HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
CMS, through CMMI, has multiple new models focusing on value based care, continuing to push the envelope towards improving care through their programs. In this webinar, experts examined how organizations are able to seize opportunities through operationalizing these models and what it means for safety net providers, health systems, and community-based organizations. The discussion focused on practical insights, emerging challenges, and strategic opportunities to drive impact and sustainability under new models.
Learning Objectives:
Understand recent and emerging CMMI models, including its policy intent, structure, and implications for Medicare beneficiaries and safety net providers
Examine and gain insights from organizations implementing CMMI aligned models of care, including care model design, infrastructure, and partnerships
Identify strategic opportunities for health systems, ACOs, and community-based providers to maximize impact and sustainability
Featured Speakers:
Royal Tuthill, SVP of Networks Pair Team
Lance Donkerbrook, ACO Executive Director P3 Health Partners
These proposed updates underscore CMS’s continued emphasis on value-based purchasing, episode accountability, and alignment across quality programs. In addition, CMS resurfaces ongoing debates with hospital stakeholders about the adequacy of Medicare payment updates amid rising costs and coverage disruptions.
This article reviews several key provisions in the FY 2027 proposed rule.
Hospital Payment Updates: Headline Increase Masks Net Impact
Under the proposed rule, CMS would increase base IPPS and LTCH PPS payment rates by 2.4 percent in FY 2027. However, after accounting for proposed reductions to uncompensated care payments for disproportionate share hospitals (DSH) and changes in outlier payments for extraordinarily high-cost cases, CMS estimates the effective payment increase would be closer to 1.2 percent.
In aggregate, CMS projects the proposed update would translate to approximately $1.4 billion in additional payments to acute care hospitals next year. Hospital industry groups—including the American Hospital Association (AHA) and the Federation of American Hospitals (FAH)—have pushed back, arguing that the proposed update does not sufficiently reflect medical inflation, workforce pressures, or anticipated growth in the uninsured population.
These concerns reflect a long-standing dynamic in annual hospital payment rules: CMS seeking to balance statutory updates and budget neutrality constraints against the hospital industry’s concern that Medicare payments are lagging behind underlying costs.
Quality Reporting and Program Alignment
The proposed rule would also make notable updates to the Hospital Inpatient Quality Reporting (IQR) Program. CMS proposes adding three new quality measures to be phased in during 2029 and 2030, while modifying eight existing measures to include Medicare Advantage patients. CMS also proposes shortening the performance period for certain measures from three years to two—a change designed to accelerate feedback and better align measures across programs.
These changes continue CMS’s broader effort to harmonize quality measurement across Medicare payment and value-based programs, reduce reporting lag, and incorporate a more comprehensive view of patient populations.
Updates to Mandatory TEAM Model
CMS also proposes several updates to the Transforming Episode Accountability Model (TEAM), the mandatory episode-based payment model finalized last year. Key proposals include:
Expanding the list of MS-DRGs included in the spinal fusion episode
Aligning TEAM quality measurement performance periods with the IQR Program
Making targeted technical refinements to payment methodology
In addition, CMS is seeking stakeholder feedback on whether ambulatory surgery centers (ASCs) should participate in TEAM and whether participation should be voluntary for physician-owned hospitals, signaling potential future expansion or recalibration of the model.
Proposed Expansion of Joint Replacement Bundles
CMS proposes to expand the existing Comprehensive Care for Joint Replacement Expanded (CJR-X) Model nationwide beginning October 1, 2027. The agency also plans to make participation mandatory for most IPPS hospitals.
CMS tested the original CJR model in 34 metropolitan areas between 2016 and 2024, generating improved patient outcomes and net Medicare savings, according to agency evaluations. CJR-X would become the fifth Center for Medicare and Medicaid Innovation model to meet the statutory criteria for nationwide expansion.
Under CJR-X, hospitals performing lower extremity joint replacements would be accountable for the cost and quality of care for the initial procedure and most related spending during the subsequent 90 days. Although the overall structure mirrors the original CJR model, CMS proposes several important updates:
Expansion of episodes to include ankle replacements, in addition to hip and knee procedures
Adoption of a more robust risk adjustment methodology with significantly more variables, aligning closely with the TEAM model
Introduction of a 5 percent stop-loss policy for hospitals that serve higher proportions of dually eligible beneficiaries and certain smaller hospitals
Participation would be mandatory for most IPPS hospitals, with exceptions for hospitals already participating in TEAM, which includes a lower extremity joint replacement episode; Maryland hospitals operating under global budgets; and hospitals not paid under both IPPS and the Outpatient Prospective Payment System, such as Critical Access Hospitals.
Why It Matters
The 2027 IPPS and LTCH PPS proposed rule reinforces several clear policy signals:
Pressure on hospital margins is likely to persist, as payment updates continue to trail hospital-reported cost growth.
Mandatory episode-based models remain central to CMS’s value-based strategy, with CJR-X representing a significant escalation in scope and scale.
Program alignment and MA inclusion are accelerating, with implications for hospital data systems, care coordination strategies, and reporting infrastructure.
Hospitals and health systems will need to assess not only the near-term financial impact of the proposed payment updates, but also their readiness to accept expanded episode accountability and meet evolving quality measurement requirements.
Comments on the proposed rule will shape final decisions regarding payment levels, quality program changes, and the scope of mandatory participation in CJR-X. Stakeholders will be watching closely to see whether CMS moderates its approach to mandatory models or doubles down on episode-based accountability as a cornerstone of Medicare payment reform.
In parallel, CMS has released several other proposed payment rules this month, including those that would affect skilled nursing facilities, hospice providers, inpatient rehabilitation facilities, and inpatient psychiatric facilities. For these entities, CMS generally proposes payment updates of approximately 2.4 percent and 2.3 percent for inpatient psychiatric facilities. As part of its broader program integrity focus, CMS also has proposed new transparency measures for hospice providers; this follows recent enforcement actions related to fraudulent enrollment.
Connect with Us
Health Management Associates, Inc. (HMA), monitors federal regulatory and legislative developments in the inpatient setting and assesses the impact on hospitals, life science companies, and other stakeholders. Our experts interpret and model hospital payment policies and assist clients in developing CMS comment letters and long-term strategic plans. Our team replicates CMS payment methodologies and model alternative policies using the most recent Medicare fee-for-service and Medicare Advantage (100%) claims data. We also support clients with DRG reassignment requests, New Technology Add-on Payment (NTAP) applications, and analyses of Innovation Center alternative payment models.
For more information about the proposed policies, contact one of our Medicare experts.
The Long‑term Enhanced Accountable Care Organization (LEAD) Model represents the next major step in the Centers for Medicare & Medicaid Services (CMS) accountable care strategy and reinforces a federal commitment to value-based participation in Traditional Medicare. Announced as the successor to ACO REACH, LEAD is a voluntary, nationwide, 10‑year model that will operate from 2027 to 2036, making it the longest-running accountable care organization (ACO) model the Center for Medicare and Medicaid Innovation has tested.
Momentum around the LEAD ACO model has accelerated since CMS’s recent release of the Request for Applications (RFA), which formally moves LEAD from policy design to implementation. The RFA requires prospective participants to evaluate program design choices, financial implications, and operational readiness on a compressed timeline. Notably, CMS has indicated that additional opportunities to express interest will follow for organizations that are not prepared to apply for participation in the initial cohort.
This article explains key design elements of the LEAD model and identifies considerations for organizations assessing whether and when to pursue participation in LEAD.
Core Design Evolutions of the LEAD Model
While LEAD builds on many of the elements from ACO REACH, its design reflects how the Innovation Center intends to address challenges with previous ACO models, such as the Medicare Shared Savings Program (MSSP). At its core, LEAD seeks to establish a pathway to long‑term engagement in value-based care that creates an attractive option for all types of providers, including ACOs with a history of engaging in value-based care and providers that have yet to meaningfully participate.
LEAD introduces a set of targeted design changes intended to improve predictability, alignment accuracy, and long‑term participation in accountable care—most notably through revised benchmarking, updated beneficiary alignment, and expanded flexibility for engaging specialists and high‑needs populations.
1. Revising Benchmarking Policies to Support Predictability and Success
LEAD provides a major win for ACOs seeking long-term predictability bysetting a long-term benchmark that will not rebase for the entirety of the 10-year model. In MSSP, many ACOs eventually face the “ratchet effect” in which benchmarks erode after rebasing to reflect the ACO’s more recent spending patterns. It can create a significant hurdle for ACOs that have already successfully reduced spending, as their own prior success lowers their benchmark. By not rebasing for the entirety of the model period, LEAD provides an attractive alternative to the MSSP, which rebases every five years.
LEAD will also support historically successful ACOs by transitioning to a fully regional rate book by the end of the model period. As a result, benchmarks will be set based on overall spending in the region where an ACO operates rather than an ACO’s historical spending. While ACO REACH also used a regional rate book to inform some ACO benchmarks, LEAD goes further by seeking to transition all ACOs to a benchmark based fully on a regional rate book while also adding protections for higher-spending ACOs by transitioning regions at different timelines to ensure that newer ACOs have the opportunity to implement the kinds of care delivery changes that lead to lower spending before they are subject to penalties.
Other notable changes to benchmarking include a variety of ACO-specific adjustments and the addition of an administrative component to benchmarking. ACOs will be eligible to receive a boost to their benchmarks with either a regional efficiency adjustment for ACOs with lower spending or a prior savings adjustment for ACOs with a demonstrated history of achieving savings. LEAD also introduces an administratively set component to benchmarking—the Accountable Care Prospective Trend—which already is used in the MSSP, though LEAD adds a new guardrail policy to promote predictability.
2. Improving Accuracy in Beneficiary Alignment
LEAD’s new “hybrid” alignment option increases accuracy and responsiveness. Monthly additions of voluntarily aligned beneficiaries and mid-year recognition of new participant taxpayer identification numbers (TINs) adopted after the start of the performance year (PY) allow alignment to better reflect real-time care relationships, averting lag and operational friction.
3. Adding Support for High-Needs Beneficiaries
LEAD expands support for beneficiaries with complex needs through a universal High Needs category and recalibrated risk adjustment. By moving away from ACO REACH’s population‑exclusive model, LEAD lowers barriers for organizations that serve a disproportionate share of high‑needs and dually eligible populations. In addition, CMS will test Medicare‑Medicaid alignment in two states, and help states develop arrangements supporting the provision of value-based care between ACOs and state Medicaid agencies or managed care organizations.
4. Promoting Deeper Engagement with Specialists
LEAD increases flexibility for engaging specialists in value‑based arrangements. New Non‑Primary Care Capitation options and episode-based risk arrangements (CMS‑Administered Risk Arrangements (CARAs)), allow ACOs to share risk with specialists without Total Care Capitation, reducing operational complexity while expanding accountability beyond primary care.
5. Advancing Technology Adoption and Innovation
LEAD introduces structured pathways to promote technology adoption. Planned Artificial Intelligence (AI)‑inferred risk adjustment will be phased in following successful testing and validation, while the Tech Enabler Initiative and Rapid Cycle Innovation Program seek to reduce administrative burden and accelerate evidence generation—particularly for smaller or resource‑constrained ACOs.
Next Steps
The Innovation Center is operating on an accelerated timeline for the initial LEAD cohort. Prospective ACOs have fewer than 50 days to digest a detailed Request for Applications and model potential performance. Applications are due May 17, 2026. ACOs that participated in ACO REACH in PY 2026 will be well-positioned, as many of the provisions in LEAD will be familiar, and the agency is permitting this group of ACOs to submit an abbreviated application for participation.
For organizations not ready to apply for the first cohort, CMS will release a standardized Letter of Interest form by April 17, 2026, to gauge interest in future application rounds. In this context, organizations considering LEAD participation should be assessing not only near‑term application readiness, but also longer‑term strategic alignment with the model’s 10‑year commitment, risk structure, and operational requirements. Key considerations include benchmarking predictability, readiness to manage regional benchmarks, capacity to engage specialists and high‑needs beneficiaries, technology capabilities, and alignment with broader value‑based care strategies across Medicare and Medicaid.
Connect with Us
Health Management Associates (HMA), supports organizations across the LEAD decision continuum, including those pursuing immediate application and those preparing for future cohorts. HMA can help organizations:
Interpret LEAD’s policy and financial design relative to existing ACO and MSSP participation
Model performance scenarios under alternative benchmark, alignment, and risk configurations
Assess operational readiness across care management, contracting, analytics, and compliance
Develop application strategies and supporting materials, including responses to the LEAD RFA
Choose to defer application on steps that preserve future optionality
As CMS advances LEAD under an ambitious timeline, early analysis and disciplined decision‑making will be critical for organizations seeking to align participation with their long‑term value‑based care strategies.
The Medicare Advantage (MA) program continues to evolve as plans respond to shifting policy signals, market pressures, and beneficiary expectations. A new paper from Wakely, an HMA Company—The Value Shift: How Medicare Advantage Benefits Are Evolving for 2026—provides a data-driven examination of how MA benefit designs are changing and what those changes signal about the future direction of the program.
This paper refreshes Wakely’s ongoing MA benefit analysis, updating prior findings with the latest 2026 plan enrollment data. It builds on Wakely’s established work examining benefit design, supplemental offerings, and the relationship between bids, rebates, and plan value, including The Value Shift: Inside the C-SNP Surge.
This article highlights findings from the proprietary value-add metric that Wakely developed to provide a comprehensive assessment of MA plan value. Although it can be used as a comparative metric to evaluate relative changes year over year, it is not intended to represent pricing.
From Benefit Expansion to Optimization
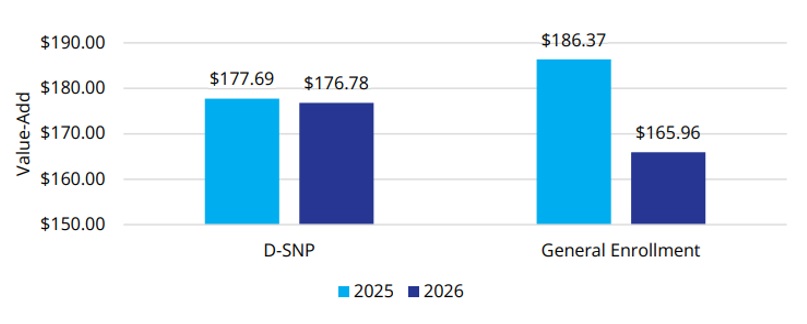
Over the past decade, MA plans have steadily expanded benefit offerings, supported by strong enrollment growth and favorable rebate dynamics. The 2026 benefit landscape suggests that plans have been taking a more measured approach (see Figure 1). Wakely’s analysis finds that plans are becoming more strategic in how benefits are designed and deployed, maintaining or enhancing benefits that are best aligned with quality performance, affordability, and target populations while pulling back in other areas.
Plans appear to be optimizing benefits to better align with member needs, quality performance, and financial parameters. Examples include refining supplemental benefits, adjusting cost-sharing structures, and rethinking how benefits support care management and health outcomes.
Figure 1. Change in Plan Value-Add from 2025 to 2026
The shift reflects an MA market in which differentiation and long-term sustainability are increasingly important.
Supplemental Benefits: More Targeted, More Strategic
Supplemental benefits remain a defining feature of Medicare Advantage, but their role is evolving. Wakely’s paper highlights a move away from expanding the number of benefits toward targeted benefit offerings that are more clearly connected to member engagement and outcomes.
Plans are homing their focus on benefits that support daily living, chronic condition management, and access to care, particularly for populations with higher needs. This targeted approach suggests plans are thinking about value, operational complexity, and how benefits contribute to overall value propositions.
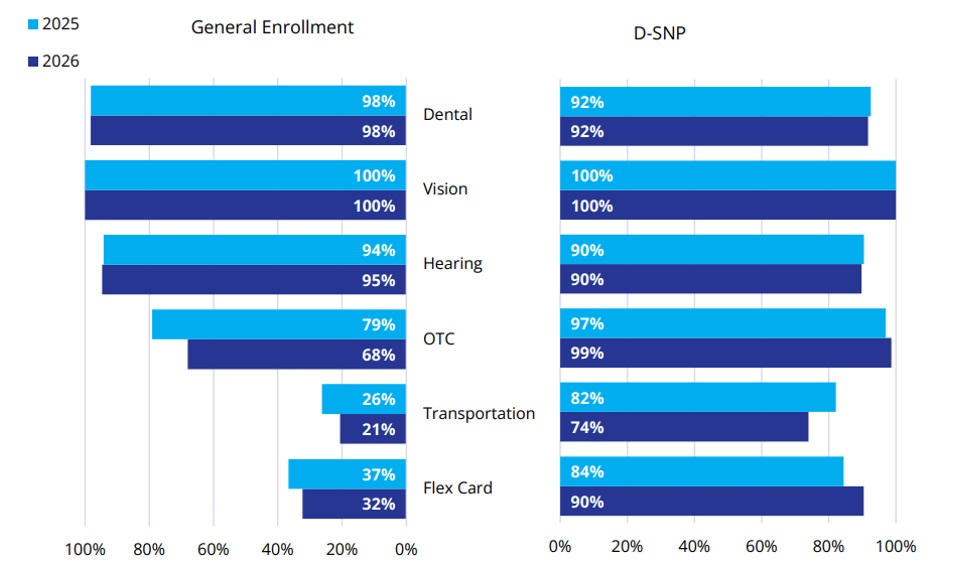
Between 2025 and 2026, the percentage of members with access to common supplemental benefits has, on average, stayed consistent or slightly decreased among the general enrollment population (Figure 2). The percentage of members who are enrolled in plans that offer over-the-counter (OTC) drug, transportation, and Flex Card benefits has decreased by 11 percent, 6 percent, and 4 percent, respectively. Conversely, the Dual Eligible Special Needs Plan (D-SNP) population saw an increase in member access to all supplemental benefit categories except transportation (an 8% decrease).
Figure 2. Percent of Enrollment in Common Supplemental Benefits
For stakeholders across the healthcare ecosystem, this trend underscores the importance of understanding not just what benefits are offered, but why.
Shifts in Cost Sharing and the Enrollee Experience
Wakely’s analysis also points to notable shifts in cost sharing and premium structures. There is continued attention to balancing affordability for members with the need to manage plan liability amid changing benchmarks and utilization patterns.
These decisions directly affect the member experience. Small shifts in copays, deductibles, or benefit limits can influence enrollment, retention, and satisfaction, particularly in competitive markets. As plans fine tune these levers, data-driven insights become critical to understanding how benefit changes may resonate with different member segments.
2026 Signals for Future Bid Cycles
The benefit trends identified in “The Value Shift” series suggest several broader signals for the MA market:
Value over volume: Plans are prioritizing benefits that support quality, outcomes, and sustainable growth.
Greater segmentation: Benefit designs are increasingly tailored to specific populations and market dynamics.
Data-informed decision-making: As margins tighten, plans are relying more heavily on analytics to guide benefit strategy.
Special needs plans continue to drive growth. Enrollment in Chronic Condition Special Needs Plans (C-SNPs) is the fastest-growing segment in MA.
These dynamics have implications for MA organizations and for providers, policymakers, and partners seeking to understand how MA continues to shape care delivery and costs.
Value-Add Metric and Benefit Design Insights
In this paper, Wakely paired its actuarial and analytic expertise with tools that enable detailed benefit and market analysis. One of those tools, Wakely’s Medicare Advantage Competitive Analysis Tool (WMACAT), calculates a comprehensive value-add metric that integrates five core components into a consistent framework that allows for apples-to-apples comparisons across plans, markets, and years. In addition, Wakely’s Strategic Market Analysis and Ranking Tool (SMART) supports broader competitive assessments by layering enrollment weighting, geographic variation, and plan positioning into the analysis.
As an HMA company, Wakely’s work is complemented by broader policy, market, and strategy expertise, helping organizations connect benefit decisions to regulatory developments, operational considerations, and long-term goals.
For health plans and healthcare organizations navigating the next phase of Medicare Advantage, these combined capabilities can respond to questions such as:
How competitive is our benefit design today, and where are the risks?
Which benefits are most aligned with our population and quality strategy?
How might future policy or payment changes affect benefit sustainability?
Looking Ahead
MA benefit design remains an important signal of market direction by showing how plans are responding to policy change, market competition, and financial pressure. As plans shift from broad expansion to more targeted value strategies, the ability to measure, compare, and interpret benefit changes becomes essential as plans look ahead to the 2027 and 2028 bid cycles.
Wakely will continue to build on this work with upcoming analyses, including deeper dives into Part D design changes and the implications of the sunset of the Value-Based Insurance Design (VBID) program.
HMA and Wakely Share Expert Insights on VBC Landscape
In this webinar, experts from HMA and Wakely reviewed the nation’s progress in the movement to value-based payment models and looked ahead to its next chapter, sharing HMA’s views on future expectations for CMMI’s model portfolio, how shifting market and policy dynamics may impact MA contracting, and the state of value-based enablers, health systems, other risk-bearing provider entities impacted by these forces. HMA’s VBC Advisory Services team supports organizations with integrated insights across strategy, analytics, and implementation to drive measurable results in value-based care.
Learning Objectives:
Review the current state of APM adoption and key trends
Explore the CMS Innovation Center’s recent activities and potential focus areas for future models
Understand policy and market headwinds facing Medicare Advantage plans with implications for VBC
Gain insights into participation trends among health systems, enablers, and states
Hospitals and health systems are under growing pressure to succeed in new value-based models that demand both operational transformation and strategic alignment. In this webinar, advisors from Health Management Associates, Wakely, an HMA Company and Nixon Peabody broke down the latest regulatory and contractual developments, explored lessons learned from the Comprehensive Care for Joint Replacement (CJR) model, and discussed how organizations can prepare for upcoming opportunities.
Speakers shared practical insights on:
The regulatory, operational, and actuarial considerations hospitals must navigate
Key takeaways from bundled payment initiatives like CJR
How to leverage data and design strategies to build partnerships that position organizations for success in new Medicare models
This session was designed for hospital executives, provider organizations, payers, and policy leaders seeking to better understand how emerging value-based models will shape the future of care delivery and payment.
On May 13, 2025, the Centers for Medicare & Medicaid Services (CMS) published its new strategic direction for the CMS Innovation Center. The strategy builds on the lessons of the first 15 years of the Innovation Center, while presenting a significant pivot in policy direction, which emphasizes evidence-based prevention, consumer engagement, and tech-enabled care, while prioritizing financial performance over broad participation.
The new strategy provides high-level direction on the Trump Administration’s vision for the next phase of value-based payment reform under the leadership of CMS Administrator Dr. Mehmet Oz and Innovation Center Director Abe Sutton. They intend to “double down on our commitment to value-based care and take the learnings from the[se] previous investments to build a health system that empowers people to drive and achieve their health goals and Make America Healthy Again.” Notably, the strategy also aligns with goals central to the Trump Administration’s Make America Healthy Again initiative.
This new direction affirms the administration’s commitment to continue advancing value-based care and opens additional opportunities for organizations seeking to enhance the delivery of services that drive positive outcomes. Health Management Associates (HMA), experts will be tracking the implementation of the Innovation Center’s new strategy, including expected forthcoming models, movement toward greater levels of downside risk, and changes to existing models to align with the administration’s priorities. In this article, our experts review the strategy and provide insights on key takeaways for stakeholders.
New Strategy Overview
CMS leaders view the Innovation Center agenda as a framework for accelerating healthy behaviors, leveraging the agency’s authority to test new approaches designed to incentivize and engage stakeholders. According to CMS officials, the Innovation Center “will work expeditiously toward the future of health—building a system in which people are empowered to achieve their health goals and providers are incentivized to compete to deliver high-quality, efficient care and improve the health outcomes of their patients.”
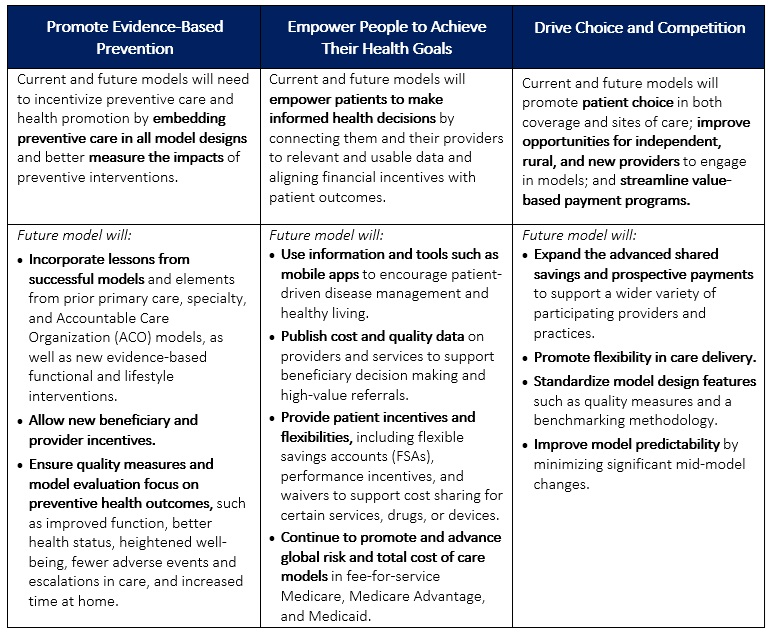
The strategy has three interrelated, foundational pillars:
Promoting evidence-based prevention
Empowering people to achieve their health goals
Driving choice and competition.
Table 1 provides more detail on each pillar.
In addition to the new agenda, CMS released a request for information (RFI) seeking industry input on strategies that can better leverage data and technology to empower consumers. The focus of the RFI aligns with the Innovation Center’s strategic pillars to use tools, information, and processes that better connect people to their health data and allow them to make informed health decisions alongside their providers.
Table 1. CMMI’s Interrelated Strategic Pillars
Takeaways and Considerations
Critical to CMS’s approach is the belief that empowering individuals to make their health decisions—through incentives, better data access, and more flexible options—can lead to better health outcomes and lower overall costs. This shift reflects an evolution in healthcare policy that places greater emphasis on personal accountability and private sector collaboration—a key theme that is emerging across the administration’s policy initiatives.
Consumer Engagement. One of the most notable aspects of the new Innovation Center strategy is the promotion of consumer engagement; it places more focus on direct consumer engagement through education and incentives compared with earlier initiatives. This is one area in which the Innovation Center plans to collaborate with the private sector to develop consumer-facing tools (e.g., mobile apps, nudges toward healthy behaviors, etc.).
The focus on consumer engagement also presents opportunities for organizations to enhance their customer experience. By understanding the needs and preferences of their patients, organizations can tailor their services and care models to better meet those demands. This personalized approach not only improves patient satisfaction, but also drives continuity of care, ultimately contributing to long-term improvements in health.
Data and Technology. The new strategy also emphasizes the importance of data, indicating intentions to better equip organizations that participate in the model with data that can inform decisions and optimize their processes. CMS officials are examining policies and collaborations that will empower private sector organizations, including model participants, researchers, and technology vendors, to develop innovative data-driven solutions to drive efficiencies and improved health.
To that end, the May 16, 2025, Request for Information (RFI) from CMS and the Assistant Secretary for Technology Policy/Office of the National Coordinator for Health (ASTP/ONC), Health Technology Ecosystem (CMS-0042-NC), focuses on Medicare beneficiaries’ use of technology to improve health outcomes. The RFI, which HMA experts analyze here [insert bookmark or link to the other In Focus article] underscores the administration’s intentions of taking “bold steps to modernize the nation’s digital health ecosystem.”
Medicare Advantage. The Innovation Center’s new strategy indicates that stakeholders should expect more models that address Medicare Advantage (MA). The agency stated that “features of a model could include testing changes to payment for MA plans, such as testing the impact of inferred risk scores, regional benchmarks, or changes to quality measures that better align with promoting health.” Additionally, the strategy references a forthcoming specialty-focused longitudinal care model within MA and Medicaid, signaling intentions to drive multi-payer alignment.
Saving Federal Tax Dollars. Another major aspect of the strategy is “protecting federal taxpayers.” This goal reflects a continued emphasis on total cost of care accountability and indicates a more aggressive shift to downside risk. The Innovation Center says it will “require all models to have downside financial risk and require providers to assume some of the financial risk..” Additional provisions of protecting tax dollars include reducing role of state governments in rate setting, simplifying model benchmark methodology, and ensuring “proper and nondiscriminatory provision of funds for health care services.”
What to Watch
For healthcare organizations, the Innovation Center’s agenda signals a need to prioritize consumer-centric models. Hospitals, providers, and insurers should anticipate the following:
Increased focus on preventive care initiatives to align with new model designs
More robust data-sharing and technology requirements, meaning investments in patient-focused digital tools will become essential
New opportunities in MA, given potential payment model innovations affecting plan structures and risk-adjusted reimbursement
Healthcare stakeholders should monitor possible developments related to the strategy.
While details on specific strategies have yet to emerge, the Innovation Center indicated it plans to provide more information on new models, as well as changes to existing models, in the coming months.
The Innovation Center has not provided a goal akin to the previous administration’s effort to have 100 percent of Medicare beneficiaries in accountable care relationships by 2030. It is still unknown whether these goals are forthcoming or if this will remain vague.
Stakeholders are still awaiting clarity on changes to existing models, including key models set to conclude at the end of 2026 (i.e., ACO REACH and Kidney Care Choices).
Strategy language indicates that the agency may develop payment innovation in prescription drugs, medical devices, and technology.
Connect With Us
The Health Management Associates Annual Conference, Adapting for Success in a Changing Healthcare Landscape, October 14-16, 2025, in New Orleans, LA, will feature discussions on how the new strategy is reshaping the healthcare system and care delivery for patients, particularly the opportunities to revisit provider contracts with MA plans and to integrate technology to advance the prevention of chronic conditions and achieve population health goals.
For more information about the opportunities and considerations the Innovation Center agenda presents for your organization, contact HMA’s featured experts below.
Digital Quality Measurement: A Key Driver to Value
The healthcare industry is on the cusp of a seismic shift in how quality data are collected, analyzed and reported. Beginning in January 2027, new federal interoperability and prior authorization rules will require widespread data exchange, paving the way for full digital quality measurement (dQM) by 2030. This move toward dQM presents enormous opportunity to enhance quality outcomes, strengthen value-based arrangements, and streamline operations. However, it also requires substantial strategic, operational, and technological changes that most organizations simply cannot manage alone.
Regulatory Mandates
Organizations that delay preparing for the 2027 rule risk costly setbacks and non-compliance.
Opportunity for Transformation
dQM drives efficiency and quality improvement, supporting population health initiatives, care coordination, and value-based contracting.
Complexity and Risk
dQM implementation spans multiple departments—IT, quality improvement, analytics, legal, and more—creating a host of challenges requiring specialized expertise.
Competitive Advantage
Early adopters will have a first mover advantage. This advantage could result in revenue associated with auto-assignment, STARS bonus, value-based purchasing, reduced sanctions and fine, etc.
Why Partner with HMA?
HMA’s dQM consulting team understands the operational, clinical, and technical dimensions of transitioning to digital quality measurement. Leveraging deep expertise across health plans, provider organizations, and state and federal agencies, we help you plan, implement, and evaluate your dQM strategies at every stage.
1. Speed to Solution
Front-Seat Knowledge: HMA, together with Leavitt Partners, an HMA Company, is actively influencing and shaping national conversations on interoperability and digital measures. Our front-line insights mean you gain rapid access to the latest best practices, regulatory updates, and strategic guidance.
Streamlined Roadmap & Implementation: We help you develop a clear, achievable plan of action—saving you from the pitfalls of trial-and-error by fast-tracking your implementation and monitoring the results.
2. Cross-Department Coordination
Complexity of Transformation: dQM requires alignment across IT, quality, clinical operations, and finance—often a monumental undertaking for organizations already at capacity. Robust change management & strategic planning and communications is crucial for success.
Meet Mandated Timelines: Waiting to act can result in financial risk, stressed operations, and missed opportunities to optimize reimbursement.
Manage Risk: Because digital quality measurement is in an emerging phase, organizations face higher levels of uncertainty. HMA mitigates risk by leveraging our extensive experience and industry partnerships.
3. Proven Expertise and Ongoing Support
Full Project Lifecycle: From early planning and strategy development through implementation and evaluation, we stand by you every step of the way.
Value Beyond Compliance: Our team identifies how dQM can drive broader business goals—improving population health, care coordination, and value-based contracting performance..
Ready to Transform Your Quality Measurement?
HMA’s expert consultants provide the advanced technical, business, and operational skills you need to succeed in today’s rapidly evolving regulatory landscape. Don’t let the complexity of dQM derail your strategic plans or burden your teams. With HMA as your partner, you can confidently navigate and optimize your transition to digital quality measurement.
Take the first step toward harnessing the power of digital quality measurement. Partner with HMA to position your organization for success today—and well into the future.
Contact our HMA dQM experts to discuss your organization’s goals and challenges:
Jennifer Bridgeforth, associate principal at Health Management Associates, dives into the complexities of fraud, waste, and abuse in healthcare, examining the blurred lines between inefficient processes and intentional misconduct. The conversation explores how value-based care, provider education, and technology could pave the way for more efficient and patient-centered healthcare. Listen to discover insights on navigating these challenges in a shifting healthcare landscape.
The Centers for Medicare & Medicaid Services (CMS) announced on December 16, 2024, that it will be terminating the Medicare Advantage Value-Based Insurance Design (VBID) model at the end of 2025 because of the model’s “substantial and unmitigable costs to the Medicare Trust Funds.” This In Focus article delves into the factors driving CMS’s decision and considerations for policymakers, Medicare Advantage Organizations and other interested stakeholders.
VBID Outcomes
VBID, run by the CMS Innovation Center, is not a permanent part of the Medicare Advantage (MA) program. Innovation Center models are required to be modified or terminated if they are a cost to the program.
CMS found that costs for the VBID model totaled $2.3 billion in calendar year (CY) 2021 and $2.2 billion in CY 2022, an unprecedent amount for an Innovation Center model. CMS concluded that these substantial expenses—driven by increased risk score growth and Part D expenditures—were unmitigable through policy modifications. Therefore, consistent with statutory requirements, CMS took action to terminate the model by the end of 2025. Earlier this year, CMS announced it would discontinue the part of VBID that allowed MA plans to offer hospice services.
Next year, the VBID model will have 62 participating MA plans and is projected to offer 7 million Medicare beneficiaries additional benefits and/or rewards, including those designed to address social determinants of health and reduce cost-sharing for prescription drugs used to treat and manage chronic conditions. As part of the announcement, CMS pledged to support a stable transition for all enrollees in MA plans participating in the MA-VBID model and emphasized that key benefits available under the model will continue to be widely available, including supplemental benefits that address the whole-person healthcare needs of beneficiaries. In addition, CMS noted beneficiary cost-sharing for prescription drugs will be reduced as the result of the expansion of the low-income subsidy program under the Inflation Reduction Act and the CMS Innovation Center’s Medicare $2 Drug List Model, which is slated to begin in 2027.
As part of the announcement, CMS released an executive summary of a forthcoming evaluation report, with the full report expected to be released in early 2025.
Key Considerations
Since the MA-VBID model’s launch in 2017, the program has experienced significant growth through a series of legislative and model changes, including requirements in the Bipartisan Budget Act of 2018 that expanded eligibility to MA plans in all 50 states and allowing all types of MA special needs plans to participate in MA-VBID. Previous CMS evaluations found that the MA-VBID model led to improvements in the quality of care for beneficiaries and promoted greater adherence to prescription drugs used to treat and manage chronic conditions. Though CMS has concluded that excess costs require the termination of MA-VBID by the end of 2025, the incoming Trump Administration can be expected to closely examine this decision and look at the entire Innovation Center portfolio.
Connect with Us
Health Management Associates, Inc. (HMA), Medicare experts will continue to assess and analyze the response to CMS’s announcement, including the incoming administration’s views on the decision and potential alternatives. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist MA organizations and interested stakeholders in analyzing and adapting to the marketplace as the MA-VBID program ends.
For further analysis of the MA-VBID decision and its impact on the market, contact our experts below.
HMA is hosting its 2024 Fall Conference October 7−9 in Chicago, IL. Unlocking Solutions in Medicaid, Medicare, and Marketplace Programs promises to enhance your ability to navigate and shape healthcare programs and systems, focusing on improving health and well-being.
In a landscape dominated by endless video meetings, the HMA Fall Conference offers a refreshing change. Join us for an enriching experience featuring:
Engagement with healthcare experts and thought leaders who are actively collaborating with stakeholders
Participation in face-to-face discussions to exchange ideas and receive valuable feedback
Opportunities to connect with peers who are committed to strengthening public programs and enhancing health outcomes
Keynote Address and Sessions
Darshak Sanghavi, MD, from the Advanced Research Projects Agency for Health (ARPA-H), will deliver the Keynote Address. He and other speakers will inspire attendees to explore innovative healthcare programs and their potential impacts on healthcare delivery, reimbursement, and health outcomes.
The conference will feature a diverse array of speakers and participants, including C-suite executives from national, regional, and local health plans. Federal and state leaders joining panels will include:
State Medicaid directors from New York, Iowa, New Mexico and Alabama
State insurance commissioners
Behavioral health agency officials
State housing agencies
Leaders from the US Interagency Council on Homelessness
The conference will include a revamped pre-conference workshop on October 7, featuring hands-on exercises and interactive sessions led by HMA leaders. Sessions will include a value-based care contracting exercise, a value-based purchasing assessment discussion for providers, tips and tricks on navigating Medicaid section 1115 demonstrations, AI applications in healthcare, and more.
Early bird registration is open until July 31. Don’t miss this opportunity to gain actionable knowledge, forge valuable connections, and discover fresh insights and best practices. Register now to secure your spot at the forefront of healthcare innovation.
Innovation is the source of progress, driving advancements across industries and shaping the way we live, work, and interact. However, the landscape of innovation is not static—it ebbs and flows, influenced by various factors including political leadership. This year’s presidential election may bring forth significant shifts in priorities, policies, and funding that directly impact innovation efforts like Center for Medicare & Medicaid Innovation (CMMI), state waivers and the Advanced Research Projects Agency for Health (ARPA-H).
CMMI serves as a catalyst for testing innovative payment and service delivery models within Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). With a new administration comes the potential for shifts in CMMI’s focus and funding priorities. For instance, a president (or his/her appointees) can direct CMMI to design payment models, reimbursement structures that can lead to higher quality outcomes and more cost-effective healthcare delivery. The policy priorities and values that undergird a president’s healthcare agenda can shape the kinds of innovation that CMMI drives. Current CMMI initiatives have prioritized value-based care approaches linking payment to outcomes, improving equity of care across race, gender, and geography, and patient-centered care models designed to support particularly high cost, complex conditions; the priorities of the previous administration included focus on substance abuse disorders, kidney disease, and diabetes.
CMS also grants waivers to states, such as Section 1115 waivers for Medicaid or 1332 waivers for insurance marketplaces, that offer flexibility to experiment with innovative healthcare solutions. The values and policy approaches of a new president will influence the degree of regulatory flexibility and the types of experimentation that will be approved. For example, several states have recently received approval on Medicaid waivers that encourage community-based approaches to whole person care, wrapping together healthcare coverage, benefits, delivery, with new support services that address upstream barriers to health.
ARPA-H, a new unit within the National Institutes of Health focuses on investments in “break-through technologies and broadly applicable platforms, capabilities, resources, and solutions that have the potential to transform important areas of medicine and health for the benefit of all patients,” holds immense potential for driving breakthroughs in healthcare by funding innovation that “cannot readily be accomplished through traditional research or commercial activity.” The types of projects funded by ARPA-H could be directly impacted by the policy and budget priorities of whomever is president in 2025 and their interest in promoting collaboration between government, academia, and industry to address complex health challenges. A prime example of a potentially impacted area is the emphasis on cancer research by the Biden Administration. This focus may shift drastically with a change in leadership.
For healthcare innovators looking to stay informed and adaptable amidst these potential policy changes, HMA has two opportunities of interest: The HMA Fall conference, and a DC Direct subscription. On October 7-9, healthcare leaders and HMA experts will gather for the 2024 Fall Conference: Unlocking Solutions in Medicaid, Medicare and Marketplace, focused on innovation in public programs. Our keynote speaker Darshak Sanghavi, MD is, a foundational leader at ARPA-H tasked with developing health programs that challenge how we think about healthcare innovation inside and outside government. Conference registration is now open – register today.
Leavitt Partners (LP), an HMA Company, guides clients who need to more closely track federal policy and regulatory activity and know when and how to influence the process. DC Direct, an exclusive offering from LP, provides timely information and insights to elevate your knowledge from simply scratching the surface of understanding to becoming part of the fabric of change.