
December 20, 2023
CMS Transforming Maternal Health Model Offers State Medicaid Agencies an Opportunity to Accelerate Improvements in Quality and Outcomes
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
CMS Transforming Maternal Health Model Offers State Medicaid Agencies an Opportunity to Accelerate Improvements in Quality and Outcomes

Previously, HMA developed a comprehensive series of webinars reviewing the potential for using 1115 waivers to expand and improve health care services for the justice-involved population. With California becoming the first state earlier in 2023 to receive approval for the authority to provide a specific set of Medicaid services for up to 90 days in advance of release to youth and adults in state prisons, county jails, and youth correctional facilities, and many other states with pending waivers of a similar type, this blog post considers the implications of this emerging policy trend for local and regional managed care organizations (MCOs) in 2024.
Delivering Medicaid services through MCOs has become the dominant strategy employed by states with 41 states (including the District of Columbia) using managed care for at least certain Medicaid populations. Local and regional MCOs represent a key component in this landscape across the country and often are deeply rooted in the states and communities they serve because of their specific focus on a single or limited number of markets.
With the precedent now in place for federal authority (and federal financial participation) to provide services such as reentry case management, behavioral health and physical health consultation services (in-person or via telehealth), laboratory and radiology services, medications as well as medication administration, medication assisted therapy inclusive of counseling, and community health worker services, states have a clear pathway toward pursuing the ability to provide services for the justice-involved population prior to release. Among the many important implementation questions states will need to consider as they continue to pursue the authority to provide these services is how the specific services will be delivered and financed. Given the dominance of Medicaid managed care, states will have to grapple with how MCOs can be leveraged to support a successful implementation of the delivery of services to the justice-involved population. The strong community presence of local and regional MCOs within the Medicaid managed care ecosystem makes these MCOs important entities for states to consider. Local and regional MCOs should consider what role they believe they can play as partners to states in these initiatives to serve justice-involved populations as successfully as they have served other Medicaid populations.
While the opportunities for local and regional MCOs will evolve over time, initial opportunities to contemplate are as follows:
As more states with pending 1115 waivers for reentry services for the justice-involved population gain approval, local and regional MCOs should anticipate engagement from states on planning and implementation in in 2024. Given this, taking action early to engage state partners and prepare your organization to serve this population is a prudent step to consider now.
If you have questions about how HMA can support your efforts related to the Medicaid services for justice-involved populations and local and regional MCOs, please contact our experts below.
As a local or regional managed care organization (LRMCO), being “ready” means proactively addressing all the areas where your organization can get tripped up, or worse, lose your contract with a state Medicaid agency. LRMCOs are heavily reliant upon government funded programs. These include Medicaid, Medicare, and Marketplace business. Most LRMCOs are not as heavily involved in the commercial market, either on a fully insured or self-insured basis, and even when they are, these areas comprise smaller parts of their overall product offerings. National MCOs have looked to Medicaid managed care to fuel growth, strengthen relationships with government partners, and leverage infrastructure.
In any government program, “readiness” is a critical capability that often gets overlooked due to the daily pressures of running the organization. It’s often said that “you should always be audit ready.” The meaning of this is that you and your organization should always be prepared to undergo an outside audit from your regulator, financial auditor, or other entity such as the National Committee for Quality Assurance. Having a well-run organization allows you to not only be ready to respond to regulators or auditors but also to be able to demonstrate stable financial, operational, and compliance performance. Having this stable base of performance allows for more meaningful strategic planning, innovation, and state and federal partnership.
In Medicaid and other government programs, where public purchasers follow stringent purchasing rules, perhaps another way to think of your MCO’s operations is to always be “procurement ready.” But what does it mean to be “procurement ready” for your MCO? Today, managed care is the primary Medicaid delivery system vehicle for most states across the country. While some states procure all Medicaid managed care services in single, comprehensive contracts, many states procure for services via specific programs. Managed long-term services and supports, behavioral health, dental, and other programs are examples of specific programs that states procure alongside those that states have procured historically including low-income children and their parents, pregnant women, people with disabilities, people aged 65 and older, and, with advent of the Affordable Care Act, low-income adults without dependent children. State Medicaid managed care contracts are typically three to five years in duration, often with single or multiple year optional extensions. What this means is that in any given year there are approximately 10 Medicaid managed care program procurements. Moreover, these procurements are now among the largest contracts awarded by states, often exceeding billions of dollars per year. As a result, the importance of being ready for these events has grown substantially over the years.
A critical element of being “procurement ready” is not to rely upon fixing issues when a Medicaid request for proposal (RFP) appears likely; it is to be on top of requirements on an ongoing basis, address issues quickly, and capture success stories as they happen. Too often, LRMCOs don’t look to begin this process until it is too late—a small issue has become a big problem and remediation is expensive, time-consuming, and painful. Even the best proposal will struggle to win in the face of a record of real or perceived suboptimal performance.
The reality is that states are asking for MCO results (Healthcare Effectiveness Data and Information Set scores, state audit findings, Health Insurance Portability and Accountability Act breaches, etc.) as part of RFPs. These data points are hard to hide even with great writing and presentation. States are also more frequently including member or case “scenarios” in RFPs, which are specific in nature and are designed to have the MCO describe exact steps, processes, and outcomes. It is therefore important to monitor and measure for performance year-round.
For incumbent LRMCOs, the best way to maximize your chances of winning a renewal is to deliver effectively—and to be seen as delivering effectively—on your existing contract. A well performing incumbent LRMCO has tremendous advantages because:
The time to begin preparing for your next procurement is while you begin to deliver under the existing procurement, not three months before a new procurement.
Best practice is to begin RFP planning 18 months to 24 months in advance of the anticipated issuance date. That planning should include developing “win strategies,” competitive assessments, and proposal logistics. Putting remediation initiatives on top of these areas adds unnecessary stress and strain on the LRMCO and the teams responsible for delivering a winning proposal. Therefore, being “procurement ready” is an important and often critical element in ultimately preparing winning proposals.
States look for “partners” not just contractors. LRMCOs can serve as invaluable thought partners to help inform how states can meet their stated policy aims. This not only puts LRMCOs in good standing with state leaders, but it also means they are well informed about state thinking so they won’t be caught by surprise if new requirements appear in the next RFP.
States frequently provide vague guidance on when RFPs will be released (“early next year,” “in the second quarter”, etc.) Some states have published concrete schedules for their multiple RFPs, but this is the exception. The implication for LRMCOs is that it is very difficult to “time” when to get your operations optimally ready for a forthcoming RFP. A wiser approach is to always be ready for an RFP to drop (again, like being audit ready). Some operational, performance, or compliance issues can be addressed in fairly short time frames. Other areas, such as quality reporting, require about a two-year lead time to fix any problems, gather the data, and exhibit optimal performance due to data/reporting lag. Other areas that require longer lead times are claims, encounter data reporting, risk adjustment, delegation oversight, and many others. Due to the lead times required, to be always “procurement ready,” LRMCOs need to have robust operational readiness and monitoring programs established as part of daily operations.
As noted earlier, strong performance on audits and a consistent record of impressive compliance is an advantage when participating in RFP processes. States prefer to contract with MCOs that have a robust track record of compliance and can persuasively demonstrate their ability to consistently meet the needs of members. Strategies that LRMCOs can employ to develop such a track record include:
To be continuously “procurement ready,” LRMCOs must be forward-thinking and adaptive. Embracing change, data-driven decision making, quality improvement, building strong provider networks, investing in technology, engaging stakeholders, and maintaining financial stability are all essential steps to ensure the sustainability and success of these organizations in the intervening years between state-issued RFPs. By taking a proactive approach to addressing these needs, LRMCOs can position themselves as leaders in providing high-quality health care services for the members they serve.
If you have questions about how HMA can support your efforts to be ready, please contact our experts below.
This week, our In Focus section highlights the efforts of Health Management Associates (HMA) and partner organizations to better coordinate services for children in foster care and for children with behavioral health needs.
First, HMA released an issue brief on November 6, 2023, as part of a partnership between HMA and the National Association of State Mental Health Program Directors (NASMHPD) Technical Assistance Coalition. Together HMA and NASMHPD experts wrote a series of five briefs on children’s behavioral health.
The brief released last month, “The Role of Specialized Managed Care,” written by HMA experts Heidi Arthur and Angela Bergefurd, with input from Caitlin Thomas-Henkel and Uma Ahluwalia, centered on the intersection of child welfare reform and behavioral health transformation. More specifically, it described how specialized Medicaid managed care plans can ensure better alignment between child welfare and behavioral healthcare services.
The paper emphasizes the role of state-level special needs plans (SNPs) in the delivery of coordinated care and examines the opportunities afforded to states seeking to leverage specialty managed care plans.
Specialized managed care plans can help fill the void by incentivizing the provision of services for children in foster care and specialty services for children with behavioral health needs. Plans in three states — Washington, Arizona, and Ohio — are highlighted, and can serve as examples of how state Medicaid SNPs can be implemented.
This paper is part of a larger effort that HMA and several partner organizations are supporting. Stakeholders include:
The goal of these collaborations is to foster dialog between state agencies and stakeholders working to improve the well-being of children and youth with complex needs.
Most recently, HMA hosted a webinar on December 12, 2023, titled “Collaborating to improve children’s behavioral health – a comprehensive playbook to fostering wellbeing in children”. The webinar featured speakers from the partner organizations to discuss insights from a federal meeting that took place in November. Webinar speakers also informed participants about plans for a multistate policy lab scheduled for February 2024, where representatives of up to eight state child welfare agencies will participate in a two-day workshop on improving the children’s behavioral health continuum of care in their states. The webinar focused on the overall effort and provided a forum for states to hear from this partnership on the importance of collaborating to strengthen the children’s behavioral health system.
For questions about the brief, the webinar, or the larger effort, please contact our experts below.
The Role of Specialized Managed Care in Addressing the Intersection of Child Welfare Reform and Behavioral Health Transformation
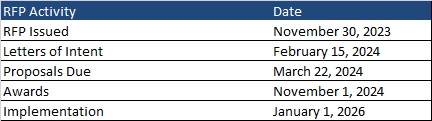
This week, our In Focus section reviews the request for responses (RFR) for the Massachusetts One Care and Senior Care Options (SCO) programs, released by the Massachusetts Executive Office of Health and Human Services (EOHHS) on November 30, 2023. The programs provide physical, behavioral, long-term services and supports (LTSS), and other community services to Medicare and Medicaid dual-eligible beneficiaries. Implementation is set to begin January 1, 2026.
One Care launched in 2013 as a Section 1115 Medicare-Medicaid Plan (MMP) program dual demonstration waiver. It operates under a financial alignment initiative (FAI) capitated model. The program provides integrated care to dual eligible adults ages 21 to 64. Individuals may remain enrolled in One Care when they turn 65 years old as long as they continue to meet all other requirements. Members can also access an independent LTSS coordinator.
As the Centers for Medicare & Medicaid Services (CMS) sunsets the FAI dual demonstrations, One Care will shift to a Fully Integrated Dual Eligible Special Needs Plan (FIDE SNP) beginning in 2026, pending federal approval of the Section 1115 amendment request. Members will have exclusively aligned enrollment with the same plan for both Medicare and Medicaid coverage.
SCO launched in 2004 and is currently a FIDE SNP with exclusively aligned enrollment. Medicaid enrollees ages 65 and older with or without Medicare are eligible. Enrollment in this managed care program is voluntary. Individuals on the Frail Elder Waiver can only join SCO.
Massachusetts will award separate contracts for One Care and SCO but may prefer bids from plans seeking to operate both; however, plans may submit bids to operate one type of plan. The state seeks to offer both One Care and SCO coverage for eligible individuals in as many counties as possible, and ideally statewide. Plans must propose to cover people in at least six counties for each type of plan.
To be selected, plans will need to have a contract with CMS to operate a FIDE SNP in Massachusetts in 2026. Applications must be submitted to CMS by February 2025.
Letters of intent are due February 15, 2024, and the deadline for responses is March 22, 2024. Plans will be selected by November 1, 2024. Implementation is set to begin January 1, 2026. Contracts will run an initial five-year term through December 31, 2030. Contracts may be renewed for up to five years in any increment.
Commonwealth Care Alliance, Tufts, and UnitedHealthcare serve 43,000 One Care members.
SCO incumbents WellSense Senior Care Options (formerly BMC Healthnet), Commonwealth Care Alliance, Fallon Health, Molina/Senior Whole Health, Tufts, and UnitedHealthcare serve 77,000 members.
Previously, Wakely Consulting Group, an HMA company, reviewed aspects of the Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA) requirements proposed rule published by the Internal Revenue Service (IRS), Employee Benefits Security Administration (EBSA), and Centers for Medicare & Medicaid Services (CMS) on August 3, 2023. The agencies accepted comments on the proposed rule through October 17, 2023. Because the proposed rule, if finalized as put forward, will have a significant impact on the compliance obligations of managed care organizations (MCOs) related to mental health parity requirements for the 2025 plan year in the group market and 2026 plan year in the individual market, MCOs will need to ensure, as they enter 2024, that they are in a position undertake any necessary steps to meet such obligations. This blog post outlines three specific requirements in the proposed the rule related to non-quantitative treatment limitations (NQTL) and their implications for a subset of MCOs: regional and local MCOs.
In the proposed rule, the IRS, EBSA, and CMS restate that MCOs may not apply any NQTL to mental health/substance use disorder (MH/SUD) benefits in any classification that is more restrictive, in policy or practice, than the predominant NQTL that applies to substantially all medical/surgical benefits in the same classification. To ensure compliance with this requirement, the proposed rule specifies exactly how an MCO must determine if the requirement is met.
First, the proposed rule outlines in detail how an MCO must complete a quantitative calculation to determine whether an NQTL applies to substantially all medical/surgical benefits in the classification at issue. If the NQTL does apply to substantially all medical/surgical benefits in the classification, the proposed rule then outlines exactly how the MCO must determine what version of the NQTL counts as the predominant one within the classification as well. Finally, once the predominant variation of the NQTL is established for an NQTL that applies to substantially all medical/surgical benefits in the classification, an MCO would have to use the proposed rule’s definition of “restrictive” (i.e., “imposes conditions, terms, or requirements that limit access to benefits under the terms of the plan,”) to determine if the NQTL applied to the relevant MH/SUD benefit is no more restrictive than the applicable medical/surgical benefit NQTL.
For local and regional MCOs, while the no more restrictive standard is not new, the steps required to ensure compliance likely represent—at the very least—an area where materially more intensive and sophisticated capabilities will need to be brought to bear. Completing the steps outlined above will require a cross-functional approach that leverages such areas as actuarial, behavioral health, clinical, compliance, financial analytics, and legal. The necessary people and processes will need to be deployed not only to accomplish the work effort but to do so in a way that is intelligible to federal and state regulators.
In the proposed rule, the IRS, EBSA, and CMS seek to make explicit a requirement which mandates that MCOs cannot impose an NQTL on MH/SUD benefits in any classification unless the factors used in designing and applying the NQTL to MH/SUD benefits in the classification are comparable to, and are applied no more stringently than, the factors used in designing and applying the NQTL to medical/surgical benefits in the classification. The agencies note that the regulatory revisions offered only seek to codify what has been a longstanding position of the agencies on this issue.
The most notable and innovative provision put forward by the agencies for purposes of determining comparability is one that would prohibit MCOs from relying on any factor in the design or application of an NQTL if the information on which the factor is based discriminates against MH/SUD benefits when compared to medical/surgical benefits. In this context, the proposed rule makes clear that discriminating against MH/SUD benefits means being biased or not objective, in a manner that results in less favorable treatment of MH/SUD benefits, based on all the relevant facts and circumstances.
For local and regional MCOs, it is advisable, given both the prudence of mitigating forthcoming potential compliance risks and likely limitations on the resources that can be devoted to compliance efforts in a discrete time period, to begin to evaluate upon entering 2024, whether NQTLs imposed on MH/SUD benefits have been designed and applied in a way that comports with this proposal by the agencies. For example, an MCO should evaluate whether factors currently employed rely on historical data or other historical information from a time when coverage was not subject to MHPAEA or was in violation of MHPAEA’s requirements where the use of such data results in less favorable treatment of MH/SUD benefits, as this would be prohibited. To this point, the agencies specifically note that MCOs would not be permitted to calculate reimbursement rates based on historical data on total spending for each specialty that is divided between MH/SUD providers and medical/surgical providers, when the total spending was based on a time period when coverage was not subject to MHPAEA or was in violation of MHPAEA, if the data results in less favorable treatment of MH/SUD benefits.
In the proposed rule, the IRS, EBSA, and CMS note that substantially disparate results are often a red flag that an MCO may be imposing an NQTL in a manner that does not comply with MHPAEA and so the agencies have included a proposal to add a requirement that, when designing and applying an NQTL, an MCO must collect and evaluate relevant outcome data in a manner reasonably designed to assess the impact of the NQTL on access to MH/SUD benefits and medical/surgical benefits as well as consider the impact as part of the MCO’s analysis of whether such NQTL complies with MHPAEA.
At minimum, MCOs would have to collect and evaluate data for all NQTLs that includes, but is not limited to, the number and percentage of relevant claims denials, as well as any other data relevant to the NQTLs as required by state law or private accreditation standards. Furthermore, due a specific concern of the agencies about network composition, the proposed rule would mandate that MCOs also collect additional applicable data for NQTLs that relate to network composition such as in-network and out-of-network utilization rates, network adequacy metrics (i.e., time and distance data and data on providers accepting new patients), and provider reimbursement rates. To the extent that data collected and analyzed demonstrates significant differences in access to MH/SUD benefits when compared to medical/surgical benefits, the MCO would be required to take reasonable action to address these differences in access as necessary to ensure compliance with MHPAEA.
For local and regional MCOs, beginning in 2024 to inventory readily available data sources that would be able to be leveraged to comply with this proposal is an important step in order to be prepared to comply during the 2025 plan year in the group market and 2026 plan year in the individual market. Additionally, assessing analytic capabilities to determine the level of readiness to be able to complete the evaluation based on the data collected is also an important component of preparing for this proposed new compliance obligation.
If you have questions about how HMA can support your efforts related to the proposed rule’s implications for local and regional MCOs, please contact our experts below.

HMA was engaged by the Washington, District of Columbia Department of Health Care Finance (DHCF) to lead their Medicaid Business Transformation D.C. Initiative, assessing the technical assistance needs of Medicaid providers and organizations in the areas of legal analysis, budgeting, and business development as they move toward value-based care arrangements. HMA partnered with the D.C. Behavioral Health Association (BHA), Medical Society of the District of Columbia (MSDC), D.C. Primary Care Association (DCPCA), and DHCF to engage, recruit, and collaborate with organizations and stakeholders across the District.
The HMA team implemented a mixed-methods assessment approach that included a literature review of national value-based payment (VBP) best practices, focus groups, interviews, and a technical assistance (TA) survey of District organizations, agencies, and stakeholders. This strategy identified the TA needs of District healthcare providers that informed the design of an intensive 3-month technical assistance program that included a variety of tools, webinars, and trainings. All resources and tools are available on the Integrated Care DC webpage. View the report and other information about the program published this week.
Experts from HMA as well as Wakely Consulting Group and Lovell Communications, both HMA subsidiaries, contributed to this report. We offer our clients a wide range of deep technical, analytical, policy, and communications support to providers, state agencies, and recommendations on ways to improve value-based payment models.
Report authors include Caitlin Thomas-Henkel, Suzanne Daub, Art Jones, Hunter Schouweiler, Amanda White Kanaley, and Vicki Loner. It was peer reviewed by Jean Glossa and Sam DiPaola.

This webinar was held on December 12, 2023.
Beyond the statistics lie the stories of countless children and families needing immediate and critical access to behavioral health services and community-based supports. Addressing these issues requires comprehensive cross-system reforms, including policies that promote integrated financing, enhanced care coordination, increased provider collaboration, and bolster upstream prevention efforts. HMA is working with these national partner organizations to prioritize and focus on cross system integrated and interoperable solutions to address the needs of children, youth, and families with complex behavioral health needs.
HMA hosted a webinar in partnership with the National Association of State Mental Health Program Directors (NASMHPD), National Association of Medicaid Directors (NAMD), Child Welfare League of America (CWLA), American Public Human Services Association (APHSA), and with support from the Annie E. Casey Foundation, Casey Family Programs and other funders. Together, these organizations have developed a multi-state policy lab to be held in February 2024. Applications for state agency participation opened the week of November 11th. State agency decision makers can click here to fill out and submit your state agency’s application. This webinar focused on the overall effort and for states to hear from this partnership on the importance of collaborating to strengthen the children’s behavioral health system.
If the link above to the online form causes problems or does not work for you, please use this fillable PDF application and send it to [email protected] with all relevant attachments. Applicants must submit the full application no later than 5 pm on December 20, 2023.
Key highlights of this webinar include:
Featured Speakers:
Julie Collins, MSW, LCSW, VP, Practice Excellence, CWLA
David Miller, M.P.Aff., Senior Operations & Project Director, NASMHPD
Sheila Poole, Vice President, External Relations, APHSA
Joe Ribsam, JD, Child Welfare and Juvenile Justice Policy Director, AECF
Proposed Changes to Opioid Treatment: What They Will Mean for Providers, Payers, and Regulators
