1300 Results found.

What Strategies Help Local Governments Stay Resilient Amid Health Policy Changes?
John Eller, managing principal at Health Management Associates, joins Vital Viewpoints on Healthcare to discuss the critical role of resilience in local health services. As communities navigate shifting federal policies, economic uncertainty, and natural disasters, John shares insights on how agencies can remain nimble, collaborative, and innovative. Drawing from his extensive experience in Medicaid transformation, behavioral health, and social services leadership, he highlights the power of community trust and cross-sector partnerships in maintaining stability during turbulent times.

New Insights on Medicaid Spending: An Analysis of Disaggregated Managed Care Spending
Medicaid is a federal/state health insurance program that served more than 86 million lower-income people in fiscal year (FY) 2021. The combined federal and state spending for Medicaid totaled $717 billion that year, $420 billion of which was spent on providing care to Medicaid managed care organization (MCO) members, and $297 billion on services provided to fee-for-service enrollees.
- While the role of managed care in Medicaid has grown tremendously over the past decade, with MCOs covering nearly three-quarters of Medicaid enrollees, detailed cost information has not been estimated for the people with MCO coverage. These data historically have been available only for fee-for-service (FFS) Medicaid because of limitations on federal data sources.
- This lack of data blocks our understanding of the relative magnitude of the cost drivers in the program and contributes to an uninformed debate about policy reforms to control the growth of spending and improve quality of care.
- Obtaining and using cost data by provider type for MCOs can help answer questions such as how much funding do MCO enrollees with diabetes, asthma, and/or hypertension consume? Of these patients, how many also have behavioral health conditions? How many MCO enrollees have six or more emergency department (ED) visits during a year and/or multiple inpatient hospital stays, and what does their resource consumption look like?
Health Management Associates (HMA) has developed a reliable methodology that can be applied to all 50 states, which approximates spending for the major categories of health services that MCOs cover, including: inpatient and outpatient hospital care, physician and other professional services, skilled nursing facilities, clinics, pharmaceuticals, and other services. HMA can determine prices for these services, which, combined with data on the number of encounters, yields reliable cost figures. These cost estimates will be useful in identifying unmet medical needs, gaps in our delivery systems, and areas of high spending where efficiencies and timely care management can be added to slow the growth in total health spending.

Navigating CMS’s 2025 Marketplace Rule: What It Means for ACA Marketplaces, Insurers, and Consumers
This week, our In Focus section also reviews the 2025 Marketplace Integrity and Affordability Proposed Rule, released by the Centers for Medicare & Medicaid Services (CMS) on March 10, 2025. The proposed rule calls for enhancing program integrity protections in the Affordable Care Act (ACA) marketplaces through targeted changes to eligibility and enrollment policies and procedures.
This proposed rule aligns with the overarching policy priorities President Trump has identified, including reducing federal costs and reforming policies related to immigrants. It also takes aim at fraud, waste, and abuse practices in the ACA Marketplaces, which is the cornerstone from which the US Department of Health and Human Services explains and justifies its proposed initiatives.
Notably, the proposed changes will occur alongside other potential federal policy revisions, including the December 31, 2025, expiration of the ACA enhanced subsides for consumers, which led to historically high coverage levels—nearly 24 million people were enrolled in the Marketplace as of January 2025. The combined changes will have a varied but significant effect on all state health insurance markets, creating a need for scenario planning and preparation to start immediately.
CMS is providing the public 30 days to submit comments on the proposed rule. An overview of the proposed changes and key considerations follow.
Rule Components
Enrollment Timeline: CMS proposes shortening the open enrollment period for all individual market coverage, including for state-based marketplaces (SBMs), which traditionally have had flexibility to set later enrollment deadlines. If finalized, open enrollment will begin November 1 and end December 15, a month earlier than the current deadline of the following January 15.
Income Verification: The rule would require marketplaces to bolster their income verification processes to protect against manipulation of the authorization and calculation of advance premium tax credit (APTC) values. CMS policymakers believe these changes will be useful in addressing broker and consumer fraud and abuse of the APTC eligibility process. Proposed income verification changes include requirements that people provide the documentation of their income if they meet the following criteria:
- The income on their application is between 100 percent and 400 percent of the federal poverty level (FPL), but the income returned from external data sources show they make less than 100 percent of the FPL
- No tax data are available from external data sources to confirm the applicant’s self-attested income
Applicants who do not verify their income will have it adjusted to align with the income returned from external data sources, and their APTC eligibility will be updated accordingly. In some cases, such as when no returned income data are available, these individuals will become ineligible for the APTC.
CMS also plans to reinstate a 2015 policy that requires marketplaces to designate applicants or enrollees as ineligible for APTCs if they fail to file and reconcile their APTC on their federal income taxes. This requirement is known as the failure to file and reconcile (FTR). The Biden Administration changed the FTR requirements to find enrollees ineligible for APTCs if they fail to file and reconcile for two consecutive tax years.
Lastly, CMS proposes eliminating the additional 60 days consumers are granted to resolve income inconsistencies. Today, most marketplace consumers have up to 150 days to resolve income inconsistences. This proposal would return to the 90-day verification period that was in place prior to the Biden Administration.
CMS also requests input on alternative redetermination and re-enrollment policies for fully subsidized consumers, including whether $5 is the appropriate premium amount or should be higher or if fully subsidized consumers should be required to actively confirm their eligibility and reenroll every year.
Another proposal would remove the ability for marketplaces to automatically reenroll Bronze members who are eligible for a cost-sharing reduction (CSR) in a Silver plan if the Silver plan has the same provider network, is in the same product, and has a lower or equivalent net premium as the consumer’s Bronze plan.
Special Enrollment Period Changes: CMS is proposing multiple changes to special enrollment periods (SEPs), including the removal of monthly SEPs for individuals with household incomes that are projected to be at or below 150 percent of the FPL and a requirement that marketplaces verify eligibility for at least 75 percent of new enrollments during SEPs. CMS also proposes adopting a pre-enrollment income verification model for SEPs.
- Bar Deferred Action for Childhood Arrivals (DACA) recipients from QHPs in the Marketplace and basic health programs, making them ineligible for APTCs and CSRs and returning to pre-Biden era DACA eligibility rules
- Remove gender-affirming care as an essential health benefit
- Allow insurers to require payment of past due premiums before effectuating new coverage, if state law permits
- Increase cost sharing/lower premiums by increasing the maximum out-of-pocket limit and widening de minimis ranges
Implications
CMS is reverting to several policies that were put in place during President Trump’s first term, increasing the likelihood that CMS will finalize many of the changes as proposed or with minimal modification.
Insurers, SBMs, insurance departments and other stakeholders should engage in the federal policymaking process and begin planning immediately for the financial and operational changes that will be required to comply, as several of the requirements will take effect as soon as the rule is finalized. Stakeholders will also want to consider the direct impact on consumers.
Health Management Associates (HMA) Marketplace experts identified the six key considerations for stakeholders:
- Market share and risk. The proposed changes are projected to decrease Marketplace enrollment and Insurers and states need to plan for shifts in their market and consider approaches to manage these changes.
- Administrative operations. A shorter enrollment period and additional eligibility and enrollment requirements may increase administrative actions for enrollees, insurers, and marketplaces. Examples include:
- Marketplaces will need to make system and operational changes to comply with the new income verification, SEP, and open enrollment period requirements.
- Departments of Insurance may need to adjust their rate and form filing instructions and timelines to give insurers the clarity and time they need to comply with new requirements.
- Consumer education. Insurers and marketplaces will need to consider the effectiveness of their marketing and outreach and education strategies, given the shorter open enrollment period.
- Interactions with the expiration of the enhanced subsidies in 2026. The Congressional Budget Office estimates that the uninsured population will increase by 2.2 million in 2026 and up to 3.8 million by 2028 if the enhanced ACA subsidies expire. While it is too early to project or measure the impact of this proposed rule and the expiring subsidies, together they undoubtedly will have direct impacts on eligibility, enrollment levels, market dynamics including pricing and risk mix, and the overall stability of the Marketplaces in the long term. Congress may also take action on other policies related to Marketplace stability for which stakeholders should prepare.
- State-level mitigation. States interested in mitigating the impacts of this proposed rule, as well as the expiring subsidies, will need to consider legislation to address the resulting affordability gaps and coverage losses. For example, states may look to state-funded subsidy wraps or reinsurance programs to minimize the net premium rate increases that most Marketplace plan members will experience when the enhanced subsidies expire in 2026.
- Federal engagement. CMS is providing the public 30 days to comment on the proposed rule. This provides stakeholders the opportunity to voice their positions on the impact of this and future Marketplace policies. Comments on the proposed rule may also be shared with congressional policymakers and staff to help shape future legislative proposals.
HMA experts have considerable experience working with marketplaces, Departments of Insurance, insurers, and federal policymakers with jurisdiction over the Marketplace. They work with these entities to inform, analyze, and influence federal policies and conduct impact analyses on pricing, enrollment, administration, and operations. HMA also provides strategic and project management support for the implementation of finalized policies.
To learn more about how the proposed rule and the scheduled sunsetting of enhanced subsidies may affect your organization contact HMA Marketplace experts below.
New Insights on Medicaid Spending: HMA Analysis of Disaggregated Medicaid Managed Care Spending
This week, our In Focus section highlights insights from a new Health Management Associates (HMA), issue brief, “New Insights on Medicaid Spending: An Analysis of Disaggregated Managed Care Spending.” Until now, most Medicaid cost data have focused on enrollees in fee-for-service (FFS) programs. HMA used the Centers for Medicare & Medicaid Services (CMS) Transformed Medicaid Statistical Information System (T-MSIS) database to analyze Medicaid managed care organization (MCO) spending in major categories of healthcare, including inpatient and outpatient hospital care, physician and other professional services, skilled nursing facilities (SNFs) and home and community-based services (HCBS), clinics, pharmaceuticals, and other services. HMA’s methodology can be applied to all 50 states and allows us to determine prices for these services, which, combined with data on the number of encounters, yields reliable cost figures.
Findings
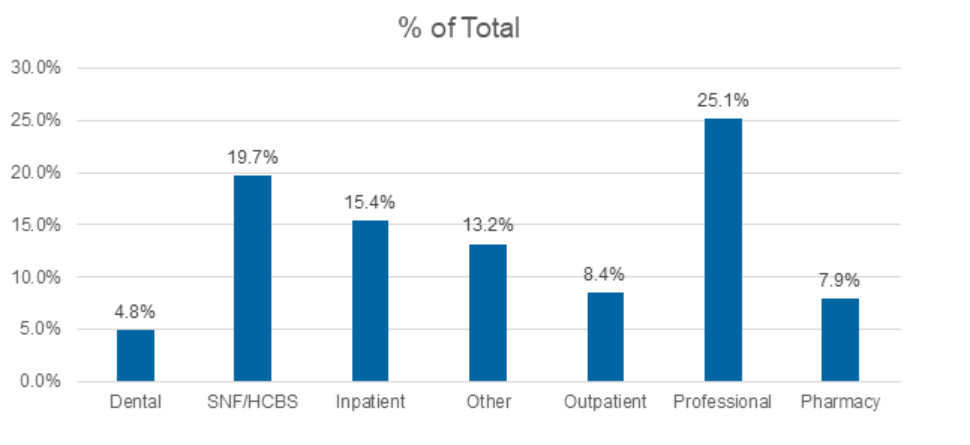
Medicaid managed care accounted for $420 billion of the total $717 billion in Medicaid spending for federal fiscal year 2021. Professional claims accounted for the largest portion of Medicaid spending, totaling 25.1 percent, followed by SNFs at 19.7 percent, and inpatient claims at 15.4 percent.
Figure 1. T-MSIS Medicaid Spending by Service Category 2021 (MCO Disaggregated plus FFS)
What’s Next
This analysis can be replicated for subsequent years and will provide important information on Medicaid spending trends. This work also sets the stage for analyses and comparisons of cost categories by variables such as eligibility category (e.g., dual eligibles, children, parents, adults without children, the Medicaid expansion population, and designated as aged/frail/disabled); race and ethnicity; frequent users of hospital services; and people with multiple chronic illnesses. This type of analysis allows us to answer fundamental questions about the Medicaid program and can pinpoint areas of high need within the Medicaid population, such as:
- How much do we spend on services for people with diabetes?
- How much do we spend during childbirth/first year of life and in the last year of life?
- How much do we spend for Medicare-Medicaid dual eligibles?
Data-informed discussions on these and other topics can help identify opportunities for efficiencies and timely care management to slow the growth in total healthcare spending. This information will provide important context for the policy debate, offering a full view of the relative magnitude of the major categories of Medicaid spending.
Connect with Us
Medicaid providers, MCOs, states, and policymakers all have an interest in identifying high-cost drivers of Medicaid managed care. The methodology applied in the analysis for the HMA issue brief can be applied and adapted for future analysis.
For details about this analysis, its implications for state and local policies, and additional research using T-MSIS, contact our experts below.

March 19, 2025
New Insights on Medicaid Spending: HMA Analysis of Disaggregated Medicaid Managed Care Spending
Join the Call to Action to Address the Behavioral Health Workforce Crisis
The behavioral health workforce crisis, a long-standing issue worsened by the COVID-19 pandemic, threatens the ability of provider organizations to meet growing demands for behavioral health treatment services. Despite decades of efforts, challenges such as inadequate compensation, workforce shortages, lack of diversity, and high burnout persist. In fact, a 2023 survey of state Medicaid officials on behavioral health revealed that nearly every state was engaged in at least one strategy to address the workforce shortage.[1]
Since 2021, The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked to create both short and long-term solutions. Efforts have included:
- Policy papers aimed at short term solutions
- Review and crosswalk of over 400 recommendations from organizations across the country
- Creation of the Workforce Solutions JAM, begun in May 2024, a monthly webinar spreading innovation and discussing all elements of the behavioral health workforce
- Multiple convenings of technical experts and partners to discuss how to support action on the workforce
- And now a call to action.
The next step for the Workforce Solutions Partnership is to expand engagement with partners to address the workforce shortage. The Partnership believes that using the Collective Impact framework, will provide the structure to build a national strategy and cross-sector approach to shared implementation of workforce initiatives, resulting in effective and scalable solutions. We understand there are countless workforce initiatives underway across the country, many of which are demonstrating progress and innovations that can be scaled. Rather than duplicate or distract from existing efforts, the Partnership will build connections between these efforts, elevate their impact and empower emerging innovative ideas.
Initial areas of focus will include:
Community alignment: Enhancing recruitment and retention of a workforce that reflects the communities accessing behavioral health services.
Creation of efficiencies: Building a new operational and administrative model that improves access.
Technology integration: Exploring tech-enabled supports to enhance skill development and service delivery.
Career pathways and compensation: Improving access to career opportunities and using evolving payment models to increase salaries for behavioral health professionals.
The Call to Action outlines the Partnership common agenda, levers of change, and the process for developing a national platform for change. It outlines how partners can engage and is the launch of what we hope will be national action to build a sustainable workforce.
[1] Saunders, H., Guth, M., & Eckart, G. (2023). A look at strategies to address behavioral health workforce shortages: Findings from a survey of state Medicaid programs. Kaiser Family Foundation. https://www.kff.org/mental-health/issue-brief/a-look-at-strategies-to-address-behavioral-health-workforce-shortages-findings-from-a-survey-of-state-medicaid-programs/
Workforce Solutions Partnerships: Call to Action to Build a Sustainable Behavioral Health Workforce
The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked since 2021 to create both short and long-term solutions addressing the behavioral health workforce crisis. In this whitepaper, we issue a Call to Action to partners across all sectors to join us in this effort to drive pervasive change and ensure the future of behavioral health care. We need you to help us create and define the future of the workforce and envision a new system of care. This paper outlines the problem and highlights the efforts developed by our partnership, and mechanisms that can help to address the problem.

The Medicaid Pivot: New Developments in Section 1115 Demonstration Policy
This week, our In Focus section examines new federal policy developments affecting Medicaid Section 1115 demonstrations. The Centers for Medicare & Medicaid Services (CMS), on March 4, 2025, rescinded two guidance letters issued by the prior Presidential Administration that defined and provided the framework for state Medicaid programs to cover health-related social needs (HRSNs) using Section 1115 authority.
Though specific Medicaid priorities under the Trump Administration are nascent, Health Management Associates’ federal and state experts are monitoring these developments. This article describes the withdrawn policy, known implications for states with approved and pending proposals, and the imperative to plan for a variety of scenarios and future opportunities.
Background on HRSN Initiative in Section 1115 Demonstrations
CMS-approved Section 1115 demonstrations allow states to pilot alternative methods to improve the accessibility, coverage, financing, and delivery of healthcare services under joint federal-state funded programs, specifically Medicaid and the Children’s Health Insurance Program (CHIP).
Addressing health disparities and promoting integrated care in Medicaid became a key focus of the Biden Administration. In November 2023, CMS introduced a Medicaid and CHIP Health-Related Social Needs Framework, giving state Medicaid agencies the opportunity to address the broader social determinants of health (SDOH) that affect their enrollees, leading to better health outcomes. The agency published an update to the guidance in December 2024. The new initiatives were not intended to replace other federal, state, and local social service programs, but rather to coordinate with those efforts.
Key Takeaways for States
The following critical components of the March 2025 announcement and the present policy landscape should inform state Medicaid agency and stakeholder response and future planning work.
First, this guidance does not affect states with a current, active Section 1115 demonstration, state plan, or 1915 waiver programs that include HRSN. States with HRSN demonstrations will maintain their approved programs; however, states and their partners should prepare for shifts in federal reporting, oversight, and evaluation expectations. Separately, states may wish to re-evaluate their resource allocation and consider adjustments that may be needed to better align with a new federal policy environment.
States seeking any amendment or extension of their demonstration program—even if unrelated to HRSN—should expect this activity to trigger a CMS review of the HRSN component of the 1115. States will need to consider the strategic advantages and necessity of such requests relative to the implications to their HRSN initiative. They also should consider planning for nonrenewal of their HRSN programs in advance of the demonstration’s current expiration date.
Pending state HRSN Section 1115 demonstration proposals are not expected to be approved. The Section 1115 option for federal matching funds to provide up to six months of housing supports, nutrition supports, and associated infrastructure capacity funding no longer aligns with the Trump Administration’s objectives for Medicaid and CHIP. Stakeholders interested in these concepts should consider alternative strategies and investment options.
What to Watch
Notably, CMS did not rescind the 2021 State Health Official Letter RE: Opportunities in Medicaid and CHIP to Address Social Determinants of Health (SDOH) (SHO# 21-001) published during the first Trump Administration. States and their partners should monitor CMS’s actions and signals for the agency’s posture toward SDOH proposals.
A new group of states proposing alternative and revised demonstration concepts and innovations is likely to emerge. These states may provide early signals of the nature and breadth of the Section 1115 demonstrations CMS is willing to consider. With regard to SDOH, states and their partners should consider aligning proposals with the approaches outlined in the 2021 guidance for regular federal program authorities (e.g., 1915(i) state plan options, 1915(c) waiver options) as well as certain managed care authorities.
In addition, states and Medicaid stakeholders should watch for other Medicaid and CHIP policy priorities advanced through demonstration and other authorities, including efforts to address substance use disorders (SUD) and reentry initiatives that focus on supporting individuals who are transitioning from incarceration back into society. SUD and reentry initiatives can intersect with Section 1115 demonstrations and other authorities, such as managed care, in a variety of ways. The intersection of these issues can provide another area of common ground and opportunity to continue work on state reentry initiatives, though likely with new and modified federal parameters.
Connect With Us
HMA is monitoring other developments in Congress and from the White House and agencies affecting federal Medicaid and CHIP policy changes. The complexity and nuances associated with potential future statutory and regulatory changes necessitate thoughtful and immediate impact analysis, scenario planning, and preparations that will allow organizations to pivot if and when policy changes occur. HMA colleagues have expertise in all of the components critical to staying informed, engaged, and prepared for changes to Section 1115 programs—from the policy knowledge to actuarial/budgeting talent, to communications and project management skills, as well as the necessary IT infrastructure.
For questions about these developments and your organization’s plan to adapt to new federal Medicaid policy priorities, contact our featured experts below.
March 12, 2025
The Medicaid Pivot: New Developments in Section 1115 Demonstration Policy
HMA partners with Healthcare Association of New York State (HANYS) on webinar series to help organizations with Survey Readiness
In today’s complex healthcare environment, navigating the scrutiny of regulatory and accreditation bodies like The Centers for Medicare & Medicaid Services (CMS), Department of Health (DOH), The Joint Commission, and Det Norske Veritas (DNV) Healthcare is critical for the success of every hospital and health system. Unexpected surveys, triggered by recertification, validations or even complaints, can occur at any time.
Early this year, HMA partnered with the Healthcare Association of New York State (HANYS) to develop the content for Survey Readiness: Prepare, Respond, Succeed, a 5-part virtual series. HMA’s expert faculty co-taught the sessions. Attendees dove deep into organizational strategies and tactics to prepare, manage and respond to surveyors effectively – and get the essential skills to excel in survey readiness.
Survey Readiness: Prepare, Respond, Succeed
Virtual Series | April 2 – 30
- April 2: Survey readiness 101: Overview and getting started
- April 9: Preparation: How to mitigate risk and prepare for upcoming surveys
- April 16: They’re here: Establishing a survey response and management protocol
- April 23: Responding to survey findings: How to develop a strong correction plan and knowing your options
- April 30: What’s next: Leveraging survey findings and strengthening organizational quality and compliance