HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
On Tuesday, April 11, 2023, HMA hosted a Future Frame Conversation covering some of the changes outlined in the recent 2024 Medicare Advantage (MA) Rate Announcement. This cycle signals a new era for MA funding and risk adjustment. The Final Rate Announcement, in particular the new risk adjustment model to be phased in over three years, will spark stakeholders to reevaluate benefit design through the bid cycle and risk adjustment strategies in the future. These refinements will impact both health plan and provider reimbursement.
During the discussion:
Amy Bassano from HMA talked about the CMS strategy for these changes; and
Tim Murray from Wakely Consulting, an HMA company, discussed how payers should be using data and analytics to evaluate and forecast the impact of CMS changes.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
The Biden administration has announced that the COVID-19 pandemic Public Health Emergency (PHE) declaration will expire on May 11, 2023. The end of the declaration and other changes in federal policy have significant implications for state Medicaid programs, including the end of a 6.2% increase in the regular federal medical assistance program (FMAP) matching rate for states and continuous enrollment requirements put into place early in the pandemic. This means that an estimated 4-14 million Americans, especially including women and children, will need to engage in state processes for re-certification to continue their Medicaid benefits and states will lose their enhanced matching.
While state have been planning for these changes, collectively referred to as “PHE Unwinding,” the public health implications of these shifts have received little attention. As millions of Americans lose Medicaid benefits, as a result of “PHE Unwinding,” public health departments nationwide are likely to face additional demands and pressures that are also critically important for states to consider. State public health agencies that have spent the last several years responding to the COVID-19 pandemic are now entering a new phase. During the CMS-recommended 12-month period that states have to complete their redeterminations, public health agencies may see increasing numbers of individuals who were previously eligible for Medicaid and other safety net services seeking access to public health programs. Public health officials also may be called on to address the community health impacts of the newly uninsured or those who have lost other benefits, such as enhanced Supplemental Nutrition Assistance Program (SNAP) dollars for food. Addressing challenges may require significant attention of Community Health Workers or other workforces engaged across public health and healthcare and take precedence over other public health priorities. All of this will be happening at a time when public health officials are being called on to re-imagine their infrastructure needs, including reconfiguring and modernizing their data systems.
Public health agencies planning for this immediate future may benefit by taking a systems approach to PHE unwinding and considering a few key variables in their planning—
1.The end of the PHE may rapidly increase demand for public health safety net programs.
Medicaid provides coverage for the sickest and most vulnerable. As redetermination processes leave some without insurance and other benefit programs like SNAP return to pre-pandemic coverage, historically marginalized and medically at-risk populations will be disproportionately impacted. This may result in increased demand for safety net programs usually found in public health departments that serve the under and uninsured, such as the Breast and Cervical Cancer Prevention Program (BCCP) that provides cancer screening for women, and Vaccines for Children (VFC) which provides required immunizations to school-age children who otherwise lack access. Programs such as the Women, Infants and Children (WIC) and perinatal home visiting programs that serve families with limited economic resources may also see increased numbers of eligible families. Health departments can quantify these increases by assessing their populations, estimating increases, and using their existing data to determine which communities and geographic areas are likely to exhibit the greatest needs, and then share this information with policymakers.
2.Unwinding may represent an opportunity to educate legislators and policymakers on the connection between Medicaid utilization and public health programs.
As states see decreases in federal matching for their Medicaid programs, policymakers will look for opportunities to fill gaps in the state share of operating these programs. Public health programs, which are usually run with a combination of state dollars and federal grants, are often looked at as potential sources to fill gaps in Medicaid program costs. Moreover, public health officials may be able to move upstream of these discussions by ensuring that states are maximizing the federal Medicaid match (FMAP) on any public health services that can be billed to Medicaid, including using waivers and state plan amendments to cover services such as maternal home visiting or tobacco cessation under Medicaid, thus stretching grant and state dollars further while covering more individuals. While public health has long discussed the benefits of calculating and sharing the long-term return on investment of public health services, officials may also wish to consider utilizing risk stratification strategies to identify short-term cost savings and cost avoidance to other state programs of the services offered by public health departments. At the local level, health departments are often closely involved in the delivery of services that keep children in school, adults at work, and protect people in hospitals and nursing homes from health care acquired infections. All of these services have immediate benefits to state and local economies.
3. New funding for public health infrastructure, data modernization, and workforce development represents an opportunity to drive collaboration between public health, Medicaid, and other sectors.
As a part of the American Rescue Plan, state public health agencies have received funding from CDC to strengthen their infrastructure to ensure that communities have the people, services, and systems to promote and protect public health. The grants are intended to allow states to focus on increasing the size and diversity of the public health workforce; modernize data systems; and ensure states can demonstrate the foundational capabilities of public health. CDC has affirmed its expectation that states will prioritize collaboration and organizational partnerships as part of these efforts. As state public health agencies use these federal investments to impact programs that reach priority populations and improve health outcomes, several opportunities to reach disadvantaged populations and improve their health outcomes become apparent. For example, public health agencies working collaboratively with state departments of education could lead to partnerships around school-based clinics or workforce training programs, while engaging with the private healthcare and laboratory sectors on data and disease surveillance seems promising. Health departments should start now to in preparation for the flurry of activity that will be sparked in the wake of the PHE. This might involve reaching out to potential partners or organizing town-hall-style” active listening sessions with citizens to meet people where they are and better understand the needs of the community they serve.
HMA and HMA companies will continue to analyze the public health implications of the Medicaid Unwinding and the end of the PHE. We have the depth and breadth of expertise to assist with capacity building, data collection and management, and population health analysis.
HMA can support your agency before or after the end of the PHE.
This week our In Focus section reviews the Florida Statewide Medicaid Managed Care Program (SMMC) Invitation to Negotiate (ITN), released on April 11, 2023, by the Florida Agency for Health Care Administration (AHCA). SMMC consists of three programs: Managed Medical Assistance (MMA), Long-term Care (LTC), and dental, covering 4.4 million individuals. This ITN is for contracts to provide MMA and LTC.
Under the SMMC program, all enrollees receive their services from a single plan providing managed medical assistance, long-term care, and specialty benefits. (Dental benefits are provided separately.)
AHCA will select plans that will achieve the agency’s goals, including providing healthy birth outcomes for mothers and their infants, improving childhood and adolescent mental health, maximizing home and community-based placement and services, and supporting the HOPE Florida program. HOPE Florida utilizes ‘Hope Navigators’ to help individuals achieve economic self-sufficiency, develop long term-goals, and map out a strategic plan by focusing on community collaboration between the private sector, faith-based community, nonprofits and government entities.
Additionally, with the new contracts, AHCA will implement the following changes:
Specialty plans will no longer be awarded separately but must be awarded to a comprehensive or MMA plan.
Enrolling voluntary recipients (such as individuals with intellectual or developmental disabilities) into the SMMC program and providing the opportunity for them to opt out
AHCA may mandatorily enroll into the MMA program full benefit dual-eligibles who are also in a Medicare Dual Eligible Special Needs Plan (DSNP).
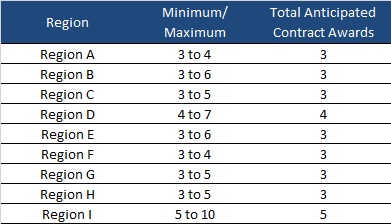
AHCA will invite 10 plans to negotiate for awards as shown below:
Timeline
Proposals are due August 15, 2023, with an anticipated award date of December 11. Contract will run from October 1, 2024, through December 31, 2030. Contracts may not be renewed, but AHCA may extend the term to cover any delays during the transition to a new plan.
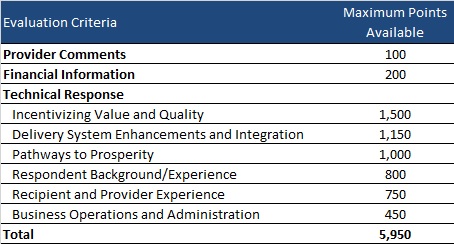
Evaluation
Plans can receive a total maximum number of points of 5,950. AHCA will invite top-ranking plans to negotiations to ensure that AHCA can enter into contracts with the minimum required number of plans per region.
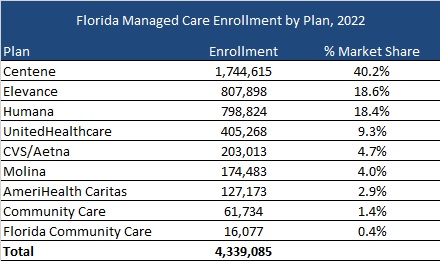
Current Market
As of December 2022, Florida served 4.3 million MMA and LTC enrollees, excluding an additional 97,000 Children’s Medical Services enrollees in the Children’s Medical Services Network plan. Centene had the highest market share based on enrollment, at over 40 percent.
A significant percentage of individuals in American jails and prisons have a substance use disorder (SUD), with those with opioid use disorder (OUD) at especially high risk of death due to overdose upon release from incarceration.1 At the same time, overdose deaths during incarceration continue to increase.2,3
Medications for opioid use disorder (MOUD) and medication assisted treatment (MAT) programs reduce in-jail overdose death by 50% and the risk of overdose death after release by 60%. MAT programs also redress substantial racial and ethnic health disparities4. Despite these proven benefits, most incarcerated Americans do not have access to this treatment. Barriers to MAT implementation include lack of resources such as money, trained staff, and leadership; stigma toward both SUD and MOUD; and limited system ability to support adaptive change.
KEY MODEL ELEMENTS AND PROMISING RESULTS
Health Management Associates (HMA), a national research and consulting firm focusing on publicly funded healthcare, developed a MAT implementation support model working with dozens of jails and prisons across the United States, rapidly scaling access to MOUD/MAT during incarceration. This implementation support model fosters both technical and adaptive change using a learning collaborative structure and adult-learning theory. The model also acknowledges the unique environment of each jail and prison and the challenges of providing healthcare services for a complex condition like OUD in a correctional setting. This model program is straightforward, documented, proven, and readily replicated.
The model provides participating jail and prisons teams with access to robust individualized technical assistance and coaching; peer-to-peer support and learning; training; and collaborative educational sessions. This approach recognizes that multidisciplinary teams inclusive of custody/security staff; medical personnel; behavioral health providers; and others must be convened and supported as a cohesive unit to effectively implement MOUD and MAT programs in jails, prisons, and the justice and addiction ecosystems. This ecosystem view incorporates the critical partners and pathways outside the jail and prison to support effective re-entry to the community following incarceration to support recovery. A change management and continuous quality improvement framework is foundational to the model.
In the California, Illinois and Michigan county jail team learning collaboratives, county teams receive implementation grants or stipends. Over the course of the projects these amounts have ranged from $15,000 to over $100,000 per county, which were included in the project budget from the funding source (State Opioid Response in CA and IL; state general funds in CA). Offering this “seed money” serves as an incentive to help counties engage in the learning collaborative. HMA has managed all aspects of these implementation grants/stipends.
Evaluation
Collection and analysis of data informs ongoing technical assistance and demonstrates the rapid scaling and positive impact of the program. In the state learning collaborative programs, deidentified data is collected from county jail teams and analyzed and compiled to reflect trends and progress in the implementation effort. Where HMA supports state departments of correction with MOUD and MAT implementation, HMA assists the prison system with identifying and using key data points to inform a continuous quality improvement process.
Funding
The MOUD and MAT county jail implementation model was initiated in 2018 in California’s MAT in Jails and Drug Courts program with demonstrated impact for expanding access to MAT in the state’s county jails. The project was funded with federal State Opioid Response dollars administered by the California Department of Health Care Services (DHCS) through September 2022. The California legislature approved state general funds to support continuation of the program from October 2022 through June 2025.
Illinois’ Department of Health Services Substance Use Prevention and Recovery (SUPR) sponsored implementation of that state’s learning collaborative beginning in 2021 with federal State Opioid Response Dollars. It is currently funded through June 2024 with plans to extend the learning collaborative under a new SOR funding cycle.
Michigan Department of Health and Human Services elected to implement the county jail learning collaborative in late 2023, funding it with state opioid settlement funds for continuation through November 2026.
HealthCare Access Maryland in support of the Maryland Governor’s Office of Crime Prevention, Youth, and Victim Services deployed this model for a limited three-month period with HMA to increase access to MOUD for incarcerated persons. The impetus for this project was the OUD Examinations and Treatment Act, which requires local jails/jurisdictions in Maryland to offer all forms of MOUD.
Michigan Department of Corrections has engaged HMA for years as its contracted third-party health care evaluator. HMA supported the DOC’s MAT implementation across multiple sites in the Michigan prison system with state general funds from 2020-2022.
HMA supported the Alaska Department of Corrections with widescale MAT implementation under a contract through state general funds 2022-2023.
RESULTS
HMA’s successful model incorporates strategies that overcome typical barriers to MOUD/MAT implementation in corrections settings.
In the California learning collaborative, HMA has engaged 41 county jails over four years resulting in 35,000 person-months5 of individuals on MAT with counties participating representing almost 90 percent of the state’s total population.
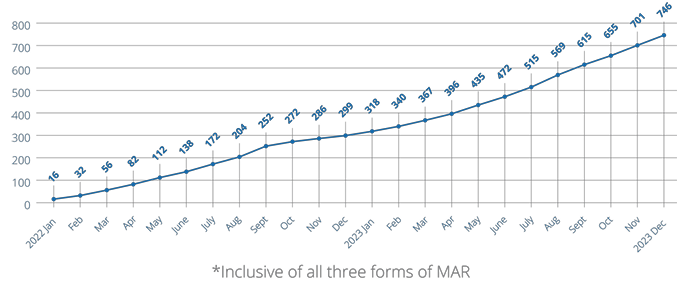
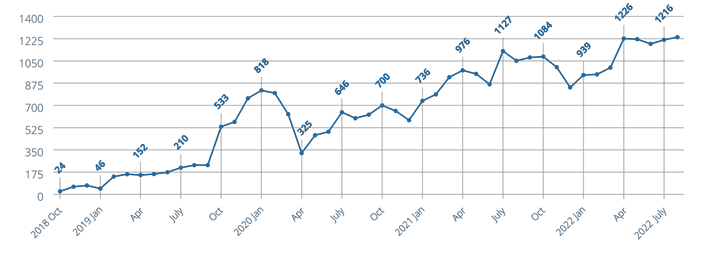
In the Illinois learning collaborative, HMA has engaged 28 counties over three years resulting in over 720 unique individuals receiving MAT in jails with participating counties representing 64 percent of the state’s population (Cook County is excluded because of an evolved MAT program prior to inception of Illinois’ county learning collaborative).
Figure 1. Running total of unique individuals who have received MAR in Jail in Illinois from inception of data collection from counties through December 2023. (MAR is medication assisted recovery – the term used for medication assisted treatment in Illinois.)
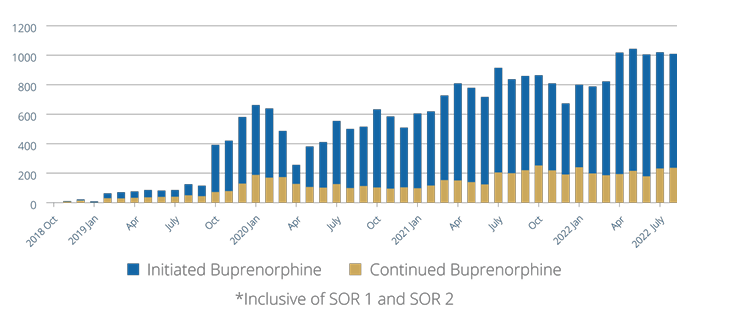
Figure 2. Running total of person-months individuals who have received MAT in jail in California participating jails from program inception through August 2022
Figure 3. Running total of person-months individuals were initiated or continued on buprenorphine in California participating jails from program inception through August 2022
STRATEGY/APPROACH/INTERVENTIONS
HMA coaches and subject matter experts (SMEs) understand and respond to the unique regulatory oversight, policies, and procedures in jail and prison operations, requiring customized approaches to introduce and expand MOUD and MAT access. Both adaptive and technical change strategies are deployed to assist jails and prisons in changing their culture and operations to treat SUD like other chronic, treatable diseases. HMA coaches and SMEs stay deeply involved with implementation teams to initiate and support change over time.
County jail teams in the learning collaborative and DOC site teams are assigned an HMA coach who understands and supports their individualized operations, resource capacity, and goals. The coach convenes an in person-team meeting and initial facility walk-through to jump start the initiative and inform ongoing team implementation goals and activities. The coach assists the team in establishing and executing goals and action steps that align with the overarching goals of the learning collaborative or DOC system.
All county teams are regularly convened for collaborative learning sessions to support their implementation plan on an ongoing basis. These sessions include fundamental information on MAT/MOUD and related components of evidencebased SUD treatment in corrections settings. Coaches identify challenges and barriers at their sites and these themes inform sessions at additional learning collaborative convenings. These identified themes are also targeted with training and hands-on coaching support (e.g., biases against MAT among providers and custody staff; custody concerns about diversion of medications; payment mechanisms for the medications; and sufficient staff capacity to offer the treatment).
Critical elements of the change effort include:
Improved SUD screening, assessment, treatment options, and planning to include at least two forms of MAT are core themes and goals of the learning collaborative. This messaging and expectation accelerate implementation by “setting a bar” for teams’ efforts while providing them with individualized assistance to overcome challenges in meeting their goals.
Engagement across the treatment ecosystem including advisors from state associations of counties, sheriff departments, treatment providers, and the state prison system connects the counties with emerging policy and best practices from their professional peers.
Multidisciplinary teams: MAT in jails and drug courts requires an integrated approach inclusive of medical and behavioral health care staff, custody/security and other justice professionals, and county providers and leadership.
This implementation model drives rapid, systemic change that would likely not be possible with individual site efforts. Scaling is accelerated by the learning collaborative model in which barriers that are identified by multiple county or DOC site teams, such as regulations for methadone access to incarcerated individuals or practice of a healthcare vendor serving multiple sites, are addressed at the levels of state policy or corporate leadership and addressed in group learning opportunities.
Lessons Learned
The approach needs to be tailored to each jail and county – and for departments of correction, each DOC site – who have resources, concerns, and goals unique to them. For example, a DOC reception center will have different security and programming requirements and workflows than a general detention center. A rural county with an average daily population of 15 and intermittent nursing and provider access has different resources than a suburban jail with an average daily population of 500. The technical assistance must incorporate this understanding and meet each site where they are to be effective.
The aim – improved SUD treatment systemwide including transitions when individuals enter the corrections system and again at release – needs to be addressed as a countywide problem that needs a comprehensive ecosystem solution. Or, in the cases of departments of corrections, system and statewide perspective and strategies are required.
Implementation of MAT in jails should be sponsored by the sheriff, and key partners from probation, jail custody, jail healthcare, drug courts, local county drug treatment programs, and the county administrator’s office must be included in planning and implementation. Implementation of MAT in departments of corrections must be endorsed and actively supported by the highest levels of leadership in the system and at each prison location.
Do not underestimate the prevalence and impact of stigma. There is an ongoing need for broader education about substance use disorders and treatment including about MAT and MOUD. All stakeholders and those impacted by opioid use disorder need to understand that substance use disorder is a chronic brain-based disease and that MAT/MOUD is effective treatment – not use of a substance that is problematic, i.e. “MAT is just replacing a drug with another drug.”
It is important to build supportable, sustainable implementation plans. If teams are not given sufficient support and opportunity to evolve in their understanding and development of the implementation program they may fail. At the same time a sense of urgency is important because people are dying due to lack of access to needed treatment.
ABOUT HMA
HMA is a leading independent research and consulting firm with more than 500 consultants with expertise across all domains of publicly funded healthcare and human services. HMA has distinguished itself from other consulting companies with our decades-long tradition of hiring senior-level policymakers, healthcare system leaders, and other experts with hands-on experience.
1 National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services.
This week, our In Focus section reviews the recently announced major policy updates from the Centers for Medicare and Medicaid Services (CMS) that affect the Medicare Advantage (MA) and Part D programs.
First, on January 30, CMS released the final Risk Adjustment Data Validation Final Rule, a highly anticipated and controversial policy that establishes the agency’s approach to auditing MA Organizations’ (MAOs) risk-adjustment payments and collecting overpayments as needed. Second, CMS released the CY 2024 Advance Notice for MA Capitation Rates (Part C) and Part D Payment Policies on February 1, 2023. Read HMA’s summary of the advance notice.
Most recently, on March 31, 2023, CMS released the CY 2024 Final Rate Notice for Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies, which incorporates CMS’s responses to public comments on the Advance Notice. These changes reflect CMS’ continued efforts to strengthen oversight in the MA program, including improving payment accuracy, and implementation of Part D policies from the Inflation Reduction Act (IRA).
Below are highlights of some of the key provisions of the CY 2024 Final Rate Notice and significant changes CMS made from the Advance Notice to the Final Rate Notice.
Risk Adjustment: The Final Rate Notice details the updated risk adjustment model using restructured condition categories based on ICD-10 codes, newer data, and clinical adjustments made to ensure the conditions are stable predictors of costs in the model. Specifically, diagnoses data will come from 2018 rather than 2014 and expenditure data will come from 2019 rather than 2015 to reflect changes in costs. These updates should more accurately reflect the cost of caring for beneficiaries and make payments less susceptible to discretionary coding that can lead to excess payments to MA plans.
Also, CMS changed course from its initial proposal in the Advance Notice to implement the above risk adjustment model changes fully in 2024, and instead decided to phase in these changes over three years. The updated risk adjustment policy will be phased in over three years for organizations other than PACE. As a part of the agency’s phase-in plan, 67 percent of the CY 2024 risk adjustment will come from the risk scores measured under the 2020 adjustments and 33 percent will come from the 2024 adjustments. In CY 2025, 67 percent of the risk adjustment will come from the 2024 adjustment. In 2026, 100 percent of the risk adjustment will come from the 2024 adjustment. For PACE organizations in CY 2024, CMS will continue to use the 2017 risk adjustment model and associated frailty factors to calculate risk scores.
Effective Growth Rate: The effective growth rate identified within the Final Rate Notice for CY 2024 is 2.28%, up from 2.09% in the Advance Notice. The Effective Growth Rate is largely driven by growth in Medicare Fee-for-Service expenditures. CMS will phase in a technical adjustment to remove MA-related indirect medical education and direct graduate education costs from the historical and projected expenditures. The technical adjustment to the Effective Growth Rate will be phased in over three years, where 33 percent of the adjustment will apply in CY 2024, 67 percent in CY 2025, and 100 percent in CY 2026.
Payment rate impact in MA: CMS expects that average payments to MAOs will increase by 3.32 percent in CY 2024 because of the finalized rate announcement, which is higher than the 1.03 percent increase outlined in the Advance Notice. This will result in an estimated $13.8 billion increase in MA payments for CY 2024.
Medicare Part D: The changes from the Inflation Reduction Act to the Part D drug benefit will be implemented as described in the Advance Notice. The changes for CY 2024 include:
Elimination of cost sharing for covered Part D drugs for beneficiaries in the catastrophic phase of coverage.
Increased income limits from 135 percent of the federal poverty limit (FPL) to 150 percent of the FPL for the low-income subsidy program (LIS) under Part D for the full LIS benefit with a $0 deductible.
Continuation of the policy to not apply the deductible for any Part D covered insulin product. Also, in the initial coverage phase and the coverage gap phase, cost sharing must not exceed the applicable copayment amount, which for CY 2024 is $35 for a month’s supply of each covered insulin product.
Continuation of the policy not to apply the deductible to any adult vaccine recommended by the Advisory Committee on Immunization Practices (ACIP). Also, the statute requires these vaccines to be exempt from any co-insurance or other cost sharing, including cost sharing for vaccine administration and dispensing fees for such products, when administered in accordance with ACIP’s recommendation, for beneficiaries in the initial coverage and coverage gap phases.
Base beneficiary premium (BBP) growth will be held to no more than 6 percent by statute. The BBP for Part D in 2024 will be the lesser of the BBP for 2023 increased by 6 percent or the amount that would otherwise apply under the original methodology if the IRA were not enacted.
Star Ratings: Medicare Advantage star ratings for CY 2024 will include 30 measures with 12 included in the 2024 categorical adjustment index (CAI) values. By contrast, Part D star ratings for CY 2024 will include 12 measures with 5 of those measures included in the 2024 CAI values. The CAI for the 2024 Star Ratings is expected to be issued later in 2023. The CAI was introduced in 2017 as an interim analytical adjustment to address the average within-contract disparity in performance among beneficiaries who receive a low-income subsidy, are dual eligible, and/or are disabled.
The Final Rate Notice also includes three criteria for determining if Part C and D organizations are eligible for the “extreme and uncontrollable circumstances” adjustment to their Star Ratings. To be eligible, an organization must be in a 1) service area that is within the “emergency area” during the “emergency period,” 2) service area that is within a geographic area designated in a major disaster declaration under the Stafford Act and the Secretary exercised authority under the Act based on the same triggering events, and 3) a certain minimum percentage (25 or 60 percent) of beneficiaries must reside in the Federal Emergency Management Agency (FEMA) designated Individual Assistance area at the time of the extreme and uncontrollable circumstance. If an organization meets the criteria outlined and meets the 25 percent minimum, then they will receive the higher of their measure-level rating from the current and prior Star Ratings years for purposes of calculating the 2024 Star Ratings. For organizations meeting the 60 percent minimum and the other criteria, they are excluded from the measure-level cut point calculations for non-CAHPS measures, and the performance summary and variance thresholds.
Upcoming LinkedIn Live: Join HMA for our Future Frame Conversation on Policy Changes in Medicare Advantage and the Implications for Coding, Risk Adjustment, and Reimbursement. Tuesday April 11, 2023, at 12 p.m. E.T.
If you have questions about the contents of CMS’s MA final notice and how it will affect MA plans, providers, and patients, contact our featured experts below.
Jay Rosen, founder, president, and co-chairman of Health Management Associates (HMA), today announced the firm’s acquisition of Crestline Advisors, an Arizona based healthcare consulting firm.
Founded in 2013, Crestline Advisors supports health plans, provider organizations, and state agencies with an array of services designed to help them navigate the changing healthcare landscape. The company’s team of independent consultants has an extensive track record of developing successful RFP responses, provider networks, and business development strategies to fuel client success.
“Crestline Advisors brings an impressive mix of expertise and relentless client focus – that delivers results – to HMA,” Rosen said. “Their ability to consistently develop winning proposal responses for Medicaid managed care organizations (MCO) complements our extensive MCO supports as we continue to expand the ways in which we serve our clients.”
In addition to Crestline’s proposal response development and MCO network management and operations support services, the company also assists clients with regulatory and contract compliance, accreditation, and strategic planning for business development.
“Crestline has demonstrated a commitment to supporting health plans, providers, and states to improve healthcare for Medicaid beneficiaries,” said Crestline CEO Susan Dess. “We firmly believe that as part of the HMA family of companies we will bring even more success to our clients and drive continued growth and development in Medicaid healthcare delivery.”
Dess and Tim Mechlinski will continue to lead Crestline Advisors, an HMA Company, as managing directors. Terms of the transaction were not disclosed.
About HMA
Founded in 1985, HMA is an independent, national research and consulting firm specializing in publicly funded healthcare and human services policy, programs, financing, and evaluation. Clients include government, public and private providers, health systems, health plans, community-based organizations, institutional investors, foundations, and associations. With offices in more than 20 locations across the country and over 500 multidisciplinary consultants coast to coast, HMA’s expertise, services, and team are always within client reach. Learn more about HMA at healthmanagement.com, or on LinkedIn and Twitter.
About Crestline Advisors
Established in 2013, Crestline Advisors, LLC is a consulting company designed to support the needs of health plans, provider organizations, and state agencies. Crestline specializes in helping large and small organizations operate successfully and grow despite the constant operational, financial, and political challenges they face. Crestline uses its current understanding of industry drivers to strategize with our clients so they can respond timely and effectively to small, large, or enormous market-place changes. Learn more about Crestline Advisors at crestlineadvisors.com.
Health Management Associates (HMA) is a national leader in supporting states with the design, development, negotiation and implementation of Section 1115 demonstration waivers and waiver extensions. HMA has assisted more than 20 Medicaid departments directly with their state plan amendments, waivers, and other demonstration projects – and most recently supported Alaska, Colorado, Delaware, Indiana, Missouri, and Oklahoma.
HMA’s behavioral health team is currently working with multiple Medicaid agencies on the development of substance use disorder (SUD), serious mental illness (SMI), and serious emotional disturbance (SED) specific 1115 waivers.
We pair our behavioral health and Medicaid subject matter experts to support states with:
Developing and applying for SMI/SED and SUD Section 1115 demonstration waivers.
Providing an assessment of the requirements under the Section 1115 demonstration waiver and Medicaid managed care “in lieu of” authorities, including requirements for average length of stay, provider oversight, and monitoring, as well as other considerations.
Reviewing managed care contract requirements and providing applicable Medicaid managed care contract language for states that are utilizing “in lieu of” authority to provide reimbursement for inpatient or residential stays in IMDs.
Technical assistance with developing administrative infrastructure to monitor utilization, including adherence to length of stay requirements under the waiver and “in lieu of” options. CMS’ SMI Section 1115 demonstration waiver guidance prohibits states from receiving Federal Financial Participation (FFP) for any IMD stays that exceed 60 days. In cases where states do not meet this metric, CMS can reduce this maximum length of stay (LOS) to 45 days or less. HMA understands it is important for states to have utilization management (UM) strategies in place to identify these instances and minimize the state’s financial risk, and can therefore provide examples of state UM strategies, as well as incentives to manage inpatient and residential LOS while maintaining access to medically necessary services.
Supporting design of data capture and reporting functions for meeting wavier requirements.
Serving as the independent evaluator for approved SUD and/or SMI/SED 1115 waiver demonstrations.
For more information, contact our featured experts below.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
What does your organization need to know?
March 31st marked the end of the COVID-19 Medicaid continuous coverage condition. Most forecasts project between 10-15 million enrollees will lose Medicaid coverage. State Medicaid programs will lose supplemental funding provided for the continuous coverage requirement and begin to transition to normal eligibility operations. Health Management Associates (HMA) and HMA companies can help the full spectrum of stakeholders plan for, adjust to, and administer the changes up to and beyond the 12-month continuous coverage “unwinding” period. The immediate work can serve as a springboard for future improvement initiatives and to respond to federal guidance that is under development to strengthen and streamline eligibility and enrollment processes and improve the experience for consumers.
Who is affected by this change?
Payers including Medicaid managed care organizations and Qualified Health Plans
Provider organizations
Trade associations of Medicaid managed care or provider organizations
State and local community-based organizations
State and local governments responsible for administering and overseeing the eligibility processes for Medicaid and other public programs
Advocacy groups
Foundations
Vendors supporting state agencies, health plans and providers
Watch a video presentation about the HMA Coverage Model
What is in the HMA model?
HMA has developed an insurance mix model that projects how the resumption of Medicaid eligibility redeterminations beginning in April 2023 will affect Medicaid enrollment, employer sponsored insurance (ESI), Marketplace coverage, and the uninsured. The model includes enrollment projections for all 50 states and considers the enhanced Marketplace subsidies included in the Inflation Reduction Act (IRA). Approximately 20 million individuals gained coverage during the redetermination freeze and well over 10 million of the approximately 90 million current Medicaid enrollees are at risk for disenrollment. HMA’s model contemplates the variety in state approaches to managing the resumption of eligibility redeterminations as well as key insights related to the differential impact by Medicaid eligibility categories.
HMA can help with immediate needs to help you plan:
HMA has detailed state-specific unwinding policy insights for each state including observations regarding which states are taking more aggressive and less aggressive approaches.
We can provide technical assistance and strategic planning services to help states and organizations manage the necessary changes.
Actuarial experts can assist with acuity changes caused by the change in enrollment.
Our colleagues are available for a discussion of the product and the key policies influencing the projections.
HMA can also help with post PHE support.
For more information, please contact our experts below.