rule: CMS proposed several modifications to the forthcoming CMS Innovation Center TEAM framework. Among the various methodological modifications proposed to this mandatory payment model beginning January 1, 2026, CMS proposed to take the following actions:
- Limit the deferment period for certain hospitals
- Replace the Area Deprivation Index (ADI) with the Community Deprivation Index (CDI)
- Use a 180-day lookback period and Hierarchical Condition Categories (HCC) for risk adjustment
- Remove health equity and health-related social needs data reporting
- Expand use of the Skilled Nursing Facility (SNF) three-day rule waiver
HMA Analysis: The critical aspect of CMS’s TEAM provision is that the agency proposes to follow through with this Innovation Center model while cancelling other Innovation Center payment models in recent months. It also is noteworthy that the agency has proposed to remove the health equity data reporting requirements for TEAM in line with actions taken with many other CMS programs. Another proposal of note is the plan to expand the use of the waiver to circumvent the SNF three-day inpatient stay rule, which will allow hospitals to discharge patients more quickly to SNFs.
Uncompensated Care Payment Increase for Disproportionate Share Hospitals
Proposed Rule: CMS proposes to increase uncompensated care payments to DSHs by $1.5 billion in FY 2026.
HMA Analysis: CMS’s proposal will increase uncompensated care payments to hospitals by 26 percent. This increase is driven by CMS’s assumption that the rate of uninsured people will increase to 8.7 percent of the population in 2026 from 7.7 percent in 2025.
Stakeholder comments on the IPPS proposed rule are due no later than June 10, 2025.
Connect With Us
The Health Management Associates, Inc. (HMA), Medicare Practice Group monitors federal regulatory and legislative developments in the inpatient setting and assesses the impact on hospitals, life science companies, and other stakeholders. Our experts interpret and model hospital payment policies and assist clients in developing CMS comment letters and long-term strategic plans. Our team replicates CMS payment methodologies and model alternative policies using the most current Medicare fee-for-service and Medicare Advantage (100%) claims data. We also support clients with DRG reassignment requests, NTAP applications, and analyses of Innovation Center alternative payment models.
For more information about the proposed policies, please contact Zach Gaumer ([email protected]), Amy Bassano ([email protected]), or Clare Mamerow ([email protected]).
[1] U.S. Bureau of Labor Statistics. Table 1. Consumer Price Index for All Urban Consumers (CPI-U): U.S. City Average, by Expenditure Category. Modified April 10, 2025.
[2] Centers for Medicare & Medicaid Services. 2026 Medicare Advantage and Part D Rate Announcement. April 7, 2025.
The Medicare Advantage VBID Program Is Ending: Here’s What All Plans Can Do to Prepare for What’s Next
This week, our second In Focus article addresses the transition to end the Medicare Advantage Value-Based Insurance Design (VBID) model, which launched in 2017 and subsequently has been expanded with bipartisan support. This model was designed to promote flexible benefit design, reduce cost barriers, and enhance care for targeted populations, especially dual eligibles and individuals with chronic conditions. In December 2024, however, the Centers for Medicare & Medicaid Services (CMS) announced that the model would be terminated by the end of 2025, citing unmitigable costs to the Medicare Trust Funds, totaling more than $4.5 billion across 2021 and 2022 alone.
Despite its popularity and effectiveness in improving medication adherence and addressing social determinants of health, CMS concluded that the cost trajectory was unsustainable within the parameters of the Innovation Center’s mandate.
The end of the VBID model is not the end of innovation in Medicare Advantage (MA); rather, it is a strategic inflection point. Plans that approach this transition with a proactive, data-driven lens will be best positioned to maintain competitive advantage, compliance, and member trust. This article reviews critical steps VBID plans should be taking and how Medicare Advantage Organizations (MAOs) and their partners can best prepare for future opportunities.
Pain Points and Key Strategic Decisions for MAOs
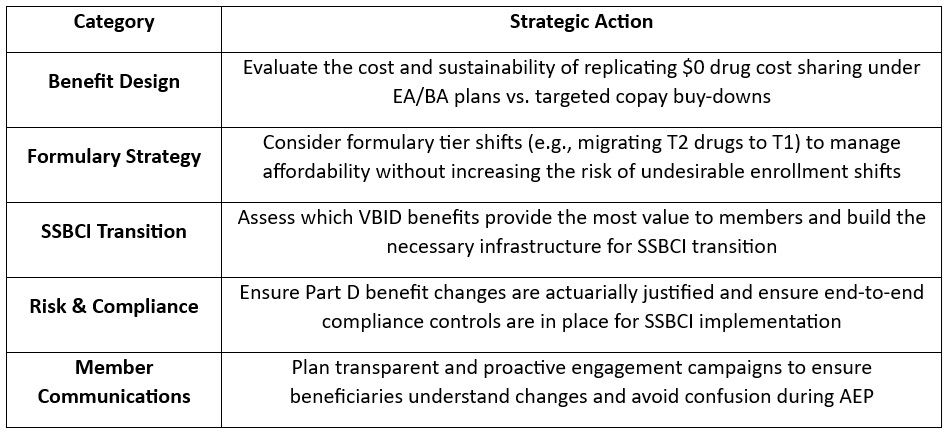
As plans prepare for a post-VBID world, they face a series of complex trade-offs—especially those with Dual Eligible Special Needs Plans (D-SNPs) that had $0 drug cost sharing under VBID. With the end of CMS’s drug cost offset in the initial coverage phase, MAOs will need to determine whether and how to absorb those costs through alternative mechanisms. In addition, plans will need to make important decisions regarding their other VBID benefits, namely, whether to discontinue or transition them to the special supplemental benefits for the chronically ill (SSBCI) program. MAOs should consider the following key strategic decisions:
- Offer an Enhanced Alternative (EA) or Basic Alternative (BA) Part D Plan: To replicate $0 cost sharing, MAOs would need to use EA or BA plan designs with $0 deductibles and $0 copays across all tiers—an expensive move and potentially untenable investment for many.
- Tier-Specific Buy-Downs (T1/T2): Some plans may consider buying down T1 and T2 copays to $0, a much less costly approach. Others may consider moving key T2 drugs to T1, while keeping T1 copays at $0 to protect access and using non-zero dollar T2 copays to limit costs.
- Competitive Alignment Considerations: MAOs offering broader cost-sharing reductions (e.g., $0 copays on both T1 and T2 drugs) may experience undesirable shifts in enrollment patterns depending on how competitors structure their formularies and benefit designs. MAOs should consider competitive parity and attempt to maintain a balanced benefit structure that aligns with market norms.
- Transferring VBID Benefits to SSBCI: Some benefits—like non-health-related transportation, healthy foods, and general supports for living—could migrate to the SSBCI program. But SSBCI has strict eligibility, documentation, and operational requirements, calling for nuanced workflows and cross-departmental coordination.
Action Plan: What MAOs Should Be Doing Now
To navigate this transition successfully, teams of experts at Wakely, a Health Management Associates, Inc. (HMA) Company, are already working with VBID stakeholders to evaluate multiple transition scenarios. Our experts recommend that MAOs take the following actions:
What to Watch: Future Innovation in Medicare Advantage
Though VBID is ending, the innovation landscape is far from static. With the new Trump Administration and the return of Abe Sutton—a VBID expansion advocate—appointed as Director of the CMS Innovation Center, our experts are closely monitoring the potential for a revised version of VBID or similar models. Stakeholder advocacy could influence how CMS prioritizes the next wave of innovation. Plans should consider engaging in dialogue now to shape what happens next.
Connect with Us
Wakely is embedded in MA strategy and policy. Wakely and HMA teams are working with clients to evaluate multiple transition scenarios, helping them optimize value, protect Star Ratings, and preserve member satisfaction during this pivotal shift, while also supporting targeted policy engagement efforts to ensure their perspectives are reflected in future CMS and Innovation Center decision making.
Our joint capabilities bring together:
- Actuarial modeling expertise to quantify cost and risk impacts of design alternatives
- Regulatory insight to ensure compliance with CMS requirements
- Operational support to help you implement SSBCI programs efficiently
- Market strategy consulting to align your plan offerings with local competition and enrollment goals
- Policy advocacy to help clients engage in the conversation around what comes next after VBID
To connect on additional questions contact our featured experts Eric Wiliams and Elizabeth Ritter.
HMA Roundup
Arizona
Arizona Submits Section 1115 Demonstration Amendment for Medicaid Work Requirements, Lifetime Coverage Limits. The Centers for Medicare & Medicaid Services (CMS) announced on April 10, 2025, that Arizona has submitted a request to amend its Section 1115 Arizona Health Care Cost Containment System (AHCCCS) demonstration to implement Medicaid work requirements, a five-year lifetime coverage limit for certain adults, and cost-sharing requirements to discourage non-emergency use of emergency services. The program would require adults aged 19 to 55 to engage in at least 20 hours per week of employment, education, or job training to maintain coverage. Public comments will be accepted through May 9, 2025.
Arkansas
Arkansas Legislature Advances Bill to Increase ARHOME Medicaid Expansion MLR, Add Work Requirements. Arkansas Senate Bill 527 to increase the Arkansas Health and Opportunity for Me (ARHOME) Medicaid expansion program Medicaid loss ratio (MLR) was passed by the Legislature on April 15, 2025, and delivered to the Governor for consideration. The bill proposes amendments to improve the program’s fiscal sustainability and healthcare outcomes. Key provisions include increasing the medical loss ratio to ensure more funds are directed toward patient care, mandating that insurers seek and remit pharmacy rebates to the state, and authorizing the Governor to request a federal waiver to implement work requirements for Medicaid beneficiaries.
Arkansas Senate Passes Bill to Ban PBM Pharmacy Ownership. STAT News reported on April 10, 2025, that Arkansas Senate has passed a House Bill 1150 which prohibits pharmacy benefit managers (PBMs) from owning or operating retail and mail-order pharmacies within the state. The legislation aims to address perceived conflicts of interest and pricing practices linked to PBMs that lawmakers say harm independent pharmacies and consumers. The bill is now awaiting action by Governor Sarah Sanders.
Senate Committee Blocks Postpartum Medicaid Extension. The Arkansas Advocate reported on April 9, 2025, that the Arkansas Senate Public Health Committee voted down House Bill 1004, which would have extended postpartum Medicaid coverage from 60 days to 12 months for women not already covered under the state’s Medicaid expansion. Although the bill passed the House with bipartisan support, it failed in the Senate Committee amid concerns over cost and duplication of services. The state Department of Human Services (DHS) opposed the measure, estimating a state cost of $2.4 million.
California
California Governor Signs $2.8 Billion Bill to Close Medi-Cal Gap, Maintain Coverage Through June. The Associated Press reported on April 14, 2025, that California Governor Gavin Newsom signed a bill allocating $2.8 billion to close a budget gap in Medi-Cal and maintain coverage through June for 15 million low-income residents, including undocumented immigrants. The funding is part of a broader effort to address a $6.2 billion shortfall driven by higher-than-expected costs from expanding Medi-Cal eligibility, after state officials underestimated enrollment and faced rising pharmacy and elderly care expenses. To date, California has borrowed the maximum allowed from its general fund to keep the program afloat. State officials warn the current situation is unsustainable and are weighing cost-cutting measures for the next fiscal year, including possible changes to enrollment policies.
Connecticut
Connecticut Faces Civil Lawsuit Challenging HUSKY C Income Limits for Disabled Beneficiaries. CT Insider reported on April 11, 2025, that a civil rights lawsuit was filed against the Connecticut Department of Social Services, alleging that the state’s Medicaid eligibility rules discriminate against people with disabilities. The suit, filed with the Hartford judicial district, argues that disabled residents are unfairly restricted to the HUSKY C plan for the aged, blind, or disabled, which has stricter income and asset limits than HUSKY D, Medicaid for low-income adults without dependent children, effectively denying them access to Medicaid. The plaintiffs claim this violates the state Constitution’s equal protection clause and seek to raise HUSKY C income limits to match those of HUSKY D.
District of Columbia
Amerigroup DC, DC Connected Care Network Launch Medicaid VBA. Amerigroup DC and the DC Connected Care Network (DC CCN) announced on April 10, 2025, that they have launched Washington, D.C.’s first Medicaid Value-Based Agreement (VBA). This three-year partnership includes seven Federally Qualified Health Centers (FQHCs) and is designed to improve healthcare equity, quality, and efficiency for Medicaid enrollees. The VBA links provider payments to performance on health outcomes, with shared financial risk and a focus on preventive care, chronic disease management, and data-driven decision-making.
Florida
Florida House Committee Advances Bill to Expand Medicaid Access for Medically Fragile Children. Florida Politics reported on April 16, 2025, that the Florida House Health and Human Services Committee unanimously passed House Bill 1529, which seeks to expand Medicaid access to families caring for medically fragile children. The bill, sponsored by Representative Chase Tramont (R-Port Orange), would make changes to the Home Health Aides for Medically Fragile Children (HHAMFC) program—which allows family members to be reimbursed by Medicaid if they are a home health aide to an eligible relative—by disregarding any income a family makes from the program when determining their Medicaid eligibility. As the program stands, families being reimbursed by HHAMFC are likely to make too much money to qualify for Medicaid.
Florida Legislators Consider Bill to Transition Agency Oversight for the Children’s Medical Services Program. Florida Health News reported on April 10, 2025, that state legislators are considering legislation that would transfer oversight of the Children’s Medical Services program from the Florida Department of Health (DOH) to the Agency for Health Care Administration (AHCA). House Bill 1085 seeks to streamline services for the medically complex children that the program services, according to bill sponsor Representative Vanessa Oliver (R-Punta Gorda). It would also expand home health services and reduce administrative personnel from 50 at the DOH to four at AHCA. The bill is on the House Health Care Budget Subcommittee calendar.
Florida MCO Pays Out $67 Million PBM Settlement to AHCA, Hope Florida. Politico reported on April 9, 2025, that Medicaid managed care organization (MCO), Centene, paid $57 million to the Florida Agency for Health Care Administration and $10 million to the Hope Florida Foundation as part of a $67 million out-of-court settlement over a lawsuit claiming the insurer’s pharmacy benefit manager (PBM) had failed to pay out savings made through prescription drug rebates. Hope Florida, led by First Lady Casey DeSantis, is a program meant to help Floridians become more financially independent and depart from publicly-funded programs such as Medicaid through access to community-based services. State lawmakers have raised concerns that the $10 million payment to Hope Florida was not legal and should have been deposited into a state bank account.
Indiana
Indiana Governor Signs Multiple Executive Orders Aligned with Make America Healthy Again Initiative. Fierce Healthcare reported on April 16, 2025, that Indiana Governor Mike Braun has signed nine executive orders at a “Make Indiana Healthy Again” press conference, which aim to align the state with the Trump administration’s Make America Healthy Again initiative. One order seeks to bolster the state’s Medicaid program integrity and reduce costs by directing the state to submit a report to the Centers for Medicare & Medicaid Services (CMS) on improper payments by October 2025, to no longer accept certain eligibility information without verification before enrollment unless federally required, and to review eligibility information more frequently. Other executive orders focused on food-related and prevention initiatives, which would impose stricter work and eligibility requirements from the Supplemental Nutrition Assistance Program (SNAP), remove candy and soft drinks from SNAP, prompt evaluations of food dyes and diet-related chronic diseases, and increase direct-to-consumer food.
Iowa
Iowa Submits Section 1115 Demonstration Application to Impose Medicaid Expansion Work Requirements. The Iowa Capital Dispatch reported on April 15, 2025, that Iowa has submitted a Section 1115 demonstration application to the Centers for Medicare & Medicaid Services (CMS) to require most able-bodied adults enrolled in the state’s Medicaid expansion program to work at least 100 hours per month to maintain coverage in the Iowa Health and Wellness Plan (IHAWP). If the federal government rejects the waiver, state legislation mandates that the entire IHAWP program be terminated. The proposal could impact up to 142,000 Iowans, with an estimated 32,000 likely to lose coverage. Public hearings on the waiver are scheduled for April 23 and April 29.
Kansas
Kansas Legislature Overrides Veto to Reform Medicaid Contracting Process. The Kansas Reflector reported on April 11, 2025, that the Kansas Legislature overrode Governor Laura Kelly’s veto on House Bill 2284, which imposes new requirements on how the state conducts Medicaid managed care procurements. The bill requires the executive branch to preserve all procurement records, adopt formal tiebreaking procedures, and increase transparency with the Legislature throughout the bidding process. It also establishes a new appeals process led by a legislative panel, replacing the current system where bid protests are reviewed solely through the courts. The bill was introduced after Aetna Better Health of Kansas lost its bid to remain a KanCare managed care organization and unsuccessfully challenged the process, citing destroyed scoring records and a lack of transparency.
Nevada
Nevada to Split Department of Health and Human Services; Releases Fiscal 2026-27 Budget Priorities. The Nevada Department of Health and Human Services Division of Health Care Financing and Policy released in April 2025 its budget priorities for the 2026-27 budget biennium, including reorganizing the Department of Health and Human Services to create the Nevada Health Authority and the Department of Human Services. The Nevada Health Authority will house the Medicaid program, along with the state health care purchasing unit, the healthcare workforce unit, the consumer health and access unit, and public employee benefits. Meanwhile, the Department of Human Services will focus on social, aging, children/family, and public health services. The new authority, which must be approved by the state legislature, is meant to strengthen the state’s purchasing power related to health insurance and improve member services. The biennium budget supports funding for improving access to care by strengthening the healthcare workforce, strengthening the behavioral healthcare system, adding adult dental coverage to Medicaid, and modernizing the Medicaid enrollment and eligibility systems.
New York
New York CDPAP Home Care Program Still Has 30,000 Recipients Yet to Re-enroll. Crain’s New York reported on April 15, 2025, that approximately 30,000 recipients have yet to re-enroll in New York’s Consumer Directed Personal Assistance Program (CDPAP) with the state’s new administrator, Public Partnerships LLC (PPL), potentially disrupting essential home care services for these individuals. Approximately 190,000 individuals have already enrolled. The state previously implemented a one-month grace period to assist consumers experiencing difficulties with the registration process and a proposed delay is waiting to be finalized by a federal judge to push the transition to June 6.
North Carolina
North Carolina Lawmakers Advance Medicaid Work Requirement Bills. The Carolina Journal reported on April 10, 2025, that North Carolina lawmakers in both chambers have advanced legislation that seeks to add work requirements to the Medicaid program. Senate Bill 403, sponsored by Senator Ralph Hise (R-Mitchell), and House Bill 491, sponsored by Representative Donny Lambeth (R-Forsyth), would direct the state Department of Health and Human Services to apply for a waiver to implement Medicaid work requirements for expansion beneficiaries. Both bills were approved by their respective health committees.
Oregon
Oregon Submits Extension Request for SUD Section 1115 Demonstration. The Centers for Medicare & Medicaid Services announced on April 10, 2025, that Oregon has a submitted a request to extend its Oregon Health Plan Substance Use Disorder (SUD) Section 1115 Demonstration though March 31, 2031. The application requests to keep all currently approved authorities and seeks to add authority to provide contingency management incentives as a medical intervention for eligible beneficiaries to help motivate enrollees to meet their treatment goals. The current demonstration is approved through March 31, 2026. Public comments will be accepted until May 9, 2025.
Oregon Completes Medicaid Unwinding; 83 Percent Maintain Benefits. The Oregon Health Authority (OHA) announced on April 10, 2025, that the state completed its post-pandemic Medicaid eligibility redeterminations at the end of February, with 83 percent of enrollees maintaining benefits, according to an analysis of the state’s Public Health Emergency Unwinding Project. Oregon disenrolled 247,104 individuals between April 1, 2023, and February 28, 2025. OHA renewed coverage for 1,169,042 individuals and reduced benefits for 40,563. Most of the beneficiaries with reduced coverage were removed from the full Oregon Health Plan but are able to continue in Medicare Savings Programs.
Wisconsin
Wisconsin Bill Proposing Stricter Medicaid Eligibility Requirements Stalls After Hearing. The Wisconsin Examiner reported on April 16, 2025, that Wisconsin Assembly Bill 163, which proposes more frequent and stricter Medicaid eligibility reviews, is currently on hold after facing opposition at a recent public hearing. The bill would require eligibility redeterminations every six months, prohibit automatic renewals, restrict pre-filled information on forms, and impose a six-month enrollment lockout for beneficiaries who fail to report changes affecting eligibility. The bill remains in the Assembly Committee on Public Benefit Reform while amendments are considered, including one that would exempt individuals with developmental disabilities from certain provisions.
National
Trump Signs Executive Order on Drug Price Negotiations, Hospital Payments. STAT News reported on April 15, 2025, that President Donald Trump signed an executive order meant to lower prescription drug prices, increase transparency with pharmacy benefit managers, and limit outpatient Medicare payments to hospitals. The order directs the U.S. Department of Health and Human Services Secretary Robert F. Kennedy Jr. to:
• Guide Medicare drug price negotiations for 2026–2028 under the Inflation Reduction Act
• Develop a payment model to improve Medicare’s value on high-cost drugs
• Survey hospital acquisition costs to reduce outpatient drug reimbursement
• Ensure health centers pass 340B discounts on insulin and epinephrine to eligible patients
• Recommend ways to strengthen the pharmaceutical supply chain
• Align timelines for small molecule and biologic drug negotiations
• Consider rules to prevent Medicare payment policies from driving patients to higher-cost facilities
Separately, OMB, HHS, and other departments must provide the president with recommendations to ensure drug manufacturers pay accurate Medicaid drug rebates, to promote innovative Medicaid drug payment methodologies, to link drug payments to the value they give, and to support states in lowering prescription drug spending. In addition, it directs the Food and Drug Administration to work with states to improve the process of applying for the Canadian drug importation program and streamline the approval of generic drugs and biosimilars.
CMS Releases FY 2026 SNF Payment Proposed Rule with 2.8 Percent Rate Increase. The Centers for Medicare & Medicaid Services (CMS) released on April 11, 2025, a proposed rule for the FY 2026 Skilled Nursing Facility Prospective Payment System (SNF PPS), which includes a 2.8 percent net payment increase ($720 million) and updated ICD-10 code mappings under the Patient-Driven Payment Model (PDPM). The rule proposes updates to the SNF Value-Based Purchasing (VBP) Program, including the removal of the health equity adjustment, addition of a new reconsideration process, and a change in scoring methodology for low-volume facilities. For the SNF Quality Reporting Program, CMS proposes removing four standardized patient assessment data elements (SPADEs) related to social determinants of health (SDOH) to reduce burden.
CMS Releases FY 2026 Hospice Wage Index, Payment Rate Update Proposed Rule With 2.4 Percent Rate Increase. The Centers for Medicare & Medicaid Services (CMS) released on April 11, 2025, the Fiscal 2026 Hospice Wage Index and Payment Rate Updated Proposed Rule, which recommends a 2.4 percent, or $695 million, increase to hospice reimbursement rates. The rule also seeks to clarify hospice payment regulations as to who may recommend admission to hospice care to align with certification regulations and the Conditions of Participation, and that hospice face-to-face encounter attestation must include a clinician’s signature and date. CMS is also releasing two requests for information (RFIs) regarding the Hospice Quality Reporting Program (HQRP) to gain input on future measures on the topics of interoperability, nutrition, and well-being, and on advancing digital quality measurement.
CMS Recommends 2.6 Percent Rate Increase in FY 2026 Inpatient Rehabilitation Facility PPS Proposed Rule. The Centers for Medicare & Medicaid Services (CMS) released on April 11, 2025, the Fiscal Year 2026 Inpatient Rehabilitation Facility Prospective Payment System (IRF PPS) Proposed Rule, which recommends a 2.6 percent rate increase worth an estimated $295 million. The rule proposes to remove two measures from the IRF Quality Reporting Program—the COVID-19 Vaccination Coverage among Healthcare Personnel measure and the COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date measure—and remove four Social Determinant of Health (SDOH) standardized patient assessment data elements. The rule also seeks to amend the reconsideration policy. In addition, CMS is releasing four requests for information (RFIs) regarding IRFs. The RFIs seek feedback on potential future measures on the topics of interoperability, nutrition, delirium, and well-being; possible revisions to the IRF-Patient Assessment Instrument; possible revisions to the data submission deadlines for assessment data; and advancing digital quality measurement.
CMS Releases FY 2026 Medicare Inpatient Psychiatric Facility PPS Proposed Rule, Recommends 2.4 Percent Rate Increase. The Centers for Medicare & Medicaid Services (CMS) released on April 11, 2025, the Fiscal Year 2026 Medicare Inpatient Psychiatric Facility Prospective Payment System (IPF PPS) and Quality Reporting Updates Proposed Rule reccomending a 2.4 percent reimbursement rate increase for IPFs. The proposed rule updates facility-level adjustment factors, and also updates the Extraordinary Circumstances Exception policy and quality measures in the IPF Quality Reporting Program. The updates would modify the IPF Emergency Department Visit Measure reporting period and remove four reporting measures from payment determinations: Facility Commitment to Health Equity; COVID–19 Vaccination Coverage among Health Care Personnel; Screening for Social Drivers of Health; and Screen Positive Rate for Social Drivers of Health. CMS is also issuing three requests for information regarding the IPFQR program seeking input on a potential future star rating system, future measure concepts on the topics of well-being and nutrition, and the potential usage of Fast Healthcare Interoperability Resources standards for IPFs reporting patient assessment data to CMS.
CMS Issues RFI on Potential Changes to Medicare Regulations. The Centers for Medicare & Medicaid Services (CMS) released on April 11, 2025, a request for information (RFI) “Unleashing Prosperity Through Deregulation of the Medicare Program,” potential changes to Medicare regulations in response to President Trump’s Executive Order 14192. The RFI seeks stakeholder input on ways to reduce regulatory burden and streamline Medicare rules without compromising care quality or program integrity. CMS is requesting feedback on how to simplify or eliminate duplicative administrative, documentation, and reporting requirements, including those related to Conditions of Participation, quality programs, and value-based payment models. The agency also seeks suggestions to align Medicare policies with industry standards and reduce overlap with Medicaid and private insurance requirements. Responses are due by June 10, 2025.
Trump Administration Launches Investigation Into Pharmaceutical Imports. STAT News reported on April 14, 2025, that the U.S. Department of Commerce has launched an investigation into how the importation of pharmaceuticals may threaten national security. The investigation will look at current and projected pharmaceutical demand, whether domestic production can meet the demand, foreign supply chains, and the associated risks of having a concentration of imports with a small number of suppliers. The notice of the investigation comes after President Donald Trump indicated that he would impose tariffs on pharmaceutical imports.
Hospitals Sue HHS Over Denied Medicare Disproportionate Share Hospital Payments. Modern Healthcare reported on April 14, 2025, that almost 150 hospitals have filed three lawsuits against the U.S. Department of Health and Human Services (HHS) over claims its Provider Reimbursement Review Board wrongfully denied appeals for disproportionate share hospital (DSH) payments. The lawsuits, representing providers from over 25 states, claim that the Centers for Medicare & Medicaid Services (CMS) should take into account all Medicare, Medicare Advantage, and Social Security Supplemental Security Income (SSI) beneficiaries when calculating DSH payments. CMS currently calculates DSH payments based only on the number of fee-for-service Medicare patients receiving SSI cash assistance during hospital stays.
Congress Passes Fiscal 2026 Budget Resolution with $880 Billion Healthcare Cuts. Modern Healthcare reported on April 10, 2025, that Congress has finalized the fiscal year 2026 budget resolution, a joint framework approved by both the House and Senate. The resolution instructs House committees to find at least $1.5 trillion in cuts, including up to $880 billion by the House Energy and Commerce Committee from Medicaid or other healthcare programs. The Senate committees are only required to cut $4 billion. Lawmakers will begin drafting reconciliation bills after the recess, though divisions remain within the Republican caucus regarding the scope of proposed tax and spending changes.
CMS to End Approvals of DSHP, DSIP Federal Matching Funds. The Centers for Medicare & Medicaid Services (CMS) announced on April 10, 2025, that it will no longer approve new or existing requests for federal matching funds through Section 1115 demonstration authority for designated state health programs (DSHP) and designated state investment programs (DSIP). The move intends to refocus CMS on its core mission of preserving the Medicaid program by ending spending that “duplicates resources” or is not directly tied to healthcare services for Medicaid beneficiaries, such as childcare, housekeeping, rural internet services, etc. CMS indicated that it will continue to focus on the statutory objectives of the Medicaid program. DSHPs and DSIPs had $2.7 billion in eligible expenditures in 2025.
Dr. Mehmet Oz Outlines Priorities for CMS. The Centers for Medicare & Medicaid Services (CMS) announced on April 10, 2025, that new administrator Dr. Mehmet Oz has outlined his priorities and vision for the agency. Oz will prioritize President Trump’s Make America Healthy Again initiative and aims to modernize Medicare, Medicaid, and the Marketplaces. Oz’s plans include: implementing President Trump’s executive order on transparency; equipping providers with better information about patients and holding them more accountable for health outcomes; identifying and eliminating fraud, waste, and abuse; and focusing on preventative care and disease management such as improving holistic health outcomes.
MACPAC Releases Briefs Exploring State, Federal Strategies to Manage Medicaid Spending Growth. The Medicaid and CHIP Payment Access Commission (MACPAC) released in April 2025, two policy briefs which explore strategies to manage Medicaid spending growth at both the state and federal levels. The first brief outlines options available to states, such as modifying eligibility, benefits, provider payment rates, and delivery systems, as well as improving program integrity to help control costs. The second brief examines alternative approaches to federal Medicaid financing, including policy design considerations intended to ensure long-term fiscal sustainability. Together, the briefs highlight the need for balanced solutions that maintain access and quality while addressing rising costs shared by state and federal governments.
Industry News
UnitedHealth Group, Amedisys Antitrust Lawsuit Heads to Mediation. Modern Healthcare reported on April 14, 2025, that a federal judge has signed a mediation order for the U.S. Department of Justice’s antitrust lawsuit against UnitedHealth Group and Amedisys. The lawsuit is attempting to block United’s $3.3 billion acquisition of Amedisys over claims that it would stifle competition in the hospice and home health industries. The mediation is set to begin August 18, 2025.
CMS Denies Humana Administrative Appeal Over Star Ratings. Health Payer Specialist reported on April 16, 2025, that the Centers for Medicare & Medicaid Services (CMS) denied Humana’s administrative appeal over 2026 quality bonus payments tied to its 2025 Medicare Advantage star ratings. Humana is pursuing a separate lawsuit to compel CMS to revise the ratings, which if successful could double its projected 2026 earnings. The dispute centers on CMS penalizing Humana for disconnected calls during secret shopper tests, which Humana says were mischaracterized. CMS rejected Humana’s argument due to a lack of supporting call logs. A similar challenge by UnitedHealth previously succeeded.
Scan Group, Sutter Health to Launch Joint Medicare Advantage Plans in 2026. Modern Healthcare reported on April 10, 2025, that Scan Group and Sutter Health are partnering to launch a new nonprofit Medicare Advantage company in California. The entity, set to launch in 2026, will focus on developing technology, co-branded plans, and care models for California’s 6.9 million Medicare-eligible residents. The collaboration aims to roll out new private Medicare plans over the next three years, starting fall 2025.
RFP Calendar

The Actuaries' Corner
Trump Rejects Biden Administration Plan to Let Medicare Cover Obesity Drugs. The Trump administration will not permit Medicare to pay for obesity drugs directly, declining on Friday to finalize a Biden-era proposal that would have allowed the federal health insurance program to cover popular GLP-1 medications like Wegovy and Zepbound.
Discover other developments in the Wakely Wire here.
HMA News & Events
Leavitt Partners Webinar
Digital Health & Interoperability Policy: New Ideas to Drive Federal Government Efficiency. Thursday, April 24, 2025, 12 PM ET. Building on previous successes across multiple administrations, we have an opportunity to continue to advance patient data exchange by taking an innovative approach to federal health care technology policy. How can we more effectively advance Fast Healthcare Interoperability Resources Application Programming Interface (FHIR API)-based data exchange between payers, providers, patients, and pharmacies? What should the role of The Centers for Medicare & Medicaid Services (CMS) and Office of the National Coordinator for Health IT (ONC) be over the next decade? What federal technology policies are needed (or not needed any longer) to truly create a patient-centered health care system? How does Certified Electronic Health Record Technology (CEHRT) need to evolve to support a modern, API-based, interoperable ecosystem? Join us to explore how top payers and providers, in collaboration with Leavitt Partners, an HMA Company, crafted bold, innovative federal technology and interoperability policy recommendations for the Trump administration.
HMA Webinars
Ask HMA Experts: Medicare Town Hall. Wednesday, April 30, 2025, 12 PM ET. Join us for an open and engaging Medicare Town Hall with the experts from Health Management Associates (HMA). Whether you’re navigating Medicare Advantage policy changes, seeking actuarial insights, analyzing risk-based payment structures, or working to improve integration for Dual Eligibles and align D-SNPs, our team is here to provide actionable insights and answers. This is your opportunity to ask anything—from strategy to service delivery, coverage to compliance. We’ll have HMA professionals from across the country ready to share their perspectives and help you navigate the complexities of Medicare. Bring your questions. Share your ideas. Gain clarity.
PACE Development Best Practices for Policy Makers and Program Sponsors. Thursday, May 15, 2025, 1 PM ET. Health Management Associates (HMA) conducted a multi-state study to examine the policy decisions influencing the operation and expansion of Programs of All-Inclusive Care for the Elderly (PACE). It explored different program structures, associated advantages and challenges, and strategies to enhance efficiency while meeting regulatory requirements. This webinar will summarize our research on 10 active PACE states (CA, FL, IL, KY, LA, MA, NJ, NY, OH, and WA) that have either implemented or expanded their PACE programs between 2020 and 2024. Using state survey responses and credible third-party, publicly available data, we will showcase the outcomes of PACE program development through open and competitive RFP processes. We will also outline development timelines to demonstrate the effectiveness of each approach and highlight key insights gained during the discovery and research phase of the study.
Survey Readiness: Prepare, Respond, Succeed, a 5-part Virtual Series. Every Wednesday in April 1:00 PM to 2:30 PM ET.
In today’s complex healthcare environment, navigating the scrutiny of regulatory and accreditation bodies like The Centers for Medicare & Medicaid Services (CMS), Department of Health (DOH), The Joint Commission, and Det Norske Veritas (DNV) Healthcare is critical for the success of every hospital and health system. Unexpected surveys, triggered by recertification, validations or even complaints, can occur at any time.
HMA has partnered with the Healthcare Association of New York State (HANYS) to develop the content for Survey Readiness: Prepare, Respond, Succeed, a 5-part virtual series on Wednesdays in April from 1- 2:30pm ET. HMA’s expert faculty will also co-teach the sessions. Attendees will dive deep into organizational strategies and tactics to prepare, manage and respond to surveyors effectively – and get the essential skills to excel in survey readiness.
While some examples in the program will address issues from the New York state perspective, attendees from organizations nationwide should attend. Hospital and long-term care executive team and leaders in quality and compliance, survey coordinators, and risk management will benefit from attending.
Survey Readiness: Prepare, Respond, Succeed
Virtual Series | April 2 – 30
- April 2: Survey readiness 101: Overview and getting started
- April 9: Preparation: How to mitigate risk and prepare for upcoming surveys
- April 16: They’re here: Establishing a survey response and management protocol
- April 23: Responding to survey findings: How to develop a strong correction plan and knowing your options
- April 30: What’s next: Leveraging survey findings and strengthening organizational quality and compliance
The cost to attend this series is $475.
State hospital associations and their members can enjoy $50 off when using this code when registering: SHADISCOUNT25
NEW THIS WEEK ON HMA INFORMATION SERVICES
(Exclusive Access for HMAIS Subscribers):
HMAIS Reports
- Updated Medicaid Fee-for-Service Pharmacy Benefit Management RFP Calendar
- Updated Section 1115 Medicaid Demonstration Inventory
- Updated California, Maryland, and Oregon State Overviews
Medicaid Data
Medicaid Enrollment and Financial data from Indiana, Iowa, Kentucky, Mississippi, Pennsylvania, Rhode Island, South Carolina, West Virginia, and Wyoming.
Public Documents:
Medicaid RFP documents from Arkansas, Delaware, District of Columbia, Hawaii, Idaho, Indiana, Iowa, Kansas, New Hampshire, New Mexico, North Carolina, Tennessee, and Wyoming.
Medicaid Managed Care Rate Certifications, Medicaid Annual Reports, Medicaid Quality Strategy Reports, Medicaid Committee Meeting Materials, and other key documents from the following states: Alaska, Arizona, Nevada, Oregon, and Wyoming.
A subscription to HMA Information Services puts a world of Medicaid information at your fingertips, dramatically simplifying market research for strategic planning in healthcare services. An HMAIS subscription includes:
- State-by-state overviews and analysis of latest data for enrollment, market share, financial performance, utilization metrics and RFPs
- Downloadable ready-to-use charts and graphs
- Excel data packages
- RFP calendar
If you’re interested in becoming an HMAIS subscriber, contact Andrea Maresca at [email protected].