Weekly Roundup -
April 22, 2026
Smart. Strategic. Essential.
Unmatched Healthcare Insights from HMA,
Leavitt Partners & Wakely.
Featured:
Medicare’s “Inpatient Only” Rule Is Going Away. Now What?
LISTEN NOW

Trending: In Focus
HMA Resource Provides Key Insights about the Evolving Medicare-Medicaid Integration Landscape
People who are dually eligible for Medicare and Medicaid remain a central focus for policymakers and healthcare organizations, given their complex care needs, disproportionate share of spending, and the long-standing challenge of coordinating coverage across two programs. One of the primary vehicles for advancing integration has been Dual Eligible Special Needs Plans (D-SNPs), which continue to play an increasingly prominent role as federal and state policymakers encourage tighter Medicare-Medicaid alignment.
As states play a more active role in shaping enrollment rules, Medicaid contracting, and procurement strategies, the duals market is becoming more structured and more explicitly guided by state policy decisions. Health Management Associates (HMA’s) 2026 Duals Integration Environmental Inventory, examines how this shift shapes the integration landscape in 2026. This comprehensive inventory is based on a review of the 2026 market, insights from states, and other publicly available resources.
This article examines key trends from HMA’s 2026 inventory and addresses federal policy changes scheduled to take effect for 2027, which contribute to this dynamic environment.
What to Expect in 2026
As the landscape for duals integration evolves, the central question has shifted from whether D-SNPs operate in a state to the more consequential question of how states are using Medicaid policy levers (i.e., enrollment rules, procurement, contracting, and managed care structures) to drive tighter alignment between Medicare and Medicaid.
At the federal level, recent Medicare Advantage and Part D rulemaking is reinforcing that movement. The Contract Year 2025 Medicare Advantage and Part D Final Rule finalized the second phase-down of the D-SNP look-alike threshold to 60 percent for 2026 and established 2027 rules that limit enrollment in certain D-SNPs to members of an affiliated Medicaid managed care organization. The rule also limits the number of D-SNP benefit packages that can be offered alongside an affiliated Medicaid managed care organization. More recently, the Contract Year 2026 Medicare Advantage and Part D Final Rule requires certain D-SNPs to use integrated member ID cards and integrated health risk assessments beginning in 2027.
Together these rules signal a continued federal emphasis on linking D-SNP enrollment and operations more closely to Medicaid coverage and delivery systems, with states playing a greater role in determining how alignment is achieved.
What the 2026 Inventory Shows
HMA’s 2026 Duals Integration Environmental Inventory shows how these policy signals are translating into state action. More specifically:
- Statewide exclusively aligned enrollment appears in 16 states in the 2026 inventory, up from nine in 2025.
- Applicable Integrated Plans (AIPs) are present in 22 states, up from 14, and default enrollment is in place in 21 states, up from 16.
- The inventory also captures 6,084,997 total D-SNP enrollees, including 1,975,250 in Highly Integrated SNPs (HIDE) and 743,683 in Fully Integrated SNPs (FIDE-SNPs).
Those changes are already visible in state markets:
- Illinois, Massachusetts, Ohio, and Rhode Island entered 2026 with a greater FIDE-SNP presence tied to legacy Medicare-Medicaid Plan transitions.
- Michigan launched MI Coordinated Health as a HIDE-SNP in selected regions in 2026, with statewide expansion planned for 2027.
- Delaware also stands out: Although it already had AIPs in the 2025 inventory, it adds statewide exclusively aligned enrollment in 2026 and shows both HIDE-SNPs and coordination-only D-SNPs.
A Resource to Track State Market Direction
HMA’s 2026 Duals Integration Environmental Inventory, available to HMA Information Services (HMAIS) subscribers, includes a state-by-state view of the Medicaid policy, contracting, and program structures shaping duals integration and D-SNP markets. In addition to enrollment trends, the inventory documents the integration model each state is pursuing, whether long-term services and supports or behavioral health are included in managed care, and how procurement and contract decisions may inform future market activity.
HMA experts work with clients to apply this information and deepen their understanding of state integration approaches, inform assessments of their market readiness and alignment opportunities, and develop strategies that support more effective Medicare-Medicaid integration.
Looking Ahead
Notably, HMA’s inventory reflects a point in time understanding of where an individual state is today and what is known at this time about their next steps and plans. However, we expect changes in many states as they seek guidance from the Centers for Medicare & Medicaid Services and the D-SNP community to implement required changes and adopt new regulatory provisions that support state goals and priorities.
The 2026 inventory suggests that more states are using formal alignment tools, that more enrollment is concentrated in integrated products, and that more markets are being shaped by the interaction between Medicaid structure, procurement, and D-SNP strategy.
Connect with Us
For organizations seeking to understand where the market is headed, the Duals Integration Inventory offers a clear view of how state policy and market structure are evolving and where tighter Medicare-Medicaid alignment is taking hold.
Contact Holly Michaels Fisher and Julie Faulhaber to discuss your organization’s questions and needs regarding an integration strategy and market analysis. For information about the HMAIS subscription, access to the Duals Environmental Inventory contact Andrea Maresca and Gabby Palmieri.
Medicaid Managed Care Enrollment: Q4 2025 Trends and Early Signals Ahead of New Eligibility Policies
This week Health Management Associates (HMA), draws on its database of monthly Medicaid managed care enrollment to present its latest quarterly analysis, offering a snapshot of enrollment trends across 37 states.
The analysis comes at a critical time. As states prepare for Medicaid eligibility policy changes that take effect in 2027—including more frequent eligibility determinations and expanded work and community engagement requirements—current enrollment trends provide an early signal of how policy decisions and administrative practices are already influencing coverage levels.
The HMA Information Services (HMAIS) analysis shows that Medicaid managed care accounted for 85.6 percent of total Medicaid enrollment in December 2025. This analysis, available to HMAIS subscribers, uses data from nearly 300 health plans in 41 states. The report provides by-plan enrollment plus corporate ownership, program inclusion, and for-profit versus not-for-profit status, with breakout tabs for publicly traded plans.
Key Insights from Q4 2025 Data
The 37 states included in this review have released monthly Medicaid managed care enrollment data through public websites or in response to a public records request from HMA. The report includes the most recent data obtained and illustrates the effect of state-level choices around eligibility and administration. Key findings include:
- As of December 2025, Medicaid managed care enrollment across the 37 states declined by 2.2 million members year over year, falling to 62.5 million—a 3.4 percent decrease.
- Of the 37 states, eight—Colorado, Delaware, Mississippi, Missouri, New Jersey, North Carolina, North Dakota, and Oregon—did not experience year-over-year managed care enrollment declines, and instead showed flat enrollment or modest gains. With the exception of Mississippi, these are all Medicaid expansion states.
- Arizona and Indiana experienced double-digit percentage declines. Notably, Indiana began requiring enrollees to actively respond to renewal mailers, which aligns with enrollment declines that began in March 2025.
- Among the expansion states in the analysis, enrollment declined by 1.7 million (-3.3%) to 50.8 million. The seven non-expansion states experienced a similar decline (-3.6%), bringing enrollment to 11.7 million enrollees.
Data Considerations. The data have some important limitations. States report enrollment figures at different points during the month, with some data reflecting beginning of the month totals and others capturing end of the month enrollment. In addition, some state datasets encompass all Medicaid programs offering managed care plans, whereas others reflect only a subset of the managed Medicaid population. As a result, the findings should be viewed as indicative of broader trends rather than a comprehensive state-by-state comparison.
Market Share and Plan Dynamics
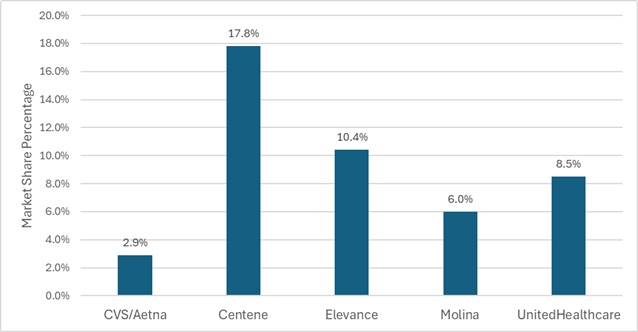
Using our data repository for 300 health plans across 41 states, HMAIS analyzes corporate ownership, program participation, and tax status among Medicaid managed care plans. As of December 2025, Centene maintained the largest share of the national Medicaid managed care market at 17.8 percent, followed by Elevance (10.4%), United (8.5%), and Molina (6.0%) (see Figure 1). These figures highlight continued concentration among large national plans, even as overall enrollment declines.
Figure 1. National Medicaid Managed Care Market Share by Number of Beneficiaries for a Sample of Publicly Traded Plans, December 2025
What to Watch
Enrollment trends observed in the fourth quarter (Q4) of 2025 and continuing into 2026 indicate increasing state attention to eligibility policy and program integrity. State legislative activity, budget pressures, and federal regulatory developments are prompting many states to assess and strengthen certain aspects of their programs related to eligibility, particularly as they prepare to implement redetermination and work and community engagement requirements.
Several states are already moving toward implementation. Nebraska is scheduled to launch Medicaid work requirements on May 1, 2026, while Montana plans to begin implementation on July 1, 2026. With additional federal guidance still emerging, most other states are working toward compliance ahead of January 2027 deadlines. In expansion states, policymakers retain authority to tighten administrative processes, alter optional benefits, or adjust provider payment levels—actions that may materially affect enrollment.
These developments underscore why Medicaid managed care enrollment trends deserve close attention. Declines in enrollment are often an early indicator of broader system impacts, including rising uncompensated care for providers, shifts in payer mix, and increased financial pressure on safety‑net systems. For managed care organizations, even modest enrollment changes can mask more significant shifts in risk profiles, geographic concentration, or service needs.
Connect with Us
HMA is home to experts who know the Medicaid managed care landscape and how it is evolving. HMAIS’s Medicaid enrollment data, financials, procurement tracking, and a robust library of public documents equips stakeholders with timely, actionable intelligence.
For more information about the HMAIS subscription, contact Andrea Maresca and Alona Nenko.
CMS Proposes Modest Hospital Payment Updates and Signals Expanded Use of Mandatory Value-Based Models
On April 10, 2026, the Centers for Medicare & Medicaid Services (CMS) released the proposed rule for the Fiscal Year 2027 Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System (LTCH PPS). The proposal combines a modest net increase in hospital payments with policy signals around quality reporting and mandatory episode-based payment models—most notably a proposed nationwide expansion of the Comprehensive Care for Joint Replacement (CJR) model.
These proposed updates underscore CMS’s continued emphasis on value-based purchasing, episode accountability, and alignment across quality programs. In addition, CMS resurfaces ongoing debates with hospital stakeholders about the adequacy of Medicare payment updates amid rising costs and coverage disruptions.
This article reviews several key provisions in the FY 2027 proposed rule.
Hospital Payment Updates: Headline Increase Masks Net Impact
Under the proposed rule, CMS would increase base IPPS and LTCH PPS payment rates by 2.4 percent in FY 2027. However, after accounting for proposed reductions to uncompensated care payments for disproportionate share hospitals (DSH) and changes in outlier payments for extraordinarily high-cost cases, CMS estimates the effective payment increase would be closer to 1.2 percent.
In aggregate, CMS projects the proposed update would translate to approximately $1.4 billion in additional payments to acute care hospitals next year. Hospital industry groups—including the American Hospital Association (AHA) and the Federation of American Hospitals (FAH)—have pushed back, arguing that the proposed update does not sufficiently reflect medical inflation, workforce pressures, or anticipated growth in the uninsured population.
These concerns reflect a long-standing dynamic in annual hospital payment rules: CMS seeking to balance statutory updates and budget neutrality constraints against the hospital industry’s concern that Medicare payments are lagging behind underlying costs.
Quality Reporting and Program Alignment
The proposed rule would also make notable updates to the Hospital Inpatient Quality Reporting (IQR) Program. CMS proposes adding three new quality measures to be phased in during 2029 and 2030, while modifying eight existing measures to include Medicare Advantage patients. CMS also proposes shortening the performance period for certain measures from three years to two—a change designed to accelerate feedback and better align measures across programs.
These changes continue CMS’s broader effort to harmonize quality measurement across Medicare payment and value-based programs, reduce reporting lag, and incorporate a more comprehensive view of patient populations.
Updates to Mandatory TEAM Model
CMS also proposes several updates to the Transforming Episode Accountability Model (TEAM), the mandatory episode-based payment model finalized last year. Key proposals include:
- Expanding the list of MS-DRGs included in the spinal fusion episode
- Aligning TEAM quality measurement performance periods with the IQR Program
- Making targeted technical refinements to payment methodology
In addition, CMS is seeking stakeholder feedback on whether ambulatory surgery centers (ASCs) should participate in TEAM and whether participation should be voluntary for physician-owned hospitals, signaling potential future expansion or recalibration of the model.
Proposed Expansion of Joint Replacement Bundles
CMS proposes to expand the existing Comprehensive Care for Joint Replacement Expanded (CJR-X) Model nationwide beginning October 1, 2027. The agency also plans to make participation mandatory for most IPPS hospitals.
CMS tested the original CJR model in 34 metropolitan areas between 2016 and 2024, generating improved patient outcomes and net Medicare savings, according to agency evaluations. CJR-X would become the fifth Center for Medicare and Medicaid Innovation model to meet the statutory criteria for nationwide expansion.
Under CJR-X, hospitals performing lower extremity joint replacements would be accountable for the cost and quality of care for the initial procedure and most related spending during the subsequent 90 days. Although the overall structure mirrors the original CJR model, CMS proposes several important updates:
- Expansion of episodes to include ankle replacements, in addition to hip and knee procedures
- Adoption of a more robust risk adjustment methodology with significantly more variables, aligning closely with the TEAM model
- Introduction of a 5 percent stop-loss policy for hospitals that serve higher proportions of dually eligible beneficiaries and certain smaller hospitals
Participation would be mandatory for most IPPS hospitals, with exceptions for hospitals already participating in TEAM, which includes a lower extremity joint replacement episode; Maryland hospitals operating under global budgets; and hospitals not paid under both IPPS and the Outpatient Prospective Payment System, such as Critical Access Hospitals.
Why It Matters
The 2027 IPPS and LTCH PPS proposed rule reinforces several clear policy signals:
- Pressure on hospital margins is likely to persist, as payment updates continue to trail hospital-reported cost growth.
- Mandatory episode-based models remain central to CMS’s value-based strategy, with CJR-X representing a significant escalation in scope and scale.
- Program alignment and MA inclusion are accelerating, with implications for hospital data systems, care coordination strategies, and reporting infrastructure.
Hospitals and health systems will need to assess not only the near-term financial impact of the proposed payment updates, but also their readiness to accept expanded episode accountability and meet evolving quality measurement requirements.
Comments on the proposed rule will shape final decisions regarding payment levels, quality program changes, and the scope of mandatory participation in CJR-X. Stakeholders will be watching closely to see whether CMS moderates its approach to mandatory models or doubles down on episode-based accountability as a cornerstone of Medicare payment reform.
In parallel, CMS has released several other proposed payment rules this month, including those that would affect skilled nursing facilities, hospice providers, inpatient rehabilitation facilities, and inpatient psychiatric facilities. For these entities, CMS generally proposes payment updates of approximately 2.4 percent and 2.3 percent for inpatient psychiatric facilities. As part of its broader program integrity focus, CMS also has proposed new transparency measures for hospice providers; this follows recent enforcement actions related to fraudulent enrollment.
Connect with Us
Health Management Associates, Inc. (HMA), monitors federal regulatory and legislative developments in the inpatient setting and assesses the impact on hospitals, life science companies, and other stakeholders. Our experts interpret and model hospital payment policies and assist clients in developing CMS comment letters and long-term strategic plans. Our team replicates CMS payment methodologies and model alternative policies using the most recent Medicare fee-for-service and Medicare Advantage (100%) claims data. We also support clients with DRG reassignment requests, New Technology Add-on Payment (NTAP) applications, and analyses of Innovation Center alternative payment models.
For more information about the proposed policies, contact one of our Medicare experts.
Federal Policy News
Fueled By Leavitt Partners Weekly Health Intelligence
Leadership Shift at HHS Signals New Direction for Public Health and Affordability
A number of recent announcements signaled further leadership changes at the US Department of Health and Human Services (HHS), notable among them President Trump’s announcement on April 16 through a Truth Social post that he is nominating Erica Schwartz, MD, JD, MPH, to serve as the new Centers for Disease Control and Prevention (CDC) Director. The agency has been without a confirmed director since Dr. Susan Monarez’s departure in August 2025, with former HHS Deputy Secretary Jim O’Neill followed by NIH Director Dr. Jay Bhattacharya temporarily leading the agency since then. Dr. Schwartz is a retired Rear Admiral in the U.S. Public Health Service Commissioned Corps and served as Deputy US Surgeon General from January 2019 to April 2021, during President Trump’s first term and at the height of the COVID-19 pandemic. HHS Secretary Robert F. Kennedy, Jr. also expressed his support for the nomination last week.
Further, Dr. Schwartz’s nomination has been largely positively received by public health leaders, including the American Public Health Association and Dr. Jerome Adams, a former US Surgeon General, who has been a vocal critic of the current Trump Administration’s changes to public health policy.
Dr. Schwartz’s nomination will be considered by the Senate HELP Committee.
In the post announcing Dr. Schwartz’s nomination, President Trump also announced the appointment of Mr. Sean Slovenski, a healthcare executive, as CDC Deputy Director and Chief Operating Officer; Dr. Jennifer Shuford, the Commissioner of the Texas Department of State Health Services, as CDC Deputy Director and Chief Medical Officer; and Dr. Sara Brenner, the Principal Deputy Commissioner of FDA as Senior Counselor for Public Health to Secretary Kennedy.
Further, on April 17, Secretary Kennedy announced that economist Casey B. Mulligan, PhD, will serve as the Chief Economist and Chief Regulatory Officer of HHS. Dr. Mulligan previously served as Chief Economist on the Council of Economic Advisers during the first Trump Administration and the Chief Counsel for Advocacy at the US Small Business Administration. In the press release announcing the appointment, HHS states that “his portfolio will include cost-benefit analysis of regulation, econometric modeling, and program evaluation of major expenditures,” with a focus on making healthcare more affordable.
The personnel changes at HHS likely reflect a waning interest among White House personnel to place MAHA-affiliated leaders in senior departmental positions, particularly as the nomination of Casey Means to be Surgeon General has stalled and the midterm elections approach. The personnel announcements are instead intended to reflect a disciplined message from the Administration and a focus on healthcare affordability.
Executive Order Advances Psychedelic Therapy Research
On April 18, President Trump issued an Executive Order (EO), titled, “Accelerating Medical Treatments for Serious Mental Illness.” The EO discusses the prevalence and severity of serious mental illness in the United States, particularly among U.S. veterans, as well as suicide rates. The EO notes the complex nature of treating these conditions, including that they are often resistant to treatment, and goes on to discuss the potential use of psychedelic drugs to treat these conditions, “for patients whose conditions persist after completing standard therapy.” As such, the EO:
- Directs FDA to “provide Commissioner’s National Priority Vouchers to appropriate psychedelic drugs that have received a Breakthrough Therapy designation and are in accordance with the criteria of the National Priority Voucher Program.” The CNPV provides faster review times and increased communication with the agency for sponsors of drug and biologics applications that support administration priorities.
- Directs FDA to establish a pathway for eligible patients to access psychedelic drugs consistent with the Right to Try Act.
- Directs HHS through ARPA-H to allocate $50 million in existing funds to a federal and state government collaboration focused on supporting states that have “enacted or are developing programs to advance psychedelic drugs for serious mental illnesses” through technical assistance and data sharing. In the Fact Sheet detailing the EO provisions, it is stated that this funding should be used to “to match investments made by state governments.”
- Directs HHS, FDA, and the VA to collaborate to “increase clinical trial participation, data sharing, and real-world evidence generation” regarding the use of psychedelic drugs. Specifically, the EO directs the agencies to enter data-sharing agreements such that FDA may access relevant data that would ultimately support drug approvals.
- Directs the Attorney General to “initiate and complete review of any product containing a Schedule I substance that has successfully completed Phase 3 clinical trials for a serious mental health disorder,” to ensure timely rescheduling of the drug if appropriate.
FDA Steps Up Efforts to Close Gaps in Clinical Trial Reporting
On April 13, the US Food and Drug Administration (FDA) announced that it sent messages to more than 2,200 medical product companies and researchers to remined them of requirements to disclose certain clinical trial results information to ClinicalTrials.gov. The Food and Drug Administration Amendments Act of 2007, section 801 and subsequent Final Rule on Clinical Trials Registration and Results Information Submission requires sponsors to register and submit summary results within one year after completing a clinical trial of an FDA-regulated drug, biological product, or medical device regardless of whether or not the results are favorable.
On March 30, the agency contacted sponsors and researchers associated with more than 3,000 registered clinical trials that do not appear to have submitted required results information or potentially incomplete actions related to the National Library of Medicine’s quality control review process. FDA stated that, of those studies highly likely to be subject to such requirements, an internal estimate of 29.6 percent of studies do not have results data submitted to ClinicalTrials.gov. The messages seek voluntary compliance and represent an “extra step” the agency is taking before considering further action, which may include Pre-Notices of Noncompliance and Notices of Noncompliance. FDA framed the initiative as a means of reducing publication bias, improving patient safety, and better informing clinicians and researchers about the benefits and risks of medical products.
HHS Budget Hearings Continue; House Advances Healthcare Bills
After appearing before three House committees last week, HHS Secretary Robert F. Kennedy, Jr. returns to the Hill this week to testify on the fiscal year (FY) 2027 HHS budget request. This past week he testified before the House Ways and Means Committee, Education and Workforce Committee, and Appropriations Subcommittee on Labor, Health and Human Services, Education, and Related Agencies, where members asked questions related to the Administrations expenditure of FY 2026 funding, and the proposed budget for FY 2027. Several committee members reiterated concerns regarding the Administration’s policy changes related to vaccines, biomedical research, and HHS staffing, while Republican Committee members and some Democrats applauded actions related to addressing the prevalence of artificial food dyes and microplastics in the environment. Secretary Kennedy highlighted recent action taken by the Administration to advance the MAHA agenda, while previewing future action including reforming the U.S. Preventive Services Task Force.
Further, this week, the House considering the following healthcare legislation under suspension of the rules:
- H.R. 2319, the Women and Lung Cancer Research and Preventive Services Act of 2025, which requires the Secretary of HHS, in consultation with the Secretaries of Defense and Veterans Affairs, to conduct an interagency review and make recommendations on opportunities related to accelerating research related to lung cancer in women and underserved populations, access to lung cancer screenings for those populations, and lung cancer public awareness and education campaigns.
- H.R. 2493, the Improving Care in Rural America Reauthorization Act of 2025, which would reauthorize certain rural health grants and update uses of funds for rural underserved populations. The bill extends the following programs at currently authorized levels of $79.5 million for each of fiscal years 2026 through 2030:
- Rural Health Care Services Outreach Grants;
- Rural Health Network Development Grants; and
- Small Health Care Provider Quality Improvement Grants.
- H.R. 3419, the Telehealth Network and Telehealth Resource Centers Grant Program Reauthorization Act, which would reauthorize the grant programs at $42 million for each of fiscal years 2026 through 2030.
Each of these bills was reported out of the House Energy and Commerce Committee with unanimous support and are expected to easily pass in the House. Two of the bills, the Improving Care in Rural America Reauthorization Act and the Women and Lung Cancer Research and Preventive Services Act, have companion legislation introduced in the Senate that have been reported out of the Senate HELP Committee.
Ready to talk about your organization's challenges?
Schedule a Consultation
State Policy News
Hawaii Awards AlohaCare Medicaid Behavioral CCS Contract
Hawaii’s Department of Human Services, Med-QUEST Division, announced on April 8, 2026, that it awarded AlohaCare a competitive contract to operate the Community Care Services (CCS) program, which provides comprehensive behavioral health services integrated with physical health services to Medicaid-enrolled adults with serious mental illness or serious and persistent mental illness. The program is delivered statewide and is intended to provide the full range of required behavioral health services under the request for proposals. The contract carries a total value of $180 million, with a contract period running from July 1, 2026, through June 30, 2029. The incumbent is Centene/Ohana Health Plan.
Kentucky Launches Medicaid Reentry Coverage for Individuals Leaving Incarceration
The Kentucky Lantern reported on April 16, 2026, that it is implementing a federal 1115 reentry demonstration that will provide eligible people leaving incarceration with Medicaid coverage for 12 months and a one-month supply of prescribed medications upon release. The program allows pre-release screenings beginning 60 days before scheduled release and is intended to support reentry, reduce recidivism and overdose deaths, and improve access to care. While the demonstration was approved in 2024, state officials said implementation took time because it required coordination across agencies, eligibility systems, and correctional facilities.
Michigan Awards Healthy Kids Dental Contract to Delta Dental
The Michigan Department of Health and Human Services (MDHHS) announced on April 17, 2026, that it is awarding the Healthy Kids Dental contract to incumbent Delta Dental. The program serves approximately 955,000 children under the age of 21, and covers services such as X-rays, cleanings, fillings, extractions, and sealants. The new contract will begin October 1, 2026, and run through September 30, 2031, with up to three one-year extension options.
Minnesota Warns $3.1 Billion in Federal Medicaid Funding Remains at Risk
Minnesota Department of Human Services announced on April 16, 2026, that state officials warned that despite federal approval of the state’s corrective action plan, up to $3.1 billion in Medicaid funding remains at risk as the Centers for Medicare & Medicaid Services continues to defer and withhold payments. State officials said the ongoing funding restrictions could destabilize healthcare providers and local economies, particularly in rural areas. The state is appealing the federal actions while continuing to implement fraud prevention measures, including provider revalidation, enhanced payment review, provider dis-enrollments, and other program integrity initiatives.
Pennsylvania Court Rules Medicaid Abortion Ban Unconstitutional
WGAL reported on April 20, 2026, that the Pennsylvania Commonwealth Court declared that the state’s ban on Medicaid-covered abortions is unconstitutional in a 4-3 ruling. The judges determined that the state constitution includes the fundamental right to reproductive autonomy, rendering the ban unconstitutional.
Virginia Seeks to Develop Medicaid Maternal Health Desert Mobile Clinic Pilot Program
The Virginia Department of Medical Assistance Services (DMAS) released on April 17, 2026, a request for information (RFI) on the development and implementation of a Maternal Health Desert Mobile Clinic Pilot Program, which would expand access to prenatal and postpartum care for Medicaid and CHIP members in underserved areas. DMAS is seeking information regarding organizational experience, service delivery models, geographic coverage, partnerships, outreach, data collection, and reporting practices from organizations with expertise in mobile health service delivery, maternal health, and care coordination. Responses are due May 1, 2026.

Private Market News
Fueled By Wakely Consulting Group
California Judge Tosses Elevance’s Surprise Billing Suit
A California federal judge dismissed an Elevance Health lawsuit accusing HaloMD and providers of abusing the No Surprises Act’s dispute process, ruling the insurer failed to prove wrongdoing. The decision is a win for providers and may limit insurers’ ability to challenge payment disputes in court, though Elevance plans to appeal.
Medicare Navigation Company Chapter Secures New Round of Funding
Studies Examine General Purpose Chatbots
Two new studies highlight significant limitations in general-purpose artificial intelligence chatbots used for health–related questions. One study finds that, across 21 off-the-shelf large language models and 29 standardized clinical vignettes, differential-diagnosis failure rates exceeded 80 percent for every model. The findings suggest general-purpose chatbots remain unreliable for initial diagnostic reasoning, even if performance improves once additional clinical information is provided. Another study finds that 50 percent of responses from five publicly available chatbots to evidence–based health questions were somewhat or highly problematic, with especially weak performance on open-ended prompts. The findings reinforce ongoing concerns about consumers relying on off-the-shelf chatbots for medical advice without clinician oversight.
Our Insights
Fueled By Experts Across Our HMA Companies
Health Management Associates
Saving Lives with Compassion: Overdose Response Training with RiVive®
This webinar will present findings from the 2025 RiVive Community Engagement Report and best practices in Compassionate Overdose Response™, with a focus on the community use of RiVive naloxone nasal spray 3 mg. A panel of expert speakers will present their protocols for effective overdose intervention, guidance on the training of others, and strategies for integrating trauma-informed approaches into post-overdose care. Designed for program teams, medical professionals, and harm reduction leaders, anyone who attends will leave with research and experience-backed methods for improving outcomes in opioid overdose emergencies. A recording of this webinar will be available after this session, with a link to the 2025 report.
2026 Michigan State of Reform Health Policy Conference | May 5, 2026
The 2026 Michigan State of Reform Health Policy Conference will be taking place in-person on May 5th, 2026 at the Kellogg Hotel and Conference Center! Managing constant change in healthcare takes more than just hard work. It takes a solid understanding of the legislative process and knowledge about intricacies of the healthcare system. That’s where State of Reform comes in.
2026 Maryland State of Reform Health Policy Conference | May 21, 2026
The 2026 Maryland State of Reform Health Policy Conference will be taking place in-person on May 21st, 2026 at the Baltimore Marriott Waterfront! Managing constant change in healthcare takes more than just hard work. It takes a solid understanding of the legislative process and knowledge about intricacies of the healthcare system. That’s where State of Reform comes in.
RFP Calendar
RFP Calendar
| Date | State/Program | Event | Beneficiaries |
|---|---|---|---|
| Date: February 2026 - DELAYED | State/Program: Illinois | Event: Awards | Beneficiaries: 2,400,000 |
| Date: May 1, 2026 | State/Program: Nevada Children's Specialty | Event: Proposals Due | Beneficiaries: NA |
| Date: May 12, 2026 | State/Program: Nevada CO D-SNP | Event: Awards | Beneficiaries: 88,000 |
| Date: June 24, 2026 | State/Program: Wisconsin LTC GSR 3 | Event: Awards | Beneficiaries: 56,000 (all GSR) |
| Date: Summer 2026 | State/Program: Illinois Foster Care | Event: RFP Release | Beneficiaries: 33,000 |
| Date: July 1, 2026 | State/Program: Hawaii Community Care Services | Event: Implementation | Beneficiaries: 5,500 |
| Date: July 28, 2026 | State/Program: Nevada Children's Specialty | Event: Awards | Beneficiaries: NA |
| Date: August 2026 | State/Program: Indiana | Event: RFP Release | Beneficiaries: 1,400,000 |
| Date: January 1, 2027 | State/Program: Illinois | Event: Implementation | Beneficiaries: 2,400,000 |
| Date: January 1, 2027 | State/Program: Nevada CO D-SNP | Event: Implementation | Beneficiaries: 88,000 |
| Date: January 1, 2027 | State/Program: Wisconsin LTC GSR 3 | Event: Implementation | Beneficiaries: 56,000 (all GSR) |
| Date: January 1, 2027 | State/Program: Illinois Tailored Care Management Program | Event: Implementation | Beneficiaries: 22,400 |
| Date: July 1, 2027 | State/Program: Nevada Children's Specialty | Event: Implementation | Beneficiaries: NA |
| Date: January 1, 2028 | State/Program: Wisconsin LTC GSR 4,6 | Event: Implementation | Beneficiaries: 56,000 (all GSR) |
| Date: Fall 2027 | State/Program: Oregon | Event: RFP Release | Beneficiaries: 1,200,000 |
| Date: 2028 | State/Program: North Carolina | Event: RFP Release | Beneficiaries: 2,200,000 |
| Date: 2029 | State/Program: California | Event: RFP Release | Beneficiaries: NA |