HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
In the 2024 Political Checkpoint hosted by Leavitt Partners, an HMA company, we explored up-to-the-minute insights on the election results, discussed both confirmed outcomes and remaining uncertainties, along with the mandate for change that has emerged. Our expert panelists provided an overview of what to expect from Congress and the Administration, focusing on key legislative priorities and executive actions, and shared their prediction for what to watch over the first 100 days:
2024 Wrap Up Lame duck session in Congress, end of year regulatory action
A New President Implementing campaign promises through appointments
2025 Policy Agendas Where committees, agencies may set their sights
Key Issues Healthcare priorities that could see the spotlight
The sections below review results and share key takeaways. On November 12, during NAMD’s 2024 Fall Conference, KFF experts and state Medicaid directors will delve into survey findings on policies in place or planned for fiscal year (FY) 2024 and FY 2025, including state experiences with reduced state revenues and the unwinding of the pandemic-related continuous enrollment provision.
Several of HMA’s former Medicaid directors and Medicaid experts will be in attendance at the NAMD meeting to provide additional context and address questions about FY2025 Medicaid policies in the post-election landscape. Visit our Medicaid team at our exhibit hall booth, where we will have executive summaries on hand.
Medicaid Enrollment and Spending Growth
During the COVID-19 pandemic, Medicaid enrollment reached record highs as a result of the Families First Coronavirus Response Act, which authorized a 6.2 percentage point increase in the federal match rate, also known as the or Federal Medical Assistance Percentage until the public health emergency ended, provided that states did not disenroll people with Medicaid coverage. During this time, Medicaid and Children’s Health Insurance Program (CHIP) enrollment rose to 94 million in April 2023 from 71 million in February 2020. In FY 2024 and into FY 2025, states are concluding their Medicaid unwinding eligibility redeterminations.
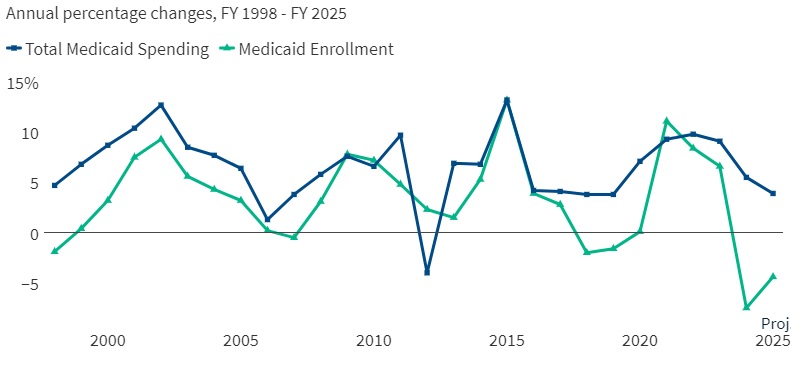
Medicaid enrollment declined by 7.5 percent year over year in FY 2024 and is expected to further decline by 4.4 percent in FY 2025. However, net Medicaid enrollment remained above pre-pandemic levels. Total Medicaid spending growth slowed to 5.5 percent in FY 2024 and is expected to slow further to 3.9 percent in FY 2025. State shares of spending, however, rose by 19.2 percent in FY 2024 and is estimated to slow to 7 percent in FY 2025. According to FY 2025 enacted budgets, most states anticipate revenue growth will continue to flatten and expect state general fund spending growth to slow. More than half of responding states anticipated a state revenue shortfall to some degree (see Figure 1).
Figure 1. Percent Change in Medicaid Spending and Enrollment, FY 1998−2025
Source: FY 2024−2025 spending data and FY 2025 enrollment data are derived from the annual KFF survey of state Medicaid officials conducted by HMA, October 2024. All 50 states submitted survey responses by October 2024; state response rates varied across questions. FY 2025 projections based on enacted budgets. Historic data reflects growth across all 50 states and DC and comes from various sources.
Managed Care and Provider Rates
Capitated managed care remains the predominant delivery system for Medicaid in most states. Specifically:
A total of 46 states operated some form of Medicaid managed care (managed care organizations [MCOs] and/or primary care case management [PCCM]).
42 states contracted with risk-based MCOs.
States use a variety of risk mitigation tools to ensure appropriate payment levels for MCOs, including risk-sharing arrangements, risk and acuity adjustments, medical loss ratios, or incentive and withhold arrangements (see Figure 2).
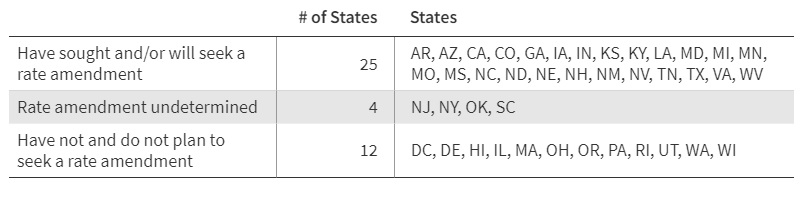
Of the 41 responding MCO states, 25 reported seeking approval from the Centers for Medicare & Medicaid Services (CMS) for a capitation rate amendment to address shifts in the average risk profile of MCO members in FY 2024 and/or FY 2025 because of the unwinding.
Separate from the KFF report, HMA tracks state Medicaid managed care rate certifications. In addition, Wakely, an HMA Company, published a paper summarizing approaches taken by actuaries in 27 states, and considerations for how they relate to the biggest enrollment shift in Medicaid since the implementation of the Affordable Care Act.
Figure 2. States Seeking Capitation Rate Amendments to Address Acuity Shifts Resulting from the Unwinding for the Rating Periods Beginning in FY 2024 and/or FY 2025
Source: Annual KFF survey of state Medicaid officials conducted by HMA, October 2024
States also are implementing a range of fee-for-service (FFS) rate increases across provider types. More than half of states reported increasing both inpatient and outpatient hospital FFS base rates in FY 2024. States reported rate increases for nursing facilities and home and community-based service providers more often than for other provider categories, reflecting ongoing staffing challenges for long-term services and supports (LTSS). Most states also reported rate increases for outpatient behavioral health providers, primary care professionals, and dentists.
Social Determinants of Health and Reducing Health Disparities
States are increasingly addressing social determinants of health (SDOH) and associated health-related social needs (HRSN) using several types of Medicaid authorities. For example:
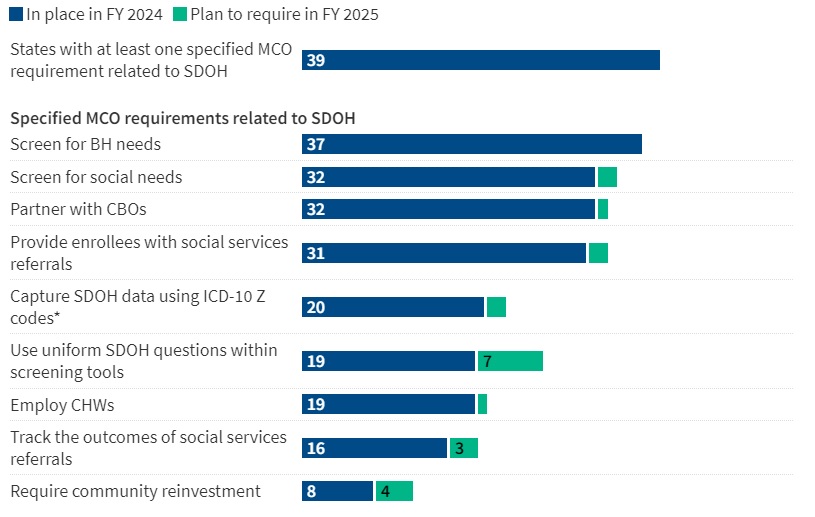
A total of 39 states reported leveraging Medicaid MCO contracts to promote at least one strategy to address SDOH, including screening enrollees for behavioral health or social needs, providing referrals to social services, partnering with community-based organizations, and requiring providers to capture SDOH data and employ community health workers. See Figure 3 for details.
Figure 3. MCO Contract Requirements Related to SDOH, FY 2024−25
Source: Annual KFF survey of state Medicaid officials conducted by HMA, October 2024
Nearly all states also had least one specified MCO requirement related to reducing racial and ethnic health disparities in FY 2025. About one-third of states reported at least one MCO financial incentive tied to reducing racial/ethnic disparities in place in FY 2024, most commonly linking capitation withholds or pay for performance incentives to improving health disparities.
Medicaid Section 1115 demonstrations are also being used to expand flexibilities by adding HRSN services and supports, including coverage of rent/temporary housing, utilities, and meal support. CMS has approved ten states under the new HRSN Section 1115 framework.
Benefits
In all, 41 states reported new or enhanced benefits in FY 2024, and 38 states reported plans to add or enhance benefits in FY 2025. Benefit enhancements continue to outpace benefit cuts.
States especially continue to expand behavioral health benefits, particularly for mental health and substance use disorder services.
A total of 11 states reported benefit actions related to the addition or expansion of crisis services, including mobile crisis responses and crisis services for youth.
Prescription Drugs
Rising prescription drug costs are an ongoing concern for states and nearly three-quarters of states reported at least one new or expanded initiative to contain prescription drug costs in FY 2024 or FY 2025.
Efforts to implement or expand value-based arrangements with pharmaceutical manufacturers were the most frequently mentioned cost-containment initiative across states.
Weight-loss prescription drugs also are a hot topic in the states; 13 states now cover GLP-1s (glucagon-like peptide-1s) prescribed to treat obesity. Most state Medicaid programs reported that cost was a key factor contributing to their decisions.
Key Opportunities, Challenges, and Priorities in FY 2025 and Beyond
Medicaid directors are focused on behavioral health, LTSS, and key initiatives related to SDOH or reentry services for justice-involved populations in FY 2025 and beyond. In addition, state-reported priorities included maternal and child health, rural initiatives, school-based services, continuous coverage for children, value-based payment and quality initiatives, and network monitoring and oversight.
Budget pressures and workforce shortages are among the main challenges for Medicaid. States noted adequate staffing and systems are obstacles for compliance with recently promulgated federal regulations, particularly the access and managed care rules, which present new reporting, oversight, and beneficiary protection responsibilities for states. Many states also reported a notable increase in per enrollee costs due to the greater healthcare needs of enrollees who retained coverage during the unwinding, adding pressure to budgets.
Connect with Us
The KFF Medicaid budget report provides important policy insights for federal and state government decisionmakers and Medicaid stakeholders. HMA’s Medicaid experts know the impact and planning needed to navigate these policies and to inform new decisions in 2025 and beyond. For more information about the key takeaways from the KFF report and HMA’s Medicaid solutions, contact our experts below.
This week, our In Focus section highlights the State of Nevada’s October 21, 2024 request for proposals (RFP), which will expand Medicaid managed care to cover nearly all populations in all counties. The Department of Health and Human Services’ Division of Health Care Financing and Policy (DHCFP) estimates that the expansion statewide will cover 75,000 additional individuals who live in rural areas, including children, parents, and adults without children. The expansion to rural areas in all counties presents new opportunities and critical issues for managed care plans, ensuring that they meet the needs of rural populations effectively.
Background
In 2024, Nevada covers 788,000 Medicaid members, with risk-based capitated Medicaid managed care making up about 75 percent of the total Medicaid population. Managed care covers traditional Medicaid and expansion, the Children’s Health Insurance Program (CHIP) known as Nevada Check Up, and children who have aged out of foster care. Enrollment in an MCO is mandatory for these populations. Currently, Medicaid managed care is only offered in the urban Washoe and Clark counties, which include cities such as Reno and Las Vegas.
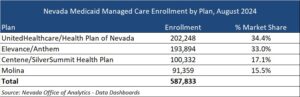
Nevada has four MCOs that were procured in 2021: Centene/SilverSummit HealthPlan, Elevance/Anthem, Molina, and UnitedHealthcare/Health Plan of Nevada. These MCOs serve approximately 588,000 beneficiaries in Urban Washoe and Urban Clark counties as of August 2024.
United and Elevance make up the majority of market share by enrollment, with 34.4 percent and 33 percent respectively.
Individuals who receive Medicaid through fee-for-service (FFS) are Medicaid-enrolled children in foster care, juvenile justice, and child welfare systems; individuals with disabilities; seniors; and individuals receiving services through one of the three 1915 home and community-based waiver programs. These individuals will continue to receive services through FFS.
RFP Highlights
The RFP describes the state’s three managed care service areas (SA): Urban Washoe, Urban Clark, and Rural. The Rural SA will include all other counties in Nevada in addition to the rural areas of Washoe and Clark counties.
MCOs must bid on all service areas. DHCFP anticipates selecting four plans. The two awarded vendors with the highest rural care score will operate in all three SAs. The remaining awarded vendors will operate in Urban Clark and Urban Washoe SAs. The state has the option to award a fifth contract to an MCO to operate in the Urban Clark SA only.
The RFP focuses on rural care and policies designed to improve outcomes and access to care, reduce burdens for providers to participate, and simplify administrative tasks for the state. MCOs will need to show their understanding of the unique challenges facing rural providers. They will describe their approach for provider outreach, contracting, and provider training strategies in rural areas, with a focus on primary care, maternal and child health, and behavioral health. Due to the geographic limitations, telehealth will also play a strong role. MCOs will need to address limitations such as access to internet and provide an approach to help members access telehealth. Additionally, MCOs will need to provide their experience in managing non-emergency medical transportation (NEMT) in rural areas and describe an approach for establishing and maintaining a network of transportation providers in these remote areas.
MCOs also will be required to offer at least one Silver and one Gold Qualified Health Plan (QHP) on Nevada Health Link Marketplace by the 2026 coverage year. The state expects this contractual requirement will help reduce churning and improve continuity of care for individuals and families who have a change in eligibility status.
MCOs must also contract with providers that use alternative payment methodologies (APMs), and plans will need to outline value-based purchasing (VBP) strategies within their proposals. APM contracting strategies must support priority areas such as addressing health-related social needs (HRSNs) and improving health equity, access, behavioral health, and maternal and child health outcomes. APM contracting strategies must include quality measures in the payment methodology and outline reporting and estimated financial details. Additionally, MCOs are required to develop a Population Health Program, so proposals must outline how it will leverage specific APMs to meet the program’s goals.
Evaluation
MCOs will require a minimum score of 945 points (out of 1,350 points) on the Technical Proposal to be eligible to win a contract. The Building Provider Networks and Access to Care technical questions is worth the most points, 450, while 300 points are available under the Rural Care and Service Area Expansion section. The table below provides a breakdown of the Technical Proposal Scoring.
The state assigns the highest number of points to the section addressing provider networks and access to care followed by the section addressing rural care and service area expansion.
Timeline
Key Considerations
HMA experts identified the key considerations for MCOs, partners to MCOs, providers who will furnish services to members, and other interested stakeholders.
The Building Provider Networks and Access to Care Rural Care and Service Area Expansion sections together are worth 750 points, most of the minimum needed, and more than half of the total available points. This is a strong indicator of that MCOs need to demonstrate capacity and innovation to ensure access to members using multiple strategies. Ensuring a robust network of healthcare providers in rural areas is crucial. This includes recruiting and retaining providers who are willing to serve in these regions.
In this RFP, DCHFP is evolving its value-based payment (VBP) initiatives and expectations for MCOs. The VBP strategies are intended to enhance care quality, improve patient outcomes, and ensure the sustainability of the Medicaid program. MCOs will need to design these models and successfully work with providers to implement the strategies and models.
Both improving maternal and child health outcomes and addressing mental health and substance use disorders are priorities for the state. These can be more challenging in rural settings due to limited access to specialized care and will require rural specific solutions.
Changing the Medicaid delivery system model in some rural areas may create the need for building awareness and understanding for the changes that come with this transition. MCOs should be prepared to effectively address the issues of equity and disparities that are present in in rural communities.
Connect with Us
HMA’s experts understand the Medicaid managed care environment and specific issues presented by rural areas. We work with clients to address the multilevel challenges for delivery of quality healthcare and social services to rural populations, and the workforce concerns they create. We identify and help plan for access issues such as lack of services, transportation difficulties, and socio-economic barriers. HMA knows the difficulties that often keep rural providers and organizations from achieving their full potential to serve and support their communities’ need and help Medicaid clients in rural areas in states around the country to solve these difficult problems.
Read more about the work we are engaged in with a range of healthcare industry leaders focused on rural and frontier areas.
The HMA Conference – Unlocking Solutions in Medicaid, Medicare, and Marketplace – was held in early October in Chicago, drawing a crowd of 350 participants hailing from all parts of the healthcare ecosystem. In the words of one attendee, what made the HMA conference unique was that “it was very rare to have providers, CBOs, health systems, insurers, and public sector organizations in one place…I gained significant value by viewing similar issues from different perspectives.”
Attendees participated in plenary sessions and breakouts that were grounded in Medicaid, Medicare, and Marketplace, with each session extending beyond the traditional topics for these public health insurance programs. Attendees were challenged and inspired to consider the cross-cutting work underway to address health equity, the integration of housing into healthcare, innovative strategies for behavioral health coverage for adults as well as children and families involved in the child welfare system, and the opportunities for federally qualified health clinics to engage in value-based care delivery to improve outcomes.
Signature HMA discussions with health plan leaders and Medicaid directors also provided valuable insights that will help guide the next phase of innovative programs and technologies designed and deployed to improve health. Breakout sessions offered in-depth exploration across Medicaid/Duals, Medicare/MA, and Marketplace/ACA tracks, alongside discussions on demand for innovation, advances in treating sickle cell disease, and creative workforce strategies. The conference concluded with a panel that prepared attendees for policymaking in the post-election, post-Chevron deference landscape.
The HMA event created opportunities to learn and network with potential partners against the background of the city of Chicago skyline, as one participant put it, “away from the daily craziness.” The discussions were robust and focused on new ideas that can be deployed by stakeholders all trying to improve the accessibility, quality, equity, and value of healthcare.
Listed below are conference takeaways that will be of interest and relevant to the broader healthcare ecosystem:
Systemize the little things that improve outcomes.
Keynote speaker Dr. Darshak Sanghavi from ARPA-H challenged people to focus on systematizing the “little things” that drive measurable improvements in outcomes as a source of meaningful innovation. His presentation focused on how ARPA-H is investing differently in private sector innovation – not just big breakthroughs, but also in data-informed approaches that produce consistent quality.
Housing is a healthcare issue.
There is increasing overlap between initiatives to address housing support in Medicare and Medicaid. Bridging diverse sectors and stakeholders is essential to address critical gaps in service delivery. HMA’s new Housing Services & Supports practice group recognizes that housing is part of healthcare, but it does not have to be fully funded by healthcare entities.
Cross-payer collaboration would improve behavioral health.
Behavioral health coverage has historically relied on the Medicaid-based chassis of coverage, but the breadth of needs and federal parity requirements have created an urgent need for new approaches to coverage across all systems and all payers. Cross-payer innovation and collaboration are essential, and systems need to position themselves to scale effective solutions that allow individuals to access services when they need them. In particular, youth and family voices must be part of the transformation of children’s mental health systems to smooth their experience.
The ACA is stable, but 2025 brings uncertainty.
The stability and future success of the ACA marketplaces hinge on the decisions of the 119th Congress regarding the extension of subsidies. If these subsidies are reduced or cancelled it could disrupt what has become a robust and reliable segment of the health insurance market, potentially requiring another pivotal transformation.
Community collaboration can bridge Medicaid health gaps.
New norms are emerging in the Medicaid program. There is unprecedented policy and programmatic work underway to ensure member experiences are informing the design of Medicaid programs as well as the type and pathways for accessing health and health adjacent services. Federal and state government, managed care plans, and providers must work together to bridge the gap to ensure Medicaid programs are best able to serve their members.
Interoperability remains foundational to quality improvement.
We have many different information systems, but when data is pushed to providers to help them manage their patient panel — ED visits, medications, and other data – higher quality care is more likely to be provided to patients.
Provider networks can be structured to ensure success in value.
Medicare providers are embracing value-based care on different timelines and in varied ways. Policymakers, health plans, and other stakeholders need to think carefully about how to structure networks with those providers who are doing it well to get the best results.
Clinics need help with data and financing to drive value-based outcomes.
Poverty is the primary diagnosis for patients of federally qualified health centers (FQHCs), and payment can better recognize the connections FQHCs make to anti-poverty services and programs. As the healthcare industry moves providers along the trajectory of value-based payment, FQHCs will be positioned to deliver whole person care if their data and financing is aligned.
These – and other takeaways and partnerships – will inform strategic, policy, programmatic and operational decisions at the hundreds of organizations represented at the HMA conference. They are also key points as we shape the conversations for the 2025 event.
Our second In Focus article reviews the recently proposed Notice of Benefit and Payment Parameters (NBPP) for 2026. The Centers for Medicare & Medicaid Services (CMS) proposed rule, released October 10, 2024, describes the policy and payment changes that will affect the Affordable Care Act (ACA) markets in 2026. Public comments must be submitted to CMS by November 12, 2024. Key highlights from the proposed rule follow.
Broker Oversight and Monitoring
CMS proposes to increase oversight and accountability for brokers and agents that write policies through HealthCare.gov. In response to the discovery earlier this year of fraudulent actors reassigning broker designations and switching consumer enrollments without their permission or knowledge, CMS has already implemented several corrective actions, including the suspension of 850 Healthcare.gov agents and brokers. CMS intends to build on these actions through the following interventions:
Clarify that lead agents, typically an agency owner or executive, are subject to the same rules as individual brokers, agents, and web-brokers and that enforcement action can be taken against the lead agents if they explicitly or implicitly condone misconduct or fraud
Broaden CMS’s authority to suspend broker and agent system access, inclusive of instances of suspected misconduct that affects eligibility determinations, operations, applicants, or systems
Update the model consent form to include documentation of the broker reviewing and confirming the accuracy of submitted application information with the consumer.
Marketplace User Fees
CMS proposes to increase the user fee collected to pay for administration of HealthCare.gov as follows:
Between 1.8 percent and 2.5 percent in 2026 for federally facilitated marketplaces (FFM) states, up from 1.5 percent of monthly premiums in 2025
Between 1.4 percent and 2 percent in 2026 for state-based marketplaces on the federal platform (SBM-FPs), up from 1.2 percent in 2025
The proposed changes are due, in part, to uncertainty caused by the future of the enhanced premium tax credits that are set to expire at the end of 2025. The enhanced premium tax credits are the driving force behind the increase in nationwide marketplace enrollment to more than 21 million people in 2020 from 11.4 million in 2020. If not extended, or if it takes past March 2025 for Congress to act, CMS has indicated the user fees will increase in 2026 to 2.5 percent for FFM states and 2% for SBM-FPs to accommodate expected enrollment declines. Notably, after several years of significant decreases, CMS is proposing to increase the user fees above 2025 levels regardless of the outcome of the enhanced premium tax credits.
Plan Limits for Non-Standard Plans
CMS proposes to clarify rules limiting the number of non-standardized plans an issuer can offer through HealthCare.gov (two or less in 2025). The limit is applied per product network type (e.g., HMO, PPO), per metal level, per service area, per inclusion of adult/pediatric dental and/or vision benefits (with additional exceptions, starting in payment year (PY) 2025, for plans with specific design features that would substantially benefit consumers and meet other requirements). To maximize the number of non-standardized plans offered on HealthCare.gov, an issuer could offer up to 16 plans per metal level and network type in a given service area by creating every combination of adult dental, pediatric dental, and adult vision (or even more, if plans meet the exception requirements).
Though CMS does not limit the number of standardized plan options an issuer offers on HealthCare.gov, they propose reinstating a meaningful difference standard to prevent consumer confusion and unnecessary plan proliferation. The proposed standard is similar to the removed standard from 2019; for plans in the same metal level, product type, and service area, a reasonable consumer needs to be able to identify at least one material difference in benefit coverage, provider networks, and/or formulary.
New Premium Payment Threshold Options for Issuers
CMS proposes new options for issuers to avoid triggering late payment grace periods for consumers who make most but not all of their premium payment to minimize termination of coverage for consumers who owe a small amount. The options include:
The current option of a “reasonable” percentage of net premium. CMS proposes codifying 95 percent as the minimum threshold.
New proposals of as low as 99 percent of gross premium and a fixed-dollar threshold of $5 or less.
CMS is also considering limiting issuers to offering just one payment threshold option—either fixed-dollar or percent of premium—to avoid consumer confusion.
Increased Transparency for State-Based Marketplaces
CMS proposes new initiatives to promote transparency into state-based marketplace (SBM) program operations. These initiatives include:
Publishing State Marketplace Annual Report Tool (SMART) submissions, which are used to monitor SBM compliance with select eligibility and enrollment, program integrity, and financial reporting requirements. SBMs must annually participate in independent programmatic and financial audits as part of SMART. CMS proposes to make the 2023 SMART submissions public in spring 2025.
Expanding the disclosure of SBM information to include data collected but not currently published, including details on SBM eligibility, enrollment, and plan certification policies as well as Navigator program spending, call center metrics, and website traffic data.
SBMs already are required to publish programmatic and financial audit summaries and generally publish robust data and information on their program operations through public reports and meetings; however, this information is neither centrally located nor consistently published across all SBMs.
Key Considerations
The proposed 2026 NBPP would build on previous actions that CMS has taken to address fraudulent broker and agent activity and to shore up financial sustainability of Healthcare.gov operations in light of uncertainty about the enhanced premium tax credits. It also seeks to make clear how plan variations adding dental or vision benefits factor into HealthCare.gov plan limits and gives issuers new premium payment threshold options. Lastly, it proposes new transparency requirements for SBMs. Interested stakeholders, including SBMs and issuers, should monitor how these proposed changes will affect consumers, operational processes, product strategy, and financial sustainability.
Connect With Us
The Health Management Associates, Inc., team has the depth, experience, and subject matter expertise to assist with tailored analysis and the modeling capabilities to assess the policy impacts to consumers, marketplaces, and issuers. If you have questions or want to discuss the proposed rule, contact our featured experts below.
This week, our In Focus section addresses the significant change in national and state-specific Medicaid enrollment as a result of the Medicaid unwinding process. First, we highlight notable enrollment changes in the post-unwinding months. Next, we provide an update on second quarter (Q2) 2024 monthly capitated, risk-based Medicaid managed care enrollment. The experiences of the unwinding and the impact and current enrollment landscape are directly affecting strategic and programmatic decisions across all states, Medicaid managed care plans, and their partners and stakeholders.
Background
As explained in previous In Focus articles (article #1, article #2 and article #3), federal COVID-19 relief laws allowed states to receive higher federal funding for Medicaid as long as they did not terminate Medicaid coverage for anyone enrolled in Medicaid during the public health emergency. One result of the continuous coverage policy was sustained growth in Medicaid enrollment. More than 21 million additional individuals were continuously enrolled in Medicaid for up to three years between February 2020 and March 2023. In December 2022, Congress ended the Medicaid continuous coverage policy after March 31, 2023. States were allowed to begin processing redeterminations as early as February 2023 and start disenrolling ineligible individuals as early as April 2023.
The Centers for Medicare & Medicaid Services (CMS) offered states a series of flexibilities intended to facilitate the unwinding process, which reduced some administrative burden and improved continuity of coverage for Medicaid enrollees. Most states adopted at least one of the flexibilities, with many using multiple options. Nonetheless, variations in timing and implementation of the flexibilities have affected their effectiveness.
California, for example, received federal approval for flexibilities in its automatic redetermination process early on but implemented enhanced automation months into its unwinding process. This increased automation cut the number of disenrollments in half. Another key challenge during the unwinding was contacting enrollees about the redetermination process, and several of the federal flexibilities involved increased coordination with Medicaid managed care organizations (MCOs).
Key Takeaways
States lost an average of 15 percent of their peak COVID-era Medicaid enrollment between March 2023 and June 2024. Several effective practices could be adopted to address those individuals and families who remain eligible but not enrolled and to minimize procedural disenrollments in the future. Below is a snapshot of data and early insights Health Management Associates, Inc. (HMA), experts identified through their work with Medicaid stakeholders and analysis of Medicaid enrollment and eligibility data.
Some states are several months beyond their anticipated unwinding period. Still, more than half of states continue to see small net reductions in their Medicaid populations (see Table 1).
Table 1. Enrollment Changes during and after Unwinding, September 2024
Despite the ongoing enrollment reductions, net Medicaid enrollment generally remains above pre-pandemic levels and is likely to remain so. This enrollment change has been boosted by several states—Idaho, Utah, Nebraska, Oklahoma, Missouri, South Dakota, and North Carolina—which expanded their Medicaid programs immediately before or during the COVID-19 pandemic.
Following the official end of the Medicaid unwinding period, the acuity of the Medicaid population increased significantly. Early actuarial assessments, including those conducted by HMA actuaries, indicate that the average Medicaid population is older and sicker than before the unwinding started. Consequently, Medicaid populations may be more complex and expensive to manage—prompting states and managed care plans to reassess their capitation rates for current and future years. The 24th annual Medicaid Budget Survey conducted by The Kaiser Family Foundation (KFF) and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD), also provides key take-aways on provider rates and managed care, among other issues in the report As Pandemic-Era Policies End, Medicaid Programs Focus on Enrollee Access and Reducing Health Disparities Amid Future Uncertainties: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2024 and 2025.
Medicaid Managed Care Enrollment Update – Q2 2024
Today, HMA Information Services (HMAIS) posted a quarterly update for Medicaid managed care enrollment. We collected and analyzed monthly Medicaid enrollment data from the second quarter (Q2) of 2024 (April−June) in capitated, risk-based managed care in 29 states. These data allow for the timely analysis of enrollment trends across states and MCOs as well as state and plan-specific analyses of managed care enrollment following the official end of the Medicaid unwinding period.1
The 29 states highlighted in this review have released monthly Medicaid managed care enrollment data via a public website or in response to HMA’s public records request. This report reflects the most recent data posted or obtained. HMA has made the following observations related to the enrollment data (see Table 2):
As of June 2024, Medicaid managed care enrollment across the 29 states tracked in this report was 62.7 million, down by 10.2 million (14 percent) year over year.
In our review, all but one state, Mississippi, saw decreases in enrollment in June 2024 because of Medicaid redeterminations.
The 22 expansion states included in the review—Arizona, California, Illinois, Indiana, Iowa, Kentucky, Louisiana, Maryland, Michigan, Minnesota, Missouri, Nevada, New Jersey, New Mexico, New York, North Carolina, Ohio, Oregon, Pennsylvania, Virginia, Washington, and West Virginia—have seen net Medicaid managed care enrollment decrease by 6.2 million (11.1 percent) in the past year, to 50.1 million members at the end of Q2 2024.
The seven states that had not expanded Medicaid as of June 2024—Florida, Georgia, Mississippi, South Carolina, Tennessee, Texas, and Wisconsin—have seen Medicaid managed care enrollment decrease 24 percent to 12.6 million members at the end of Q2 2024.
Table 2. Monthly MCO Enrollment by State, April−June 2024
Note: In Table 2 above, “+/- m/m” refers to the enrollment change from the previous month. “% y/y” refers to the percentage change in enrollment from the same month in the previous year.
It is important to note the limitations of the data presented. First, not all states report the data at the same time during the month. Some of these figures reflect beginning of the month totals, whereas others reflect an end of the month snapshot. Second, in some cases the data are comprehensive in that they cover all state-sponsored health programs that offer managed care options; in other cases, the data reflect only a subset of the broader managed Medicaid population. This limitation complicates comparison of the data described above with figures reported by publicly traded Medicaid MCOs. Hence, the data in Table 1 should be viewed as a sampling of enrollment trends across these states rather than a comprehensive comparison, which cannot be established based solely on publicly available monthly enrollment data.
Connect with Us
More detailed information on the Medicaid managed care landscape is available with a subscription to HMAIS, which collects and aggregates Medicaid enrollment data, health plan financials, and additional actionable information about eligibility expansions, demonstration and waiver initiatives, as well as population- and service-specific information, such as Medicare and Medicaid dually eligible beneficiaries, ABD populations, long-term services and supports, and patient-centered medical homes. HMAIS also includes a comprehensive public documents library containing Medicaid requests for proposals and responses, model contracts, scoring sheets, and protests.
For additional analysis of the Medicaid unwinding initiative and HMAIS’s enrollment data and subscription service, contact our featured experts below.
The 24th annual Medicaid Budget Survey conducted by The Kaiser Family Foundation (KFF) and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD), was released on October 23, 2024in the report As Pandemic-Era Policies End, Medicaid Programs Focus on Enrollee Access and Reducing Health Disparities Amid Future Uncertainties: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2024 and 2025.
At the end of state fiscal year (FY) 2024 and heading into FY 2025, states were wrapping up the unwinding of the pandemic-related continuous enrollment provision, focusing on an array of other priorities, and facing uncertainty about the stability of state revenues. States were also looking ahead to federal and state elections in November and the potential implications of those elections for Medicaid enrollees, states, and providers. As states have emerged from the now-expired COVID-19 Public Health Emergency, which profoundly affected Medicaid enrollment and spending, many are focused on using Medicaid to address long-standing health disparities (often exacerbated by the pandemic), improve access to behavioral health services and long-term services and supports (LTSS), address enrollee social determinants of health, and implement broader delivery system and value-based initiatives. The report includes key take-aways on provider rates and managed care, benefits and prescription drugs, and social determinants of health and reducing health disparities.
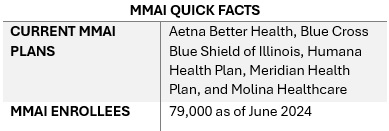
This week, our In Focus section from the HMA Weekly Roundup highlights the Illinois Department of Healthcare and Family Services request for proposals (RFP) for a dual-eligible special needs plan (D-SNP) to replace its current Medicare-Medicaid Alignment Initiative (MMAI) demonstration.
Overview
Illinois is one of the states affected by the Centers for Medicare & Medicaid Services (CMS) decision to end the capitated model in the federal Financial Alignment Initiative (FAI) demonstration. Illinois is among the last states to issue an RFP that will support the transition from the demonstration program. Two states, Texas and South Carolina, have yet to issue RFPs. On September 10, 2024, CMS issued a memo discussing end-of-demonstration enrollment and operational considerations and deadlines by which states should make operational decisions.
The Health Management Associates, Inc., (HMA) In Focus article June 26, 2024, discussed related changes that CMS finalized to the federal policy framework for D-SNPs to enhance care coordination, improve health outcomes, and ensure that dual-eligible beneficiaries receive accurate information about their healthcare while integrating successful features of the FAI demonstration and the Medicare-Medicaid Plan (MMP) program. These decisions are prompting more states to develop new models for integrating Medicare and Medicaid services.
Illinois D-SNP RFP Highlights
This Illinois procurement will transition the state to a fully integrated dual-eligible special needs plan (FIDE-SNP) model, which will include a requirement that plans provide managed long-term services and supports (MLTSS) for both people who are dually eligible and Medicaid-only beneficiaries beginning in 2027.
The RFP is largely focused on quality care provisions and improved care coordination across all services lines, including overall expectations to achieve the following:
Improved access and quality of community-based behavioral health services
Better quality of care in facilities
Fewer program opt-outs
A strategy for increasing the use of alternative payment models (APMs) in Medicaid managed care in Illinois, particularly for behavioral health providers
Emerging National Trends
Overall, the Illinois D-SNP procurement reflects broader national trends toward more coordinated, equitable, and outcome-focused healthcare.
Focus on Health Equity. The procurement emphasizes health equity and reducing disparities, including information on innovations that are responsive to health-related social needs (HRSNs) and social determinants of health (SDOH). The state is weighing payers’ experience partnering with non-traditional providers to meet Medicaid customers’ needs, their innovative programs to address customers who are difficult to locate, and their strategies for improving care for adults with complex needs in facility or community-based settings.
In addition, the state will require plans to report outcomes by race, ethnicity, and geography. Given the demographic and health equity reporting requirements, payers should be prepared to speak to their data collection, member engagement strategies, and relationships with community-based organizations. This capability will be an essential component of addressing both population health and health equity activities.
Alternative Payment Models. The RFP also requests detailed information on the payer’s strategy for increasing the use of APMs in Illinois Medicaid managed care, including the models the payer intends to implement. Experience supported by data-driven outcomes and explanations of work with providers or clinics to adopt, manage, and support reporting and analytics for APMs is a key area of interest for the state. Notably, the state seeks information on plans to include behavioral health providers in APMs.
Long-Term Services Related Transitions. The RFP questions also reflect the long-term services and supports that dually eligible beneficiaries need, as well as those of Medicaid-only beneficiaries who are eligible for these services. More specifically, the RFP raises questions to determine how payers will effectively implement nursing home diversion plans, incentivize hospitals to discharge patients to community settings, and approaches to transition members from institutional settings to the home and community, including by connecting members with supports for HRSNs. Payers will be expected to provide specific examples of their experience and outcomes in other states.
Emerging National Trends
The emphasis on health equity in the Illinois RFP reflects a broader national trend. States are increasingly interested in—and in some situations required—addressing SDOH and reduce disparities, especially for the Medicare and Medicaid dual-eligible population. As a result, payers and other healthcare organizations must develop capacity internally and through external collaborations to build their expertise and evidence base for advancing improvements.
The push for APMs in the Illinois procurement aligns with national efforts to move away from fee-for-service models. Illinois’s inclusion of behavioral health providers in APMs and requiring integrated care models highlights the growing recognition of the importance of mental health in overall health outcomes.
Illinois’s RFP also reflects heightened interest in improving care transitions and coordination. The potential for incentive programs related to community placement and increased focus on nursing home diversion will require innovative plans and a long-term commitment to working with all stakeholders to build on the federal FAI experiences.
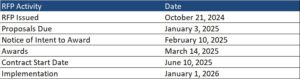
What We’re Watching
Responses to the Illinois RFP are due October 18, 2024, and awards are expected to be announced in December. The state anticipates making awards to the top four bidders. Contract execution is estimated July 2025, with implementation January 1, 2026.
As the FAI demonstration ends and CMS’s integration requirements take effect over the next several years, there will be a steep learning curve for states, payers, and other key stakeholders adapting to this evolving environment. Compliance with new CMS rules will be crucial, and experiences in Illinois and other FAI demonstration states can provide valuable insights for other states and stakeholders.
Additional growth and program refinements in the federal Medicare Advantage (MA) landscape are expected in the coming years, especially among MA D-SNPs. Those MA D-SNPs that have yet to participate in Medicaid will need to continue make significant business decisions on participation and actively compete to secure state Medicaid contracts, which will have downstream implications for their state and local partners.
Connect with Us
Health Management Associates (HMA) experts continue to review the evolving landscape and federal changes that will affect D-SNPs in 2025 and beyond. Contact our featured experts below for details about the nationwide D-SNP rules and landscape.
The upcoming HMA event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, offers extensive opportunities to engage with leaders from various sectors who are designing and implementing Medicare-Medicaid integration initiatives. Join us for main stage panel discussions with distinguished health plan executives from national and local plans and Medicaid directors from Iowa, New Mexico, New York, and Rhode Island.
HMA Principal Holly Michaels Fisher will lead a deeper dive into integration issues during the breakout session, Innovations to Improve Outcomes for Medicare-Medicaid Dually Eligible Individuals, with speakers Michael Carson, President and CEO of WellCare; Dr. Steven R. Counsell, Medical Director for the Division of Aging at Indiana Family and Social Services Administration; Dr. Linda Kurian, Executive Medical Director for the Center of Excellence of Medicare Duals/D-SNP at Aetna; and Juliet Marsala, Deputy Secretary for the Office of Long-term Living in the Pennsylvania Department of Human Services.
During the breakout, Meeting New Expectations for Health Equity and Improved Beneficiary Outcomes in Medicare Advantage, HMA Principal Greg Gierer will facilitate a conversation on the evolving landscape of MA rates and supplemental benefits, with experts Melinda Buntin, Health Economist and Bloomberg Distinguished Professor at the Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins Carey Business School; Mark Fendrick, Director of the University of Michigan’s Center for Value-Based Insurance Design, and Matt Kazan, Vice President of Policy and Government Affairs at the SCAN Group.
Caprice Knapp, a seasoned health economist with over 20 years of experience in Medicaid and healthcare policy, shares her journey through various roles in government, academia, and private insurance. In this episode, Caprice offers a unique perspective on the challenges of measuring quality in healthcare, the importance of data-driven decision-making, and how global healthcare models can inspire innovation in Medicaid. From pediatric palliative care to cost-effective policy solutions, Caprice sheds light on how improving quality of care can transform healthcare outcomes for vulnerable populations.
The report, released in August 2024 with support from Arnold Ventures, includes survey responses from 47 states (including DC) for state fiscal years (SFYs) 2023 and 2024. The survey instrument builds on questions posed in the 2019 Medicaid Pharmacy Study of all 50 states and the District of Columbia, which HMA and the Kaiser Family Foundation conducted.
The report discusses state trends for how Medicaid pharmacy benefits are administered across the country, including planned priorities and anticipated challenges in SFY 2025 and beyond. The findings are based on information provided by the nation’s state Medicaid Directors, Medicaid Pharmacy Directors, and other Medicaid agency experts.
Pharmacy Benefit Administration
In many states, managed care delivery systems play a pivotal role in administering Medicaid benefits, including prescription drugs. As of July 1, 2023, survey results found that:
A total of 33 states carved pharmacy benefits into managed care organization (MCO) contracts, with one state, Kentucky, directing its MCOs to use a single state-selected pharmacy benefit manager (PBM).
Eight states carve-out the pharmacy benefit—double the number in 2019.
MCO states were surveyed about their use of carve outs for certain drug products/classes, inclusive of physician-administered drugs covered under the medical benefit.
In all, 19 states reported carving out one or more drug classes or select agents within a drug class—often high-cost specialty drugs.
Of those states, 13 reported using the carve-out as part of a risk mitigation strategy.
Pharmacy Benefit Managers
The significant role and market power of PBMs have prompted many state legislatures to enact greater transparency practices and require health plans to accept more responsibility for monitoring the PBMs they contract with, which reflect notable changes since the 2019 survey. More specifically:
A total of 33 states reported contracting with a PBM.
The most frequently reported PBM functions included utilization management, drug utilization review, claims processing and/or payment, and rebate administration activities.
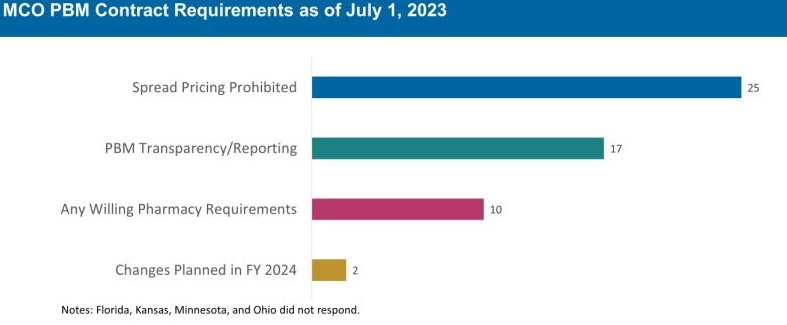
The 30 MCO states that carve in pharmacy benefits responded to survey questions about PBM transparency and spread pricing requirements. Of these states:
25 prohibit spread pricing in MCO PBM contracts—more than double the number of states reporting prohibitions on spread pricing in 2019.
17 reported having PBM transparency reporting requirements.
10 states reported having “any willing” pharmacy requirements.
The Role of PDLs, Prior Authorization, and Step Therapy in Controlling Drug Costs and Utilization
HMA’s experts also sought information on state payment strategies and utilization management protocols that are used to manage pharmacy expenditures. Nearly all responding states (44) have a preferred drug list (PDL) in place for fee-for-service prescriptions, which allow states to drive the use of lower cost drugs by encouraging providers to prescribe preferred drugs. Further, nearly two-thirds of responding MCO states (19 of 30 states) that do not carve out the pharmacy benefit reported having a uniform PDL for some or all drug classes, requiring all MCOs to cover the same drugs.
Many states have implemented step therapy and prior authorization (PA) guardrails in their Medicaid programs through legislation. However, 85.1 percent of responding states (40 of 47) report utilization controls like PA or step therapy applied to drugs that are reimbursed through the medical benefit to control utilization and costs. States also play an active role in managing MCO clinical protocols or medical necessity criteria, with 22 out of 30 MCO pharmacy carve-in states reporting that they require uniform clinical protocols for some or all drugs with clinical criteria. Approximately one-half of responding MCO carve-in states also require review and approval of MCOs’ PA criteria (15 of 30 states) and step therapy criteria (14 of 30 states).
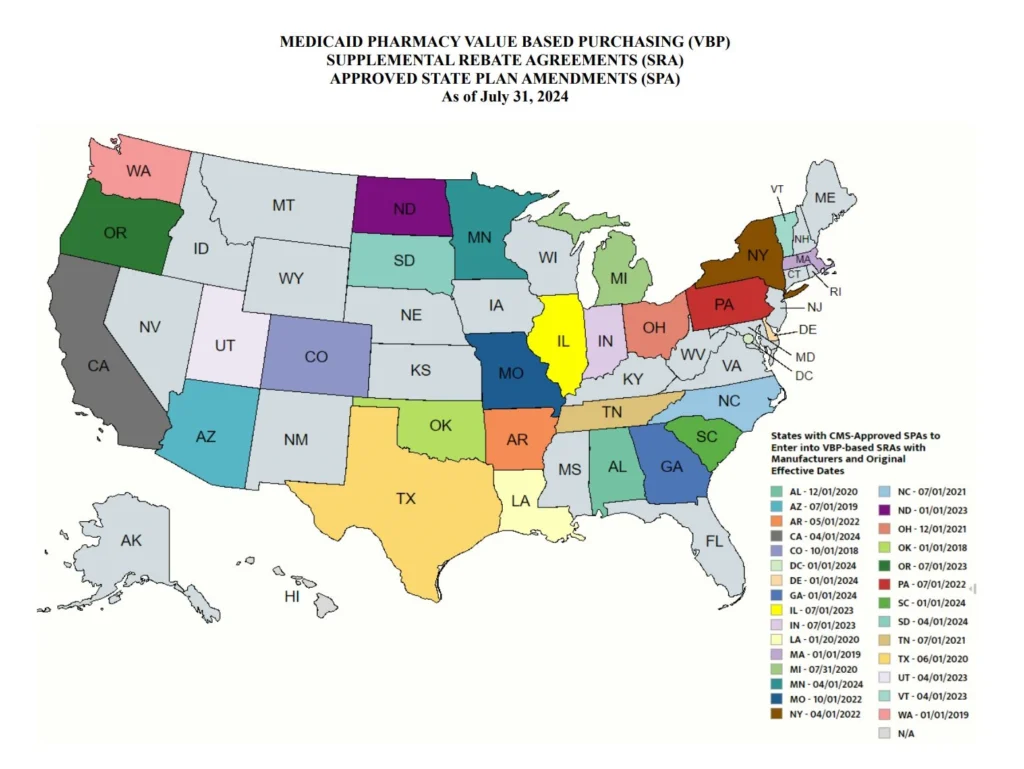
State Adoption of VBAs: Improving Patient Access to Cell and Gene Therapies
A growing number of states are actively considering entering into value-based arrangements (VBAs) with manufacturers, as pressure to improve patient access to cell and gene therapies increases. Nine states have at least one VBA in place, and 23 states reported that VBAs are among their future solutions for addressing coverage of new high-cost therapies. States will need to address common barriers to VBA implementation, which involves more upfront costs and operational challenges to implement than traditional contracts.
Subsequent to the submission of survey responses, the Centers for Medicare & Medicaid Services (CMS) released a Cell and Gene Therapy (CGT) Access Model, which begins with a focus on sickle cell disease, anticipated to go live on January 1, 2025. Under the model, CMS will negotiate outcomes-based agreements with manufacturers on behalf of the state to ensure that treatment pricing is related to treatment effectiveness. In the coming years, experiences with this model will help determine whether a CMS-led approach to developing and administering VBAs for CGTs improves Medicaid member access to innovative treatment and their impact on expenditures, if any.
Managing the Medicaid pharmacy benefit has never been more challenging. In FY 2025 and beyond, most states will be focused on managing their Medicaid pharmacy budgets, especially the development of VBAs and other policies and strategies for managing new high-cost therapies. Other top priorities and challenges cited by multiple states include management of PBM arrangements and considering coverage of the new generation of GLP-1 anti-obesity medications. States also must react to changing drug marketplace conditions driven, in part, by federal policy changes to the Medicaid drug rebate formula and changes designed to lower Medicare drug costs. Drug manufacturer responses to these changes have implications for Medicaid state budgets, but also for state PDL management decisions and beneficiary access to needed medications.
Connect with Us
The upcoming event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, hosted by HMA, will offer more opportunities to engage with report author Kathy Gifford at the pre-conference workshop Paying for Innovative Pharmaceuticals: State and Federal Trends Shaping Public Programs. Leaders from various sectors will join Kathy to discuss trends in prescription drug policies in public and commercial insurance programs.
For details about the report, contact our featured experts below.
This week, our In Focus section reviews state policies designed to increase insurer participation in Medicaid managed care and Marketplace programs. As states seek to address healthcare costs, affordability, and consumer experiences, they are exploring a range of initiatives—from the rise of prescription drug affordability boards to cost containment commissions, cost growth benchmarks, transparency, and examination of mergers and acquisitions.
A notable trend is the use of state policy and purchasing power to encourage or mandate that Medicaid managed care organizations (MCOs) offer Marketplace plans. Dual-market participation can help smooth coverage transitions, ensure continuity of care, and expand consumer choice. The remainder of this article addresses original research and analysis of this trend by our Health Management Associates, Inc. (HMA), featured experts.
Current Landscape
In 2024, enrollment in the Marketplace program has surged to more than 21 million, approximately a 30 percent increase from 2023. This growth was largely attributed to the temporary enhanced subsidies that allowed more people to access affordable coverage. Over the past several regulatory cycles, federal policymakers also have taken steps to further align the Marketplace framework with Medicaid on key issues, such as essential community provider access, eligibility and enrollment processes, and plan design standards. In response, states are innovating to meet federal requirements while pursuing their own healthcare goals related to coverage, affordability, access, and healthcare outcomes.
Value Proposition
A compelling value proposition for Medicaid MCOs to participate in the Marketplace (and vice versa) includes the ability to market to and retain people moving from one program to another as life circumstances change. Dual-market participation also supports diversification and growth strategies. In fact, enrollment in the Marketplace has nearly doubled since 2020. For Medicaid MCOs in particular, expanding product offerings to include Marketplace plans presents a unique opportunity to leverage existing provider networks and reimbursement arrangements to deliver more competitive rates.
Consumers benefit when the same organization participates in both markets. Families with parents and children who obtain coverage under different programs have an opportunity to work with a single organization and choose providers from the same or overlapping networks. Income fluctuations may result in disenrollment from one program (e.g., Medicaid) and eligibility for a new program (e.g., Marketplace subsidies). Continuity of care policies can smooth these transitions in areas such as prior authorization, care management, and provider network.
State Strategies to Increase Dual-Market Participation
The Affordable Care Act expanded access to affordable health insurance coverage for as many as 45 million individuals by giving states the option to expand Medicaid and provide federal subsidies to people who purchase Marketplace plans. States are now using various strategies to encourage or require insurer participation in both programs to ease transitions for individuals and families “churning” from one program to another, increase competition and choice of Marketplace plans, and reduce the risk of coverage gaps. For example:
Nevada is requiring any bidder that plans to respond to its upcoming Medicaid MCO procurement to separately submit a “good faith” response to the Battle Born State Plans (BBSP) RFP. This state-contracted, public option will be available on the Silver State Health Insurance Exchange beginning in 2026. Failure to submit a good faith proposal will disqualify an organization from participating in the Medicaid MCO procurement later this fall. Nevada’s current Medicaid MCOs must participate in the Marketplace by offering at least one Silver and one Gold qualified health plan (QHP) that has overlapping provider networks, serves the same service area, and charges reasonable premiums.
Rhode Island and New Mexico require or intend to require that their Medicaid MCOs participate in the Marketplace. As an awardee of Rhode Island’s recent Medicaid MCO procurement, UnitedHealthcare, must reenter the HealthSource Rhode Island market in 2027. These states also have designed their Medicaid MCO auto-assignment methodology to favor enrollment in a Medicaid MCO affiliated with an individual’s previous Marketplace plan or a family member’s Marketplace plan.
In its last Medicaid MCO procurement (2018), North Carolina offered bonus points to any bidder that agrees to offer a Marketplace MCO. The resulting contract codified the market entry commitment and included implications for failure to follow through. Nonfulfillment could result in the highest level of contract noncompliance and associated penalties.
Arkansas expanded its Medicaid program using federal matching funds to purchase QHP coverage through the Marketplace. Minnesota, one of the few states offering a basic health program, contracts with the same organizations to provide coverage under both programs.
Iowa uses contract language to encourage, but not require, Medicaid MCOs to participate in the Marketplace to facilitate continuity of care during coverage transitions.
The Centers for Medicaid & Medicare Services (CMS) collaborated with states to promote continuity of coverage following the end of the Medicaid continuous enrollment requirement established in the Families First Coronavirus Response Act of 2020, also known as the Medicaid public health emergency (PHE) unwinding. This support includes the clarification of permissible outreach activities by Medicaid MCOs that also offer a Marketplace plan, information sharing, and other assistance. Many states have incorporated the CMS guidanceiii into Medicaid MCO contracts. North Carolina, Utah, and West Virginia include additional contract terms supporting their Medicaid MCOs’ ability to co-market Medicaid and Marketplace plans, including when an individual is losing Medicaid eligibility.
What to Watch For
Coverage transition challenges throughout the Medicaid PHE unwinding have highlighted the real-life impact of coverage gaps and the importance of policies and practices that promote uninterrupted access to healthcare coverage. Historic Marketplace enrollment levels and recent CMS guidance clarifying the allowability of outreach to people who are losing Medicaid coverage about Marketplace plan available make the prospect of dual-market participation increasingly attractive for Medicaid MCOs. A greater focus on improving continuity of care and Marketplace plan choice may lead to more states encouraging or requiring Medicaid MCOs to participate in the Marketplace.
Connect with Us
The upcoming HMA event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, will offer more opportunities to engage with leaders from various sectors who are advancing innovations in Medicaid managed care and Marketplace programs and the points at which these programs intersect. State Medicaid and insurance commissioners, health plan executives, and community leaders, among others, will share insights into their market success and initiatives designed to address healthcare costs and insurance affordability.
Experts from HMA and our family of companies have extensive experience in the policy, structure, and administration of healthcare markets and health plan contracting. For more information, contact our featured experts below.