HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
This week, our In Focus section reviews the projected healthcare expenditure and enrollment data from the Centers for Medicare & Medicaid Services (CMS) Office of the Actuary, published June 14, 2023. The Office of the Actuary provides annual updates to historical and projected National Health Expenditure data on Medicare, Medicaid, CHIP, and other public insurance programs, as well as commercial healthcare insurance.
CMS projects that the average annual growth for national healthcare spending from now through 2031 will be 5.4 percent. CMS estimated that the number of insured individuals in the United States was projected to reach a high of 92.3 percent in 2022 and would decrease to 90.5 percent by 2031. CMS projects 93.6 million Medicaid and CHIP members will account for more than $1.2 trillion in annual spending in 2031 and that 76.4 million Medicare beneficiaries will account for more than $1.8 trillion in expenditures that year. A summary of other key takeaways from the actuarial report follows.
Enrollment Projections
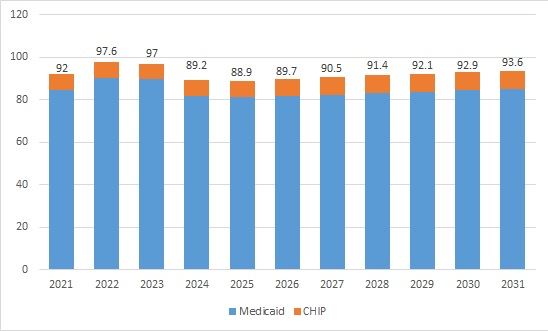
Approximately 92 million people were enrolled in Medicaid and CHIP programs in 2021. Enrollment is projected to have reached a high of 97.6 million in 2022 and is expected to fall between 2023 and 2026 because of Medicaid redeterminations. CMS projects the largest loss in 2024, with 8 million people leaving Medicaid and CHIP that year alone. By 2026, enrollment is projected to hit a low of 89.7 million and start to rise back up in the subsequent years until reaching 93.6 million enrollees in 2031.
Table 1. Historical and Projected Medicaid/CHIP Enrollment (in Millions)
Figure 1. Historical and Projected Medicaid/CHIP Enrollment (in Millions)
Medicare enrollment is projected to continue growing steadily. CMS estimates that Medicare beneficiaries totaled 63.6 million in 2022. By 2031, Medicare enrollment is expected to climb to 76.4 million.
Expenditure Projections
Medicaid expenditures are expected to grow by 5 percent on average in 2022−2031. In 2022, the Medicaid annual growth rate was projected to be −2.1 percent. Following the public health emergency unwinding, average expenditure growth would pick up to 5.6 percent in 2025−2031.
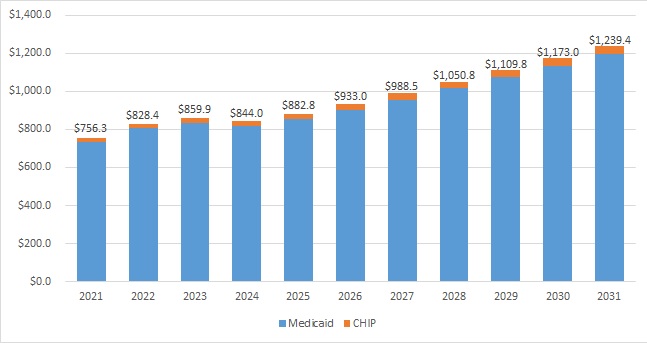
CMS estimated that total Medicaid and CHIP annual spending in 2022 was $828.4 million; by 2031, it is projected to hit $1.2 trillion. For context, private health insurance is projected to reach nearly $2.1 trillion in 2031.
Table 2. Historical and Projected Medicaid/CHIP Expenditures (in Billions)
Figure 2. Historical and Projected Medicaid/CHIP Expenditures (in Billions)
Medicare spending is projected to grow to more than $1.8 trillion in 2031 from $944.2 million in 2022. During this time, average annual expenditure growth is projected to be 7.5 percent. In 2022, spending growth dropped to 4.8 percent compared with 8.4 percent in 2021 because fee-for-service beneficiaries were using fewer emergency department services and as a result of reinstated payment rate cuts associated with the Medicare Sequester Relief Act of 2022.
Medicaid Expenditure Projections by Category
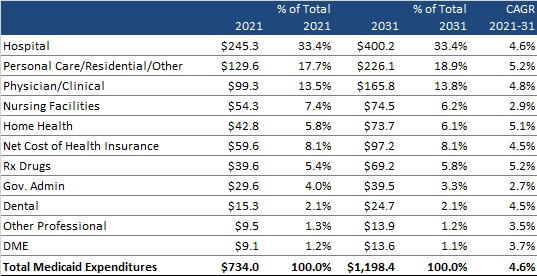
CMS provides a historical and projected breakdown of expenditures by category for Medicaid only (CHIP is bundled with Department of Defense and other public spending). Table 3 summarizes the projected change in annual expenditures for several categories of services and other expenditures. It also shows each category’s percentage contribution to total Medicaid expenditures and the compounded annual growth rate (CAGR) in 2021−2031 for each category of spending. Hospital spending, personal care/residential/other, and physician/clinical expenditures are projected to continue to be the largest contributors to overall Medicaid expenditures, together equaling approximately 65 percent of total expenditures in 2021 and a projected 66 percent in 2031.
Table 3. Historical and Projected Medicaid-Only Expenditures by Category, 2021-2031 (in Billions)
This week, our In Focus checks in on the Medicaid unwinding work and key issues HMA experts are watching as more states resume their normal policies and processes for determining eligibility. A total of 19 states started disenrollments effective for April or May coverage, and 22 additional states plan to start ending coverage this month. States are scheduled to submit the next monthly report by June 8, 2023.
Background
As explained in earlier In Focus articles, (January 12, 2023; November 12, 2022; and April 6, 2022) federal COVID-19 relief laws allowed states to receive higher federal funding for Medicaid as long as the state did not terminate Medicaid coverage for anyone enrolled in Medicaid during the public health emergency (PHE). One result of the continuous coverage policy was sustained growth in Medicaid enrollment; more than 21 million additional individuals were continuously enrolled in Medicaid for up to three years between February 2020 and March 2023. In December 2022, Congress ended the Medicaid continuous coverage policy after March 31, 2023. States were allowed to begin processing redeterminations as early as February 2023 and start disenrolling ineligible individuals as early as April 2023.
Preparations for the Medicaid unwinding have been under way for well over two years. The Centers for Medicare & Medicaid Services (CMS), states, Medicaid health plans, providers, beneficiary advocates, and other interested stakeholders have been working to ensure that the policies, outreach, and assistance are in place to support this massive eligibility renewal and redetermination initiative.
What Do We Know… Or Not Know?
Most of the available forecasts project between 10-15 million enrollees will lose Medicaid coverage. The Health Management Associates (HMA) insurance mix model projects that more than 10 million of the approximately 90 million Medicaid enrollees are at risk for disenrollment. HMA’s model illustrates the variety in state approaches to managing the resumption of eligibility redeterminations as well as key insights related to the differential impact by Medicaid eligibility categories.
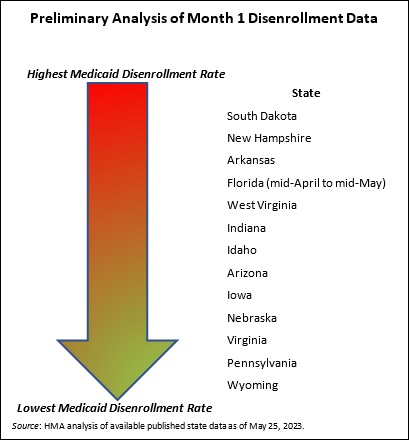
Based on published information, the number of individuals who were disenrolled from Medicaid in April through May is likely to approach 500,000. In these early days of the unwinding period, HMA experts are closely reviewing the reports and engaging with key stakeholders in individual states. Several issues already are garnering more attention, such as the impact on child enrollment, churn and experiences in states using the extended reconsideration period flexibility, among others. Stakeholders will want to monitor how these and other program nuances evolve over the next year.
We do not yet have robust or consistent data from the states that have resumed their normal processes for determining eligibility. States must submit disenrollment reports to CMS each month, and CMS must publish this information. The states are not, however, required to publish this information on their website. While some states have chosen to publish the data or plan to do so, there is no consistent approach to the specific data states post. For example, while most states publishing a state data dashboard are sharing the number of renewals they are processing each month, only slightly more than half also are sharing the number of renewals resulting in coverage terminations. CMS is not expected to publish the state data before the end of June. Once this information is available, the state unwinding reports may provide a more comprehensive and consistent picture of enrollment over the next year.
In addition, the total number of “procedural terminations” currently is difficult to determine. Lack of consistent public reporting creates gaps in the data about the number of individuals disenrolled because they did not provide a timely response to the state’s request for more information (or for other procedural reasons). As Medicaid stakeholders know, the procedural disenrollment number is critical because these individuals could still be eligible for the program.
Early disenrollment numbers should be analyzed carefully and in the context of the state. As noted earlier, the full eligibility renewal and disenrollment reports are unavailable at this time. We do know, however, that the available data is best analyzed in the context of the state’s unwinding plan (e.g., how the state is sequencing its eligibility reviews). The sequencing, pace, staffing, messaging consistency, partner outreach and assistance, and other factors will result in variation in state experiences. States are actively analyzing the data as the information is released and considering course corrections that may be needed, which could affect enrollment.
Ongoing federal and state collaboration is improving preparations and allowing partners to address concerns as they arise. CMS and states have been transparent about the magnitude of the Medicaid unwinding and the fact that challenges will be inevitable throughout this process. The experiences reported by the first tranche of states to begin their unwinding period reinforce those points. They also provide important lessons for states that are or will shortly resume normal eligibility operations.
What to Watch
HMA’s experts are working with states, Medicaid health plans and their partners, providers, and advocacy organizations to identify and implement solutions to some of the known challenges. We also are looking ahead to forthcoming data, qualitative input, and other important developments that may inform federal and state policies and operations beyond the unwinding period.
Unwinding trends. Though it is too early to definitively identify trends, HMA experts are monitoring the early state data, and we are prepared to analyze the CMS reports once they are published. We anticipate the CMS published data could be more instructive regarding the impact of the unwinding on enrollment, including states or regions that could benefit from additional outreach and assistance strategies, disproportionate impacts on certain demographic groups, new flexibilities that states may want to consider, and steps that health plans, hospitals and health systems, providers, and other partners could advance.
State operational plans. As of late May, CMS officials reported they have not asked any state Medicaid agency to develop a corrective action plan related to the unwinding; however, this does not mean that federal officials do not have concerns about the experiences and data being reported out of certain states. States, their business partners, and advocates will all benefit from monitoring shifts in state plans, potential future CMS resources and direction to states such as additional reporting or modifying eligibility processes.
Coverage Program Transitions. Significant attention has been appropriately placed on the Medicaid disenrollment numbers. HMA experts also are closely watching for new data on the number of individuals who successfully transition and enroll in qualified health plans offered in the Health Insurance Marketplaces. In the short term, the Medicaid unwinding could have a notable impact on total enrollment in Marketplace plans as well as provider payer mix. This could affect longer-term policy, strategy, and operational decisions for officials at the federal and state levels, managed care organizations, providers, and other stakeholders. For example:
Health insurers should assess the opportunity to participate in the Marketplace program. Other insurers may need to develop new strategies to remain competitive in the Marketplace.
Providers have similar assessments to conduct related to changes in the number of uninsured people to whom they deliver care, as well as their payer mix and the Marketplace plan networks in which they participate.
Policymakers may revisit Marketplace regulations and standards in response to enrollment growth, enrollee demographics, and acuity of enrollees in Marketplace plans.
Medicaid agencies, health plans, all types of Medicaid providers, and advocacy organizations should continue to analyze their immediate needs during the Medicaid unwinding. They should also be planning to identify and incorporate lessons from this transition period, as well as preparing for policy and operations changes in the post-unwinding environment.
HMA: What We’re Watching
On June 8, 2023, the Health Care Payment Learning & Action Network (LAN) will hold a virtual meeting focused on accountable primary care. The LAN — an initiative supported by the Centers for Medicare & Medicaid Services (CMS) Innovation Center — is a group of public and private health care leaders that provide thought leadership, strategic direction, and ongoing support to accelerate our care system’s adoption of alternative payment models (APMs). During the session, CMS Administrator Chiquita Brooks-LaSure and the Innovation Center’s Deputy Administrator and Director Liz Fowler will share their vision for accountable primary care.
Over the past several months CMS leaders have discussed their intent to accelerate the transition to value-based care and more accountable primary care. They have identified key principals and hinted at certain components of a potential new primary care model. Additionally, the Innovation Centers’ earlier strategy documents have highlighted the imperative to include payers beyond Medicare, importantly Medicaid and commercial insurers, in models to achieve person-centered accountable and equitable care.
This meeting is notable because the Innovation Center’s models can drive transformational shifts in health care delivery and payment across public and private payers at the system and practice levels. Providers, health systems, insurers, and other interested stakeholders will want to closely monitor the LAN discussion for more information about CMS’ evolving thinking and future opportunities related to a potential model for accountable primary care. HMA experts are available to work with health care organizations and stakeholders to interpret and respond to developments flowing from the LAN session.
Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth
Pre-Conference Workshop: October 29, 2023 Conference: October 30−31, 2023 Location: Fairmont Chicago, Millennium Park
Health Management Associates has announced the preliminary lineup of speakers for its sixth annual conference, Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth.
Hundreds of executives from health plans, providers, state and federal government, investment firms, and community-based organizations will convene to enjoy top-notch content, make new connections, and garner fresh ideas and best practices.
A pre-conference workshop, Behavioral Health at the Intersection of General Health and Human Services, will take place Sunday, October 29.
Confirmed speakers to date include (in alphabetical order):
Jacey Cooper, State Medicaid Director, Chief Deputy Director, California Department of Health Care Services
Kelly Cunningham, Administrator, Division of Medical Programs, Illinois Department of Healthcare and Family Services
Karen Dale, Chief Diversity, Equity, and Inclusion Officer, AmeriHealth Caritas
Peter Lee, Health Care Policy Catalyst and former Executive Director, Covered California
John Lovelace, President, Government Programs, Individual Advantage, UPMC Health Plan
Julie Morita, MD, Executive Vice President, Robert Wood Johnson Foundation
Anne Rote, President, Medicaid, Health Care Service Corp.
Drew Snyder, Executive Director, Mississippi Division of Medicaid
Tim Spilker, CEO, UnitedHealthcare Community & State
Stacie Weeks, Administrator/Medicaid Director, Division of Health Care Financing and Policy, Nevada Department of Health and Human Services
Lisa Wright, President and CEO, Community Health Choice
Publicly sponsored programs like Medicare, Medicaid, and the Marketplaces are leading the charge in driving value, equity, and growth in the U.S. healthcare system. This year’s event will highlight the innovations, initiatives, emerging models, and growth strategies designed to drive improved patient outcomes, increased affordability, and expanded access.
Early bird registration ends July 31. Group rates, government discounts, and sponsorships are available.
HMA is pleased to welcome new experts to our family of companies in April 2023. This diverse team brings significant expertise in Medicare, Medicaid, regulatory strategies, and managed care, strengthening HMA’s capabilities in healthcare consulting across areas like actuarial support, regulatory compliance, and strategic leadership in Medicare Advantage and Medicaid programs.
This week our In Focus section reviews the Illinois Healthcare Transformation 1115 Waiver Extension request, posted for review on May 12, 2023.
In pursuing this waiver extension, Illinois joins a growing list of states taking advantage of new Centers for Medicare & Medicaid Services (CMS) policy flexibilities to address health-related social needs (HRSNs) through Medicaid and test community-driven initiatives that are focused on improving health equity, improving access to care, and promoting whole-person care.
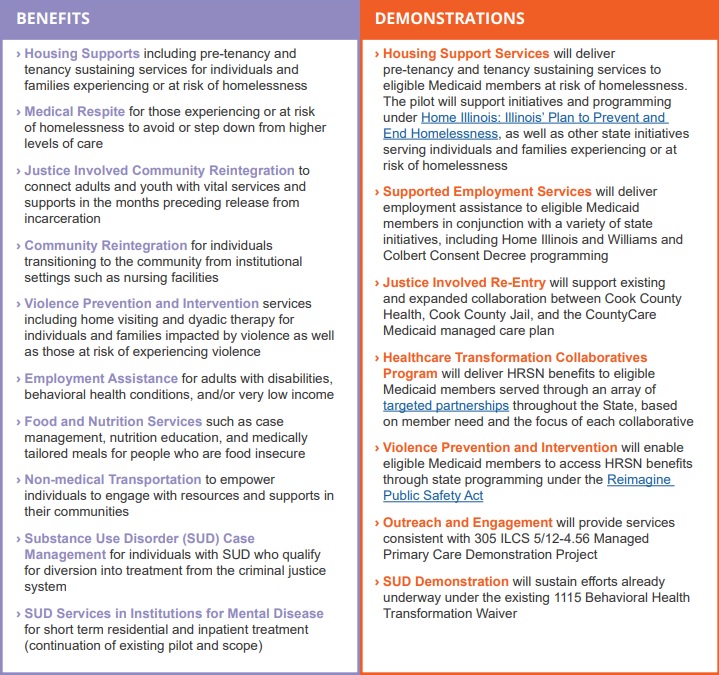
The Illinois waiver incorporates two of the most significant new opportunities in the CMS demonstration waiver flexibilities by proposing to incorporate housing supports for people who are experiencing or at risk of homelessness. The waiver also would extend community reintegration services for justice-involved adults and youths for up to 90 days before their release from incarceration. For a full list of proposed benefits and demonstrations, see Table 1.
Table 1. Summary of Illinois Medicaid 1115 Waiver Extension
The Illinois waiver represents an unprecedented opportunity to demonstrate the long-term, positive impact of providing HRSN services to achieve health equity and create a sustainable, community-driven system for delivering those services. The demonstration proposes to offer a range of HRSN services that are focused on the unmet needs of people who are homeless and housing insecure, are justice-involved, have behavioral health conditions, are pregnant, are unemployed, are food insecure, and/or have been exposed to violence or are at risk of violence with the goal of eliminating health disparities.
The waiver projects a five-year total of $4.4 billion in HRSN services expenditures and another $800 million in HRSN-related infrastructure, indicating Illinois’ long-term commitment to healthcare transformation and to building an equitable, accessible, and high-quality delivery system.
This week’s In Focus is the second in a two-part look at the Centers for Medicare & Medicaid Services’ (CMS’s) recently proposed changes to the Medicaid program. Last week we covered CMS’s proposed changes to the federal Medicaid managed care regulations (CMS-2439-P). This week we review the Medicaid Access to Care proposed rule (CMS-2442-P).
As we discussed last week, the managed care and access to care rules include significant changes to core structural and financing aspects of the Medicaid program. Though state agencies, providers, health plans, consumer groups, and other stakeholders will want to understand the distinct requirements and expectations in each rule that apply to them, the proposed changes cannot be viewed in isolation.
The Access to Care rule addresses a range of challenges that shape the experience of Medicaid enrollees, regardless of whether they are in managed care programs or traditional fee-for-service (FFS). The proposed policy changes also are designed to create an updated federal framework for Medicaid’s home and community-based services (HCBS) programs. These proposals come at a pivotal time, as states are facing workforce shortages, particularly among HCBS direct care workers (DCWs).
The remainder of this In Focus delves into notable components of the proposed changes and includes analysis of the implications of these policies for stakeholders. CMS will benefit from stakeholder input; the deadline for submitting comments is July 3, 2023.
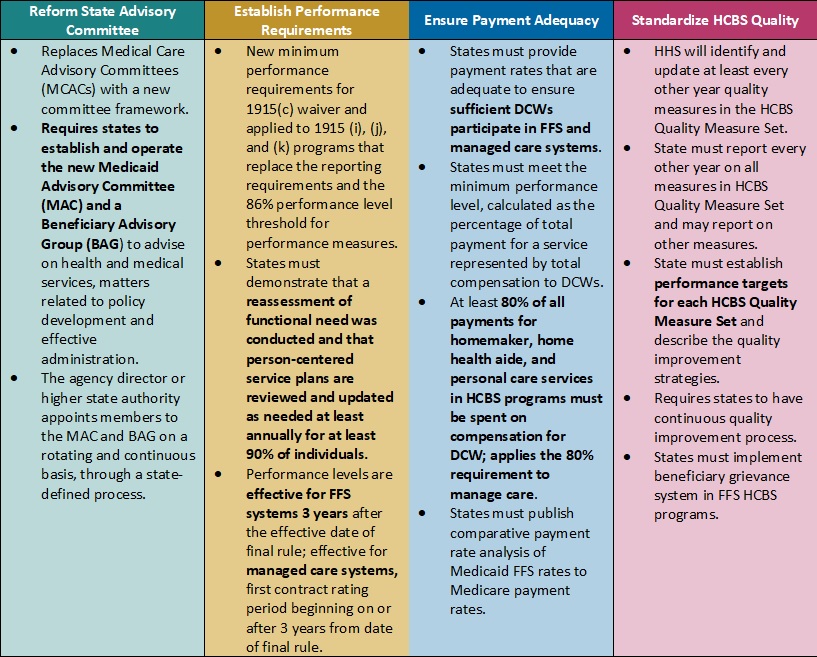
Table 1. Access to Care Regulations: Overview of Proposed Changes
Key Themes and Considerations
Ensuring Payment Adequacy for Key HCBS Services Experiencing Workforce Shortages. One of the most notable proposed changes that would directly impact DCWs is a requirement that at least 80 percent of Medicaid payments be spent on compensation. The proposed rule would apply to homemaker, home health aide, and personal care services, as they represent a large portion of HCBS services that DCWs provide. The proposal is based on feedback from states that have implemented similar provisions, which have ranged from 75 to 90 percent compensation requirements.
CMS specifically seeks stakeholder feedback on the percentage that should be adopted. This policy provision also is important from an equity perspective, given that 90 percent of DCWs are women and 60 percent are members of racial or ethnic minority populations. However, increased or mandated DCW rates may make it difficult for HCBS providers to sustain their businesses as they manage the increased administrative pressures of electronic visit verification, the complexity of filing claims for managed long-term services and supports (MLTSS), and the additional work that HCBS quality measurement may create. Smaller HCBS providers, some of which may have deep cultural expertise, may struggle to sustain themselves and meet these requirements.
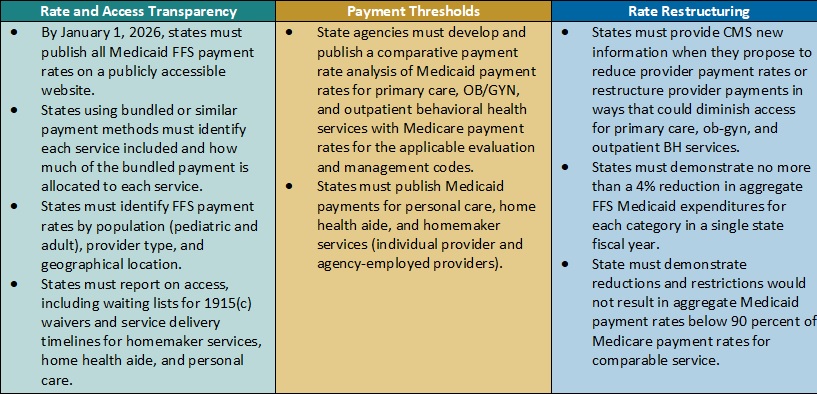
Table 2. Access to Care Regulations: Snapshot of Proposed Rate, Access, and Payment Changes
Payment Alignment. CMS is seeking to align access to care strategies and payment rate transparency more closely across the FFS and managed care delivery systems. The proposed rule includes several changes that CMS has developed achieve this goal. For example:
CMS plans to require that states publish more detailed rate information in a consistent format. States, health plans, providers, and other interested stakeholders will want to consider the implications by delivery system. Additional transparency requirements could create a new opportunity to understand rates across payers and states and use this information in addressing access challenges for services.
The proposed rule also would require extensive comparative analysis of Medicaid FFS rates and Medicare rates. CMS proposes to use Medicare non-facility payment rates as a benchmark to determine if states are meeting federal Medicaid access State analyses will be vital to CMS oversight as well as advocacy efforts within states to monitor and update FFS rates as needed.
Strengthening the Focus on Quality in State HCBS Programs. Over the last several decades, states and Medicaid stakeholders have made significant progress toward increasing participation in HCBS programs and community integration initiatives to counter Medicaid’s institutional bias. CMS is proposing more consistency in the expectations and reporting for HCBS quality measures to further the impact and create a consistent foundation for the recently mandated HCBS quality initiatives starting to take root.
In the short-term, the proposed changes will require states, and likely downstream providers and Medicaid agencies, to immediately change their quality reporting policies and systems. States and their stakeholders will want to map out processes for cyclical updates to HCBS quality measures, including cross-walking the future measures with existing ones, making systems changes, and updating dashboards. Targeted attention and focus will be needed to identify realistic HCBS performance targets that yield successful improvement strategies in the midst of a workforce crisis. Longer term, it will be necessary to map out when updates and reporting will be required to strengthen the rigor and accountability for state performance in the HCBS quality measure set, as well as reinforce the information available to make policy, clinical, and operational improvements to Medicaid programs.
HCBS Access Measurement. CMS is proposing new FFS HCBS payment and access transparency requirements to ensure compliance with Medicaid provider payment rules that require payments to be adequate to enlist at least the same number of providers that the overall geographic population can access. Because the targeted HCBS services do not have a comparable Medicare rate, CMS proposes implementation of a payment rate disclosure approach that would standardize data and monitoring across service delivery systems, with the goal of improving access. In addition to proposed payment transparency changes, CMS proposed new reporting on HCBS waiver waiting lists and timelines for the start of related services once authorized.
These new reporting requirements will provide stakeholders with more information to benchmark their state’s experience with other providers across the nation. This information could be influential to policymakers and legislators and help uncover some of the core contributors to our nation’s HCBS workforce shortage.
Improving Health Equity with Medicaid Beneficiary Input. CMS proposes overhauling the scope and membership of the state Medical Care Advisory Committee. The new Medicaid Advisory Committee (MAC) would continue to advise the state on health and medical matters and play an expanded advisory role on matters of policy development and effective administration of the program. CMS also plans to require that states establish a Beneficiary Advisory Group (BAG) composed of current or past Medicaid beneficiaries. A subset of BAG members would serve on the MAC to ensure their perspectives are integrated into the committee’s recommendations to states.
Under the new federal requirements, MAC representatives could have greater relative input and influence on policies and actions each state Medicaid agency advances. Medicaid stakeholders will want to ensure the MAC’s minimum federal requirements support effective structures and processes in states.
What’s Next
CMS plans to reframe Medicaid access as one of three parts of the continuum of care, along with enrollment and maintenance of coverage. The proposals in the Access to Care rule would have a meaningful impact on the volume and type of data available to evaluate the relationship between Medicaid payment rates and access across all delivery systems.
States, managed care organizations, providers, Medicaid enrollee advocacy organizations, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. They also can use this time to begin planning and determine which resources and tools they may need to prepare for implementation of changes across delivery systems in the Medicaid program.
HMA’s experts are taking a wholistic approach to reviewing the Access to Care and Managed Care proposed rules in tandem and identifying key points of intersection.
For more information on the access to care proposed rule, contact our experts below.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
The end of the Public Health Emergency on May 11, 2023 is likely to mark a transitional point in the rapidly evolving arena of virtual care services and not a dramatic end of coverage. Coverage of virtual care services will continue to evolve significantly over the next five years given the exponential growth in the public’s awareness of, and comfort with, these services — all hastened by the COVID-19 Federal Public Health Emergency.
The U.S. Congress and the Centers for Medicare and Medicaid Services (CMS) used its authority during the PHE to significantly expand Medicare coverage for virtual care services, covering telehealth visits in urban areas and from patient’s homes. In addition, Medicare began covering a wide range of clinical services virtually such as behavioral health and physical therapy; it also expanded coverage for different service delivery modalities to include audio-only visits. As a result of the changes, Medicare became a leading payer for virtual care nationally between 2020 and 2022. Over this same period, private insurers and state Medicaid programs largely followed Medicare’s lead by expanding their own virtual care coverage.
One of the consequences of the PHE is that most payers have embraced Medicare’s basic definitional structure for types of virtual care services. As a part of this typology, virtual care services are divided into two general buckets of services: telehealth visits (physician office visits conducted via audio and video technology), which are typically prohibited by statute in urban areas or a patient’s home; and Communication Technology-Based Services (CTBS) which can be conducted anywhere. CTBSs include: remote patient monitoring (RPM); virtual check-ins (brief patient-to-clinician exchanges); e-visits (online portal or email visits); and e-consults (clinician to clinician interaction).
With the end of the PHE on May 11, Medicare coverage of virtual care services and coverage offered by other payers will change. The details and scope of this change have many stakeholders concerned and confused. HMA has a keen sense for which virtual care services may get a new lease on life in the coming months and which are likely to be hotly debated in the years ahead. The one certainty is that the last 3 years have altered the landscape for virtual care services for years to come.
Shift in Virtual Care Landscape
As a result of the statutory geographic limitations and restrictions placed on traditional fee-for-service (FFS) Medicare coverage, use of telehealth services was minimal most of the last decade, with only one-quarter of 1 percent (0.25%) of beneficiaries in FFS Medicare using virtual care services.[1] Even among Medicare Advantage plans and Medicare Accountable Care Organizations (ACOs), neither of which which face the same restrictions, virtual care was utilized very rarely before 2019.
This sluggish use of telehealth was radically altered when HHS used its PHE authority to relax constraints on the use of use virtual care services by Medicare beneficiaries and providers.[2],[3] Among the most consequential changes made by policymakers at the outset of the PHE were:
Enabling telehealth services to be provided anywhere (e.g., urban areas and patients’ homes);
Allowing Federally Qualified Health Centers (FQHC) and Rural Health Clinics (RHC) to conduct virtual care services;
Granting various types of clinicians permission to deliver virtual care services;
Enabling new patients to receive virtual care services;
Authorizing audio-only services;
Permitting telehealth services for more than 200 different types of clinical services (e.g., mental health, emergency department, physical and occupational therapy, critical care, inpatient care);
Relaxing HIPPA rules to enable the broad use of smartphones for virtual care.
Due to these policy changes, rates of virtual care skyrocketed during the PHE (Figure 1). In April of 2020 the number of Medicare claims for any type of virtual care service exceeded 9 million, while 2019 the number of these services provided monthly never exceeded 100,000 (Figure 1). On an annual basis, from 2019 to 2021 the number of virtual care visits jumped from roughly 1 million to 39 million and the number of unique beneficiaries receiving these services increased from 300,000 to nearly 12 million.
Figure 1: Number of Virtual Care Service Visits, Number of Unique Medicare Fee-For-Service Beneficiaries, and Number of visits per Utilizer by Month, December 2019 to December 2021.
Source: HMA analysis of CMS’s 100 percent Medicare Fee-For-Service Claims data for 2019, 2020, and 2021.
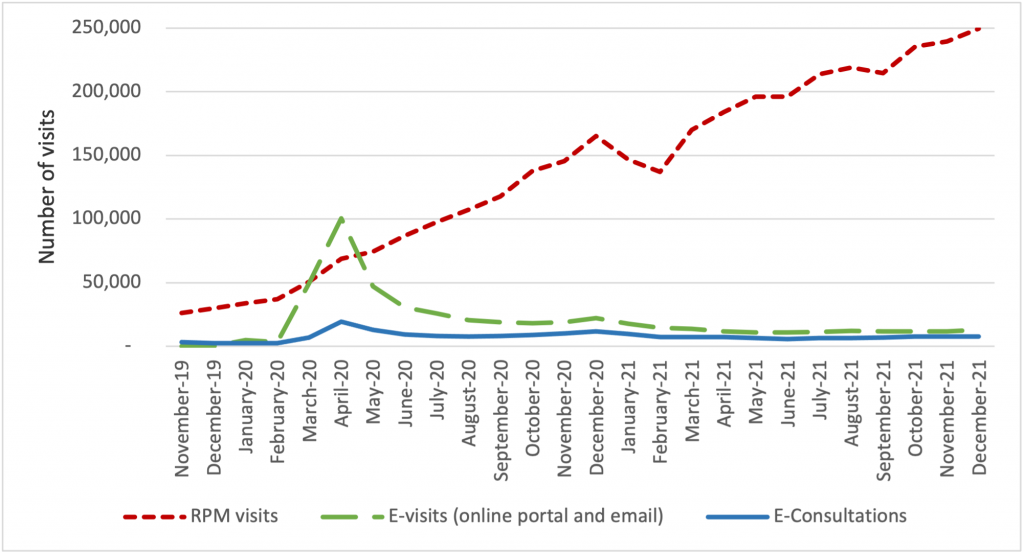
The growth of virtual care services has largely been driven by an increase in telehealth visits, but we observe important trends in the use of CTBSs, as well. In late 2021, more than 90 percent of visits were associated with telehealth, while 10 percent were associated with CTBSs. Early in the PHE, all of these service types experienced an initial, abrupt increase in use (Figure 2). By contrast, the growth in the use of remote patient monitoring (RPM) has been continuous since 2020. The growth in use of RPM reflects the general movement of services into patients’ homes and has been accelerated by specialist such as cardiologists and endocrinologists beginning to leverage the power of RPM. We expect greater diffusion and use of RPM and other CTBSs in the next five years.
Figure 2: Number of Virtual Care Service Visits for Remote Patient Monitoring, Virtual Check-ins, E-visits, and E-Consultations by Month, December 2019 to December 2021.
Source: HMA analysis of CMS’s 100 percent Medicare Fee-For-Service Claims data for 2019, 2020, and 2021.
Policies temporarily in place until the end of 2024
During the PHE, Congress made critical long-term changes to Medicare’s coverage of virtual care services that continued to spur the use of these services and offer access to care for beneficiaries. In 2021, Congress changed the law to permanently allow Medicare beneficiaries to receive behavioral/mental telehealth services regardless of location (urban or rural) and for this care to be available to patients in their own homes.
In 2022, Congress severed the link between the PHE declaration and Medicare coverage policies for virtual care services, extending those benefits through the end of calendar year 2024. We expect that coverage for all telehealth services will receive considerable attention from federal policymakers and stakeholders towards the end of 2024.
Immediate impact of expiring policies
Certain aspects of Medicare’s virtual care policies will, however, terminate May 11, 2023, when the PHE declaration comes to an end. Several of the expiring policies have a broader impact beyond the Medicare program, affecting patients insured by private payers and State Medicaid programs.
Specifically, when the PHE ends, policymakers will need to address the following anticipated changes:
The Office for Civil Rights (OCR) will return to imposing penalties on providers who violate the provisions of the Health Insurance Portability and Accountability Act (HIPAA) by using public-facing remote communication technologies which are not HIPAA-compliant. This may prohibit the use of some of the most common smartphone-based video conferencing tools for health care visits.
Medicare beneficiaries without an existing relationship with a clinician will be unable to receive CTBSs such as RPM, virtual check-ins, and e-visits.
Providers will no longer be allowed to provide virtual care services across state lines, because most state medical licensure boards will return to pre-PHE policy.
Federal rules from the Drug Enforcement Agency (DEA) may revert to the pre-PHE requirement that clinicians establish a patient-provider relationship in-person before being permitted to prescribe controlled substances for substance use disorder treatment.
Potential policy changes occurring before 2025 As explained earlier, Medicare coverage for many virtual care services will remain in place for the next 19 months. Before the end of 2024, Congress will need to address several policy questions, and among the most widely debated are whether to:
Restore Medicare’s statutory prohibition on telehealth services being delivered in urban areas or in home settings;
Allow Federally Qualified Health Centers and Rural Health Clinics to provide telehealth services to Medicare beneficiaries; or
Continue to cover audio-only telehealth visits under Medicare.
Lawmakers will look to payers, patients, and providers for feedback before making these policy decisions. Among the most critical pieces of information they will also consider will be the results of the study Congress has required of HHS regarding trends in the use of virtual care. This study’s final report is due in 2026, which has led some to speculate that Congress will delay action on virtual care coverage policy until then. In the meanwhile, we expect HHS will be assessing the overall volume of virtual care use, who is using which types of services, and the levels of related fraud and abuse.
Looking Ahead
In the United States, our experience during the acute phase of the pandemic demonstrated that patients and providers are more receptive than previously thought to utilizing digital technologies for the delivery of care. This experience may also influence policymakers’ decisions about reimbursement and coverage of wearable devices, as well as other cutting-edge tools that rely on artificial intelligence or machine learning.
HMA believes payers and providers alike can take steps now to strategically prepare for the still evolving and growing landscape of digital health care.
Based on the various changes that have occurred in the virtual care environment over the last 3 years, we are intently watching several areas of potential change in the practice of medicine and the ways payers set coverage policy. Below are some of the trends we anticipate in the years ahead:
Continued use of virtual care services at levels observed in 2021.
An expansion of CMS’s programs to protect against fraud and abuse related to virtual care.
Notable growth in the use of RPM, and related services for physical and occupational therapy services.
The proliferation of innovative home-based screening and testing technologies. We anticipate payers will encourage the use of these at-home tests for things like kidney function, liver function, and colorectal cancer screening in order to limit care delivery in higher cost settings.
Growth in “virtual-first” insurance plans, where patients are encouraged to use virtual care first – prior to being seen in person. As these plan options expand, we anticipate virtual care use will rise, and reimbursement rates will begin to change.
Virtual care services are primed for additional growth and HMA is working with a wide variety of payers, providers, and foundations to develop strategies for adapting to state and federal rules and regulations related to virtual care. Changes in this landscape will hinge on research CMS will complete by the end of 2026, and coverage decisions made by states and commercial payers. HMA is well positioned to assist stakeholders with work in this area and can leverage access to Medicare and Medicaid claims data to conduct health services research to illustrate geographic variations in the use of virtual care.
If you have questions on how HMA can support your agency before or after the end of the PHE, please contact our experts below.
[2] Centers for Medicare & Medicaid Services. Medicare telemedicine health care provider fact sheet. March 17, 2020. https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
[3] HHS Administration for Strategic Preparedness & Response (ASPR). https://aspr.hhs.gov/legal/PHE/Pages/default.aspx
This week, our In Focus section reviews CMS’s proposed changes to the federal Medicaid managed care access, finance, and quality regulation (CMS-2439-P). A future In Focus will take a closer look at the proposed changes to the federal Medicaid access to care regulation (CMS-2442-P), which also has significant implications for state Medicaid programs.
On April 28, 2023, the Centers for Medicare & Medicaid Services (CMS) unveiled two significant and related proposed rules addressing Medicaid managed care access, finance, and quality requirements. Together these proposed rules signal a new era of accountability and transparency in the Medicaid program. They also strengthen beneficiaries’ role in influencing the policies and administration of state Medicaid programs.
Table 1 identifies a few of the key themes and issues addressed in the Medicaid managed care proposed rule. The deadline for submitting comments to CMS is July 3, 2023.
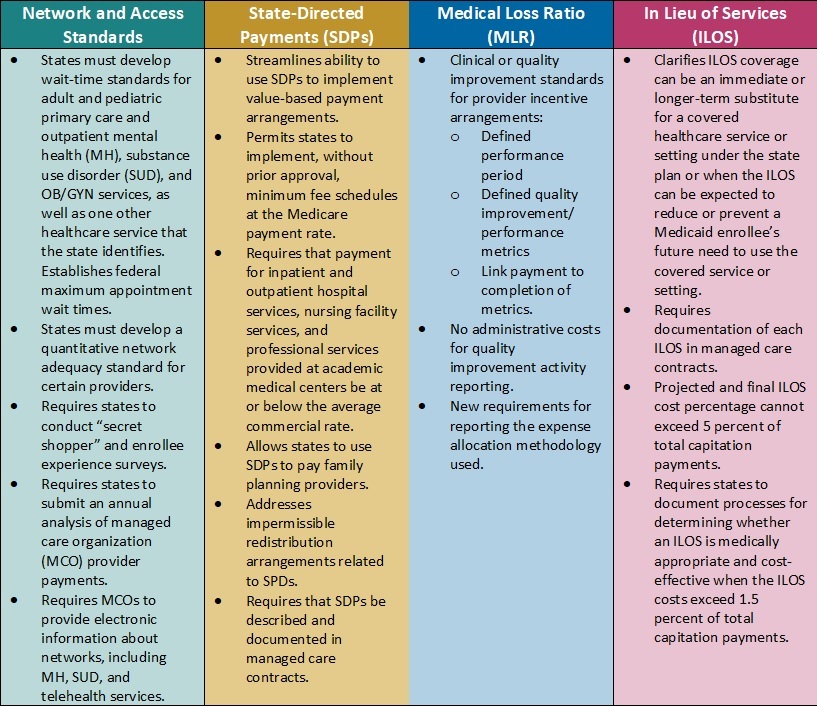
Table 1. Medicaid Managed Care Proposed Rule: Snapshot of Proposed Changes
Key Themes and Considerations
Payment Ceilings May Accelerate Value-Based Payment Arrangements. Current federal regulations allow states to direct managed care organizations (MCOs) to pay providers according to specific rates or methods. States have used these directed payment arrangements to set minimum payment rates for certain types of providers or to require participation in value-based payment (VBP) initiatives.
In the proposed rule, CMS calls for establishing an upper limit for these payments. Specifically, the agency plans to limit the projected total payment rates to the average commercial rate (ACR) for inpatient and outpatient hospital services, nursing facility services, and qualified practitioner services at academic medical centers that states include in state-directed payment (SDP) arrangements. The ACR limit, in concert with the proposed SDP documentation and reporting, is among the most significant and complex proposed changes in the rule.
Considerations: The proposed changes represent a strong federal regulatory push to accelerate movement to VBP in Medicaid, which provides states with new levers to drive value in their Medicaid delivery systems. It also means that MCOs, providers, and other stakeholders will need to navigate and help inform the policies and contractual arrangements that will flow from the pending changes. For example, states may need to reflect on the following considerations:
Whether the proposals will require them to reduce reimbursement
Whether they will need to develop new value-based arrangements through SDPs and how these policies will be structured
What outcomes they might need to prioritize
How transparency in reporting provider-level payments could affect non-federal funding and SDP initiatives
Updated Approach to in Lieu of Services (ILOS) Facilitates Whole-Person Care. In January 2023, CMS issued a State Medicaid Director Letter (SMDL#23-001) advising states of the option to use the ILOS authority in Medicaid managed care programs to reduce healthcare inequities and address unmet health-related social needs (HRSNs), such as housing, food insecurity, and intimate partner violence. The proposed Medicaid managed care rule would expand upon and codify in regulation that guidance.
Considerations: Although the ILOS proposal adds reporting requirements and guardrails to address fiscal accountability, overall, the updated policy signals CMS’s willingness to support innovative state approaches to meet a continuum of beneficiary needs, including HRSNs that affect the social drivers of health. Notably, CMS advises that the substitution of an ILOS for a state plan service or setting should be cost-effective but does not need to be budget-neutral. States also can specify that an ILOS can be an immediate or longer-term substitute for a state plan service or setting.
States could pursue a variety of options under CMS’s revised ILOS framework. State Medicaid agencies and their partners can collaborate on ILOS strategies that will allow them to make further progress toward reducing healthcare inequities, as well as fulfill their quality strategy goals and objectives.
New Standards for Medical Loss Ratio Strengthen Link to Performance Improvement. Existing federal regulations require Medicaid managed care plans to report their medical loss ratio (MLR) to states annually, and, in turn, states must submit a summary of those reports to CMS. Many state MCO contracts require plans to comply with provider incentive and bonus policies; however, MCOs infrequently make incentive payments contingent on the provider meeting quantitative clinical or quality improvement standards.
Consistent with the healthcare sector’s transition toward value-based care, CMS proposes to strengthen the link between an MCOs incentive payment to a provider and the provider meeting defined quality improvement or performance metrics. Additionally, contractual language between MCOs and providers will need to more explicitly identify the dollar amounts tied to successful completion of these metrics. Only incentive payments based on quality improvement will be considered incurred claims when plans calculate their MLR; administrative costs cannot be included in quality improvement activity reporting.
Considerations. The proposed requirements are expected to add more transparency to negotiations between Medicaid MCOs and providers. MCOs will retain flexibility to determine the quality improvement or quantitative performance metrics, which carry more weight and accountability in CMS’s revised regulatory framework.
Network Adequacy Requirements Strengthen Link to Access and Rates. CMS also proposes policies that the agency believes will help strengthen Medicaid enrollees’ access to services. For example, the rule would require states to develop wait-time standards for adult and pediatric primary care and outpatient mental health, substance use disorder (SUD), and OB/GYN services, with CMS establishing federal minimum appointment wait times. States also will need to develop a quantitative network adequacy standard, beyond wait times, for certain providers.
Notably, CMS also plans to require states to submit an MCO-level analysis of MCO-to-provider payments. This analysis may provide more insights about the relationship between rates and access to certain types of providers and services. It may also improve alignment in access policies across delivery systems.
Considerations: States and MCOs should expect to need more sophisticated analysis of provider capacity at state and local market levels. This information will be critical in developing network adequacy standards and determining where additional provider support may be necessary. Expanded and new strategies may be needed to ensure compliance with the federal rules and resulting changes to state policies.
What’s Next
Many of CMS’s proposals track closely with many recent recommendations from federal commissions and oversight entities, including the Medicaid and CHIP Payment and Access Commission (MACPAC) and Government Accountability Office (GAO), which may indicate a greater likelihood that CMS will finalize those policies. If they are finalized largely as proposed, the rule will further the Biden Administration’s directional imprint on the Medicaid program.
Within the proposed rules described above, CMS identifies numerous areas where stakeholder input would be beneficial. States, MCOs, providers, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. Stakeholders also may use this time to begin planning for 2024 and determining what resources and tools they may need to prepare for implementation of the final regulations, as well as how their approach may vary based on state-specific factors.
For questions about the rule and how HMA’s team of experts can support your organization’s response, please contact our experts below.
HMA’s five-part 1115 Justice Waivers: Building Bridges of Health for Persons Leaving Carceral Settings webinar series is designed to help plans and other stakeholders improve the long-term health outcomes of individuals leaving carceral settings. This webinar focused on the carceral settings operational healthcare practices, including intake screenings to aid in risk assignment and facilitate community re-entry. The 1115 justice waivers allow Medicaid programs to support in-carceral care, but to optimize resources, systems need information to translate transition in care best practices to carceral places of service.
HMA consultants with lived leadership experience working inside and outside jails and prisons provided plans and state agencies with a unique perspective on opportunities for transformation.
Learning Objectives:
Establishing Health Care Transitions Across Providers: Methods to improve transitions in care through recognizing carceral facilities as a place of service in the continuum of care.
Health Risk Assessments to Improve Continuity of Care: Utilizing health screening and risk assessments done at intake and throughout incarceration so Medicaid can improve healthcare transitions from jail into the community.
Other webinars in the “1115 Justice Waivers: Building Bridges of Health for Persons Leaving Carceral Settings” series:
This week our In Focus section reviews guidance from the Centers for Medicare & Medicaid Services (CMS), released on April 17, 2023, encouraging states to apply for the new Medicaid Reentry Section 1115 Demonstration Opportunity. The demonstration is aimed at helping improve care for individuals in carceral settings prior to their release.
Background
The United States has approximately 1.9 million individuals incarcerated nationwide. Studies have shown higher rates of mental illness and physical health care needs in incarcerated populations compared to the general population, as well as associations between jail incarceration and increases in premature death rates from infectious diseases, chronic lower respiratory disease, drug use, and suicide.
CMS states that formerly incarcerated individuals with physical and mental health conditions and substance-use disorders (SUDs) typically have difficulty succeeding upon reentry due to obstacles present immediately at release, such as high rates of poverty and high risk of poor health outcomes. These individuals tend to face barriers in obtaining housing, education, employment, and health care access upon release. They often do not seek outpatient medical care and are at significantly increased risk for emergency department (ED) use and hospitalization.
Purpose and Goals
After collecting feedback from stakeholders, including managed care organizations, Medicaid beneficiaries, health care providers, the National Association of Medicaid Directors, and other representatives from local, state, and federal jail and prison systems, CMS designed the Reentry Section 1115 Demonstration Opportunity. The services covered under this demonstration opportunity should aim to improve access to community resources that address the health care and health-related social needs of the carceral population, with the aims of improving health outcomes, reducing emergency department visits, and inpatient hospital admissions for both physical and behavioral health issues once they are released and return to the community.
The purpose of this demonstration opportunity is to provide short-term Medicaid enrollment assistance and pre-release coverage for certain services to facilitate successful care transitions. The full goals, as quoted from CMS, are as follows:
“Increase coverage, continuity of coverage, and appropriate service uptake through assessment of eligibility and availability of coverage for benefits in carceral settings just prior to release
Improve access to services prior to release and improve transitions and continuity of care into the community upon release and during reentry
Improve coordination and communication between correctional systems, Medicaid systems, managed care plans, and community-based providers
Increase additional investments in health care and related services, aimed at improving the quality of care for beneficiaries in carceral settings and in the community to maximize successful reentry post-release
Improve connections between carceral settings and community services upon release to address physical health, behavioral health, and health-related social needs
Reduce all-cause deaths in the near-term post-release
Reduce number of ED visits and inpatient hospitalizations among recently incarcerated Medicaid beneficiaries through increased receipt of preventive and routine physical and behavioral health care”
CMS encourages states to engage with individuals who were formerly incarcerated when contemplating the design and implementation of their proposal. CMS also encourages states to design a broadly defined demonstration population that includes otherwise eligible, soon-to-be former incarcerated individuals. States have the flexibility to target population, such as individuals with specific conditions, but are encouraged to be mindful of undiagnosed conditions. States should have a plan to ensure incarcerated individuals will be enrolled in Medicaid upon their release, applying for Medicaid no later than 45 days before the day of release.
Reentry Section 1115 Demonstration Opportunity
To receive approval for the demonstration, the state proposal must include in the pre-release benefit backage:
Case management to assess and address physical and behavioral health needs and health-related social needs;
Medication-assisted treatment (MAT) services for all types of SUD as clinically appropriate, with accompanying counseling; and
A 30-day supply of all prescription medications that have been prescribed for the beneficiary at the time of release, provided to the beneficiary immediately upon release from the correctional facility.
In addition to these three services states may include other important physical and behavioral health services to cover on a pre-release basis, such as family planning services and supplies, behavioral health or preventive services, including those provided by peer supporters/community health workers, or treatment for Hepatitis C. CMS is also open to states requesting Section 1115 expenditure authority to provide medical supplies, equipment, and appliances.
The Reentry Section 1115 Demonstration opportunity is not intended to shift current carceral health care costs to the Medicaid program. CMS will not approve state proposals to receive federal Medicaid matching funds for any existing carceral health care services funded with state or local dollars unless the state agrees to reinvest the total amount of new federal matching funds received into activities or initiatives that increase access to or improve the quality of health care services for individuals who are incarcerated.
CMS also expects states to refrain from including federal prisons as a setting in which demonstration-covered prerelease services are provided under the opportunity.
States with approved demonstrations will need to submit an implementation plan, a monitoring protocol, quarterly/annual monitoring reports, a mid-point assessment report, an evaluation design, and interim/summative evaluation reports.
California
California became the first state to receive approval for a Section 1115 waiver amendment earlier this year to provide limited Medicaid services to incarcerated individuals for up to 90 days immediately prior to release. The approval period runs through December 31, 2026, timed with the expiration of the CalAIM Medi-Cal waiver demonstration. California’s reentry demonstration initiative aims to provide health care interventions at earlier opportunities for incarcerated individuals to reduce acute services utilization and adverse health outcomes. The state anticipates it will increase coverage and continuity of coverage for eligible beneficiaries, improve care transitions for beneficiaries as they reenter the community, and reduce morbidity and mortality in the near-term post-release.
Pre-release services include comprehensive care management, physical and behavioral clinical consultation, lab and radiology, MAT, community health worker services, and medications and durable medical equipment. A care manager will be assigned to eligible individuals to establish a relationship, understand their health needs, coordinate vital services, and make a plan for community transition, including connecting the individual to a community-based care manager they can work with upon their release. Additionally, all counties implementing Medi-Cal application processes in jails and youth correctional facilities will “suspend” the Medicaid status while an individual is in jail or prison, so that it can be easily “turned on” when they enter the community.
On April 6, 2023, HMA held a webinar titled, “Medicaid authority and opportunity to build new programs for justice-involved individuals.” The webinar replay is now available. HMA will announce additional webinars on the topic.
This week, our In Focus section reviews the policy changes proposed by the Centers for Medicare & Medicaid Services’ (CMS) on April 10, 2023, for the Fiscal Year (FY) 2024 Medicare Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Acute Care Hospital (LTCH) Proposed Rule (CMS-1785-P). This year’s IPPS Proposed Rule includes several important policy changes that will alter hospital margins and change administrative procedures, beginning as soon as October 1, 2023.
Key provisions of the FY 2024 Hospital IPPS and LTCH Proposed Rule
For FY 2024, CMS proposes to make modifications to several hospital inpatient payment policies. We highlight six proposed policies that are among the most impactful for Medicare beneficiaries, hospitals and health systems, payors, and manufacturers:
the annual inpatient market basket update,
hospital wage index adjustments,
New Technology Add-on Payment (NTAP) program policy changes,
the agency’s call for input on how to best support Safety Net Hospitals,
graduate medical education payments at rural emergency hospitals, and
changes to many cardiovascular-related MS-DRGs.
Stakeholders will have until June 9, 2023, to submit comments to CMS on the contents of this regulation and request for information
1. Market basket update
Proposed Rule: Overall CMS’s Medicare 2024 Hospital Inpatient Proposed Rule will increase payments to acute care hospitals by an estimated $3.3 billion from 2023 to 2024; however, recent trends in economy-wide inflation may alter this estimate by the time the agency releases the Final Rule version of this regulation in August 2023. The primary driver of the estimated $3.3 billion increase in inpatient payments to hospitals is CMS’s proposed 2.8 percent increase in the annual update to inpatient operating payment rates.
HMA/Moran analysis: CMS’s 2.8 percent increase is largely based on an estimate of the rate of increase in the cost of a standard basket of hospital goods, the hospital market basket. For beneficiaries, increasing payment rates will eventually lead to a higher standard Medicare inpatient deductible and increased beneficiary out-of-pocket costs for many other services. For hospitals and health systems, payors, and manufacturers the proposed payment increase (2.8 percent) falls below economy-wide inflation (5-6 percent in recent months) and hospitals are already saying it is insufficient.[1] For this Proposed Rule, data from the third quarter of 2022 was used to calculate the 2.8 percent increase. Importantly, for the FY 2024 Final Rule, CMS will use data through the first quarter of 2023, which we know to include additional growth in economy-wide inflation. As a result,we anticipate the proposed 2.8 percent increase in payment rates may increase slightly by the time rates are finalized later in the year.
2. Hospital Wage Index Adjustments:
Proposed Rule: CMS proposes two wage index policies for FY 2024. First, CMS proposes to continue temporary policies finalized in the FY 2020 IPPS/LTCH PPS final rule to address wage index disparities affecting low-wage index hospitals, which includes many rural hospitals. Second, CMS proposes to include geographically urban hospitals that choose to reclassify into rural wage index areas in the calculation of state-level rural wage index and the calculation of the state-level wage index floor for urban hospitals (referred to as the rural floor policy).
HMA/Moran analysis: The two wage index policies proposed by CMS for FY 2024 will support rural hospitals. The first policy, to continue the low-wage index policy for an additional year beyond the original 4-year plan will allow hospitals with low wage indexes to boost their wage index and their payment rates across all MS-DRGs. Specifically, hospitals with wage indexes below 0.8615 (the 25th percentile across all hospitals) will automatically receive an increase in their wage index by CMS. This policy will bring additional millions of dollars to individual rural hospitals in FY 2024. The second policy, to include the labor data of geographically urban hospitals that choose to reclassify into rural wage index areas within the calculation of the state-level rural wage index and the state-level rural floor will largely benefit rural hospitals. In recent years several large geographically urban hospitals in several markets have chosen to reclassify into rural wage index areas to benefit their Medicare payments. In the past, CMS has not included the labor costs of these hospitals, which tend to have higher than average labor costs in their calculation of the state rural wage index or the rural floor wage index. In making this change, to include the labor costs of the geographically urban hospitals in these calculations, CMS will very likely increase the state-wide rural wage index. This will have the effect of increasing the wage index of many rural hospitals around the country. The overall impact of both proposed wage index policy changes for FY 2024 will be to increase inpatient payment rates to rural hospitals.
3. New technology add-on payments (NTAP):
Proposed Rule: Citing the increased number of applications over the past several years and noting the need for CMS staff to have time to fully review and analyze the applications, CMS proposes two changes to the NTAP application requirements. First, CMS proposes to require all applicants to have a complete and active FDA market authorization request in place at the time of NTAP application submission (if not already FDA approved). In addition, CMS proposes to move the FDA approval deadline from July 1 to May 1, beginning with applications for FY 2025.
HMA/Moran Analysis: CMS’ proposals to change the NTAP application process aim to ameliorate the problem of manufacturers withdrawing applications because they miss the FDA approval deadline. These withdrawals increase CMS’ workload, as the agency reviews some applications multiple times. However, while these proposals provide CMS with more time to review applications, they increase the amount of time some applicants will not receive NTAP payments, depending on the timing of the FDA approval process. The annual NTAP approval cycle and FDA approval deadline create difficulties for manufacturers with products that miss the deadline, which many stakeholders argue creates barriers to access for new technologies. Stakeholders have proposed a variety of potential solutions to these barriers, such as biannual or quarterly NTAP decisions, or extending the conditional approval pathway currently used for certain antibiotic products to all NTAP applications.
4. Safety Net Hospital Request for Information:
Proposed Rule: CMS is seeking public input on the unique challenges faced by safety-net hospitals and the patients they serve, and potential approaches to help safety-net hospitals meet those challenges.
HMA/Moran Analysis: In the 2024 Proposed Rule CMS poses a variety of questions to the public about how safety net hospitals and their patients can be better supported by the Medicare program, both in terms of payment and infrastructure investment. The agency specifically asks stakeholders their opinion on measures that could be used to define safety net hospitals and potentially make differential or additional payments to safety net hospitals. CMS names the safety net index (SNI) developed by the Medicare Payment Advisory Commission (MedPAC) in recent years and the Area Deprivation Index (ADI) developed by the National Institutes for Health (NIH) as the two leading options for defining and potentially reimbursing safety net hospitals. These two methods have several significant differences, including that the SNI is a hospital-level measure based in-part on the volume of cases at a given hospital associated with Medicare beneficiaries that are fully or partially eligible for Medicaid and the ADI is a geographic measure that correlates local socioeconomic factors with medical disparities. HMA has modeled the SNI for hospital stakeholders in the last year and has identified hospitals that would be potential winners and losers if an SNI approach were implemented by CMS.
5. Graduate Medicare Education Training in Rural Emergency Hospitals:
Proposed Rule: CMS proposed to allow Graduate Medical Education (GME) payments for training Rural Emergency Hospitals. Rural Emergency Hospitals are a new provider type established by the Consolidated Appropriations Act, 2021, to address the growing concern over closures of rural hospitals. If finalized, this proposal would allow hospitals converting to REH status and other hospitals newly designated as REHs to receive Medicare GME payments even though they do not have an inpatient facility.
HMA/Moran analysis: If finalized, the proposed policy to allow REHs to offer GME training and to be paid for GME training will enhance access to care in rural areas and will enable hospitals that convert to REHs to expand their capabilities. CMS’s proposal to allow REHs to receive payment based on 100 percent of the reasonable costs for GME training costs allows REHs to operate training programs and to focus new training programs on rural care and outpatient care. This policy, if finalized, will bring additional revenues to hospitals that decide to convert to REHs (thereby relinquishing their inpatient capacity) and will improve access to care for beneficiaries living in rural areas.
6. MS-DRG weights:
Proposed Rule: To set MS-DRG weights for FY 2024 inpatient cases, CMS proposed to use FY 2022 data, which is consistent with pre-pandemic CMS methods. In previous years, CMS had modified its MS-DRG weight calculation to account for high volumes of COVID cases. However, for FY 2024, CMS has returned to its longstanding method of using a single year of data to set MS-DRG weights. In addition, among the various changes CMS has proposed as a part of the 2024 MS-DRG weight setting process CMS has proposed significant changes to many MS-DRGs in the category for diseases and disorders of the circulatory system (Major Diagnostic Category 5).
HMA/Moran analysis: CMS’s return to using a single year of data without COVID modification will be welcomed by many stakeholders, but particularly for those with an interest in short-stay surgical cases. The modifications CMS proposes to make to the MS-DRGs within Major Diagnostic Category 5, which includes numerous cardiovascular MS-DRGs, are likely to be disruptive for many stakeholders initially but over the long term are likely to make CMS coding more consistent with standard clinical practice and per case resource use. For example, CMS is proposing to consolidate five cardiac defibrillator MS-DRGs into three, consolidate three Thrombolysis MS-DRGs into two, and overhaul the family of stenting MS-DRGs. We anticipate that these changes and other proposed by CMS may result in initial coding confusion for hospitals, but that they will slowly adapt throughout 2024.
HMA and The Moran Company work collaboratively to monitor legislative and regulatory developments in the inpatient hospital space and assess the impact of inpatient policy changes on the hospital sector. HMA’s Medicare experts interpret and model inpatient policy proposals and use these analyses to assist clients in developing their strategic plans and comment on proposed regulations. Moran annually replicates the methodologies CMS uses in setting hospital payments and models alternative payment policies to help support its clients’ comments to the rule. Moran also assists clients with modeling for DRG reassignment requests and to support NTAP applications. Typically, these projects run through the summer, to ensure readiness for October deadlines. Finally, many clients find it useful to model payments for different types of cases under different payment scenarios. For example, a client may be interested in how payments for COVID-19 cases may change after the expiration of the Public Health Emergency, and which hospitals will face the biggest payment cuts. Moran is available to help with these and other payment modeling questions—and works on many of these issues in tandem with HMA’s Medicare experts.
For more information or questions about the policies described below, please contact our experts below.
This week our In Focus section reviews the Florida Statewide Medicaid Managed Care Program (SMMC) Invitation to Negotiate (ITN), released on April 11, 2023, by the Florida Agency for Health Care Administration (AHCA). SMMC consists of three programs: Managed Medical Assistance (MMA), Long-term Care (LTC), and dental, covering 4.4 million individuals. This ITN is for contracts to provide MMA and LTC.
Under the SMMC program, all enrollees receive their services from a single plan providing managed medical assistance, long-term care, and specialty benefits. (Dental benefits are provided separately.)
AHCA will select plans that will achieve the agency’s goals, including providing healthy birth outcomes for mothers and their infants, improving childhood and adolescent mental health, maximizing home and community-based placement and services, and supporting the HOPE Florida program. HOPE Florida utilizes ‘Hope Navigators’ to help individuals achieve economic self-sufficiency, develop long term-goals, and map out a strategic plan by focusing on community collaboration between the private sector, faith-based community, nonprofits and government entities.
Additionally, with the new contracts, AHCA will implement the following changes:
Specialty plans will no longer be awarded separately but must be awarded to a comprehensive or MMA plan.
Enrolling voluntary recipients (such as individuals with intellectual or developmental disabilities) into the SMMC program and providing the opportunity for them to opt out
AHCA may mandatorily enroll into the MMA program full benefit dual-eligibles who are also in a Medicare Dual Eligible Special Needs Plan (DSNP).
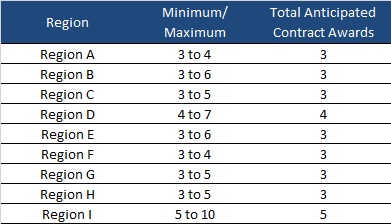
AHCA will invite 10 plans to negotiate for awards as shown below:
Timeline
Proposals are due August 15, 2023, with an anticipated award date of December 11. Contract will run from October 1, 2024, through December 31, 2030. Contracts may not be renewed, but AHCA may extend the term to cover any delays during the transition to a new plan.
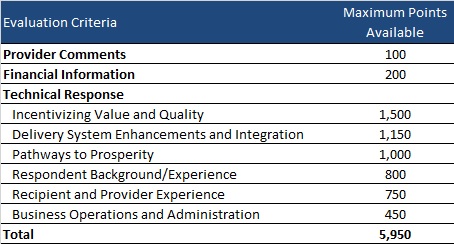
Evaluation
Plans can receive a total maximum number of points of 5,950. AHCA will invite top-ranking plans to negotiations to ensure that AHCA can enter into contracts with the minimum required number of plans per region.
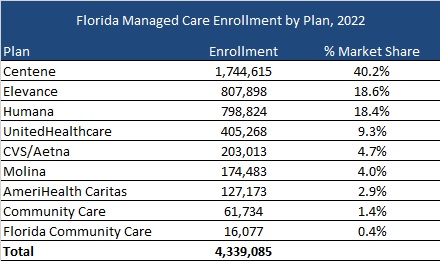
Current Market
As of December 2022, Florida served 4.3 million MMA and LTC enrollees, excluding an additional 97,000 Children’s Medical Services enrollees in the Children’s Medical Services Network plan. Centene had the highest market share based on enrollment, at over 40 percent.