
Survey data from fiscal year (FY) 2022 suggest that entities that provide ground ambulance services in the State of New York are experiencing reimbursement challenges. Health Management Associates, Inc. (HMA), contracted with the United New York Ambulance Network (UNYAN) to conduct an independent study of the costs of delivering ground ambulance services in the state and the adequacy of payment for these critical services. The HMA-UNYAN survey data highlight the wide variation in costs within the ground ambulance industry in New York and the negative Medicaid margins the industry experiences. These data demonstrate that although ambulance entities of all sizes in New York have negative Medicaid margins, these margins worsen as entity size decreases and entities become more rural. Trends in negative margins appear to be linked to some degree to entities’ relative share of “responses without transport” or uncompensated transports. This white paper poses important considerations for policymakers.
342 Results found.

Outlook 2026: Rural Health Transformation Program
As we kick off the new year, Health Management Associates (HMA) is launching a new series of brief, insightful interviews with our policy experts on issues that will define 2026—what’s changing, why it matters, and how federal, state, and industry decisions will shape what happens next. Building on our earlier analysis of the Rural Health Transformation Program ((RHTP), here and here), this week, we start with a pointed look at the Centers for Medicare & Medicaid Services’s (CMS) first year of RHTP awards.
Rural Health, Ready or Not: CMS Wants Results in 2026
An interview with Kathleen Nolan, Senior Advisor, HMA, and Sara Singleton, Principal, Leavitt Partners, an HMA Company.
Q: What do the new Rural Health Transformation Program awards tell us about US Department of Health and Human Services (HHS) and CMS priorities heading into 2026?
Kathleen Nolan: One of the clearest signals is that CMS expects visible progress in 2026. This is not a program that gives states months of planning runway. The application made it clear that CMS wants states to start doing the activities they proposed right away—not just planning or propping up existing systems. CMS wants to see meaningful movement on implementation in 2026, especially in the areas of workforce, infrastructure, technology modernization, and care delivery redesign.
Sara Singleton: Exactly, and CMS is using this investment to reinforce some of the administration’s broader policy goals. Many state proposals leaned heavily into chronic disease prevention, chronic care management, and expanding supports that promote healthier lifestyles. That alignment isn’t accidental. The Administration is looking for real traction on these priorities, and RHTP gives states both the resources and the accountability framework to make progress. So, the message from CMS is clear: Move quickly, implement strategically, and show early gains in the areas that matter for long-term population health.
Q: Was anything in the awards themselves surprising?
Singleton: There was a lot of speculation about how wide the spread in funding levels might be, particularly for states’ discretionary initiatives. But the distribution was relatively tight; 32 states fell in the “average” range of $190‒$230 million, with only four states above $230 million and 13 below $190 million. That suggests CMS isn’t signaling dramatic differences in expected performance or ambition.
Nolan: It reinforces that CMS is looking for consistent, measurable progress from every state. States that struggle to implement their plans could see less funding in about years.
Q: What should states keep top of mind heading into year one?
Nolan: Accountability. CMS has made it clear they will adjust budgets in later years if states don’t meet expectations on reporting and evaluation. That also means states need to know where the dollars are going and what they are getting for the investment. Year one performance really matters.
Singleton: And it’s not just CMS. Congress and the Office of Inspector General for HHS will also be watching how states use these funds.
Q: What rural health policy developments are you watching in early 2026?
Nolan: Decisions about the leadership for these initiatives and state legislatures. Federal investment can only go so far. States will need strong leaders and supportive policies to accelerate and sustain RHTP efforts in year one. What legislatures choose to prioritize will shape the impact of RHTP far beyond year one.
Tracking Medicaid’s Growth: FFY 2025 Spending and T-MSIS Data Provide Insights on Managed Care Spending
This week, our In Focus section highlights findings from a Health Management Associates Information Services (HMAIS) analysis of the Centers for Medicare & Medicaid Services (CMS) preliminary CMS-64 Medicaid expenditure report for federal fiscal year (FFY) 2025. The data show total medical services expenditures reached $971.4 billion across all states and territories, up 6.9 percent from FFY 2024.
This CMS-64 spending detail provides important context as states prepare for their upcoming legislative sessions and begin implementing changes required under the 2025 budget reconciliation act (P.L. 119-21, OBBBA). Early fiscal and operational pressures will stem from changes to the Supplemental Nutrition Assistance Program (SNAP) and preparations for community engagement requirements for Affordable Care Act (ACA) Medicaid expansion enrollees. In subsequent years, pressures will intensify because of major changes to provider tax financing and new federal limits on state directed payments in 2027 and early 2028.
In this article, we provide a deeper review of Medicaid spending, including the federal-state financing split. As Medicaid agencies prepare for upcoming spring sessions and anticipate potential program changes under OBBBA, it is notable that nearly two-thirds of Medicaid directors report an at least fifty percent likelihood of a Medicaid budget shortfall in FFY 2026.
Growth and Drivers in Medicaid Managed Care Spending
The HMAIS analysis looks at CMS-64 preliminary estimates of Medicaid spending by state for FFY 2025. CMS tracks state expenditures through the automated Medicaid Budget and Expenditure System/State Children’s Health Insurance Budget and Expenditure System (MBES/CBES).
While enrollment decreased for most states following the COVID-19 public health emergency unwinding, states saw an uptick in expenditures due to increased state directed payments, greater utilization and sicker populations, higher drug costs, increased provider rates, and greater use of long-term services and supports and behavioral health.
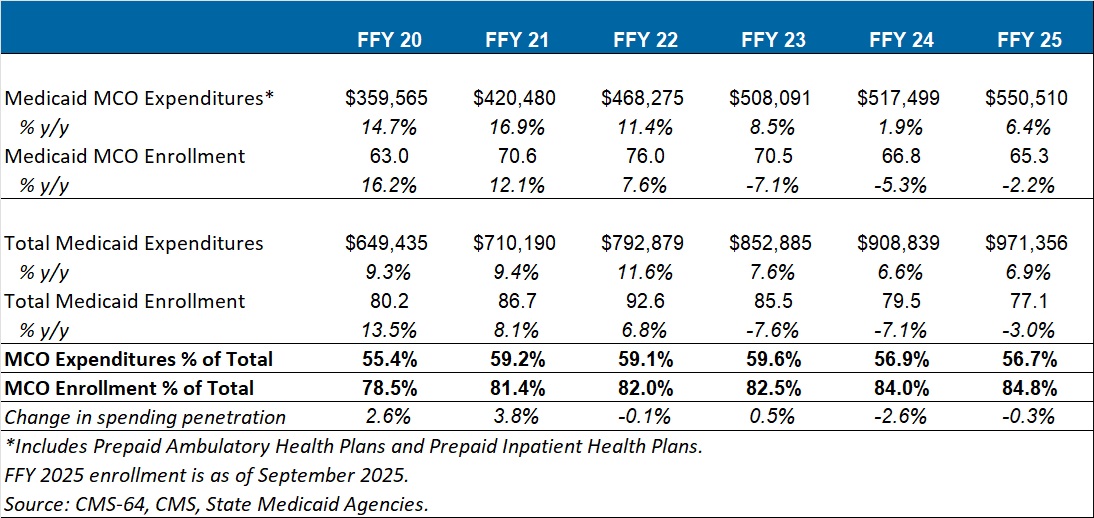
Key findings from HMAIS’ analysis (see Table 1), include:
- Total Medicaid managed care spending (federal and state share combined) reached $550.5 billion in FFY 2025, up from $517.5 billion in FFY 2024.
- This amount represents a 6.4 percent year-over-year increase from FFY 2024 to FFY 2025.
- Managed care accounted for 56.7 percent of total Medicaid spending in FFY 2025, down 0.3 percentage points from the previous year.
- The $33 billion increase from FFY 2024 to FFY 2025 exceeds the $9.4 billion increase seen the year prior, reflecting renewed growth following the unwinding transition period.
These figures include spending on comprehensive risk-based managed care organizations (MCOs), prepaid inpatient health plans (PIHPs), and prepaid ambulatory health plans (PAHPs). PIHPs and PAHPs refer to prepaid health plans that provide a subset of services, such as dental or behavioral health care. This total is exclusive of fee-based programs such as primary care case management models.
Table 1. Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures, FFY 2020–2025 (in millions)
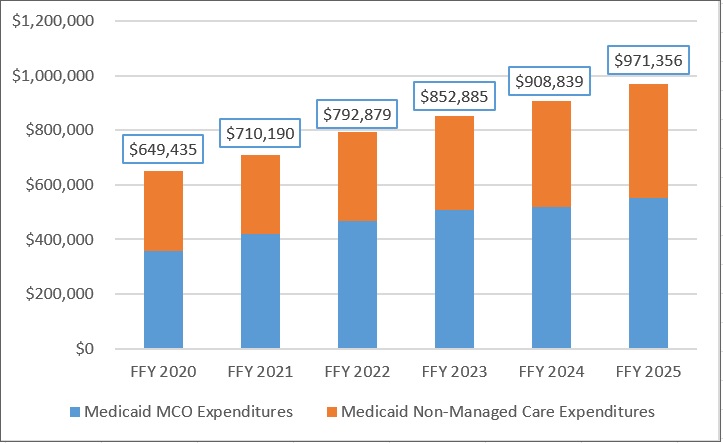
Annual Medicaid managed care expenditures have grown consistently with total Medicaid expenditures. After slower growth in FFY 2024—which aligned with the post-COVID-19 policy unwinding period when many states completed eligibility redeterminations—FFY 2025 again experienced an uptick in managed care growth (see Figure 1).
Figure 1. Total and MCO Medicaid Expenditures, FFY 2020–2025 ($M)
Federal versus State Share Spending
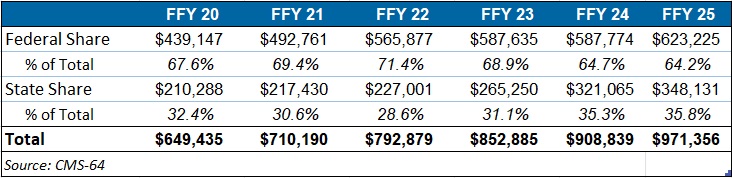
The preliminary FFY 2025 expenditure data provides a baseline before OBBBA’s changes are scheduled for implementation and as states continue to face Medicaid funding challenges. In FFY 2025, federal funding accounted for 64.2 percent of FFY 2025 spending, and non-federal matching funds accounted for 35.8 percent (see Table 2). Particularly later in 2027, 2028, and subsequent years, Medicaid expansion states stand to see disproportionally larger increases in their share of spending.
Table 2. Federal versus State Share of Medicaid Expenditures, FFY 2020–2025 (in millions)
T-MSIS Data Adds Detail to CMS-64 MCO Spending
To complement CMS-64 macro-spending trends, HMA developed a methodology allowing us to use Transformed Medicaid Statistical Information System (T-MSIS) data to approximate managed care spending by service category. Although T-MSIS enables more granular views (e.g., professional services, inpatient/outpatient hospital services, skilled nursing facilities (SNFs), HCBS, clinics, pharmaceuticals), the most recent dataset typically lags one to two years behind CMS-64 totals.
HMA’s analysis of the T-MSIS data shows that while managed care remains the dominant delivery system model for Medicaid, spending by provider types helps contextualize the CMS-64 report. Notably, the CMS-64 reports FFY25 data and our report below on T-MSIS disaggregation uses 2023 data. Although the T-MSIS and CMS-64 data are for different years, it still highlights the main components of the largest spending component of the CMS-64 with more recent data.
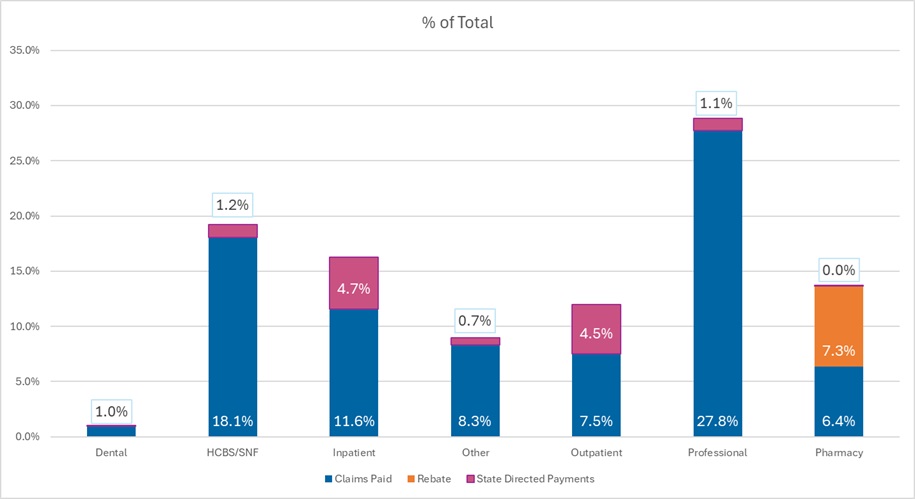
The 2023 T-MSIS analysis shows the following:
- Professional fees are the lead spending category, with nearly 30 percent of spending directed toward payments to physicians and other practitioners (e.g., physician assistants, nurse practitioners). Given that T-MSIS data are built around billing codes, services that traditionally may be considered part of a bundled rate (i.e., a large portion of physician services delivered in hospitals and clinics) are essentially unbundled and considered professional fees.
- Hospital spending (inpatient plus outpatient), SNF costs, and professional fees together account for close to 75 percent of spending in CY 2023.
Figure 2. T-MSIS Medicaid Spending by Service Category 2023 (MCO disaggregated plus FFS)
What to Watch
Because Medicaid is such a big part of state government spending, outlays for Medicaid will always be a focus and challenge for states. Upcoming state legislative sessions and OBBBA driven changes will begin in 2026 with SNAP pressures and major operational preparations for community engagement requirements for expansion states. Preparations for new limits on provider taxes and state directed payments will likely begin immediately, but the true impacts will occur in 2027 and early 2028. States will need to tailor their programs under funding constraints.
Connect with Us
HMAIS, a subscription-based tool that Health Management Associates offers, provides state-by-state analysis of the CMS-64 data, Medicaid managed care enrollment trends, and state budget reporting. For more information about an HMAIS subscription, contact Andrea Maresca and Alona Nenko. For details on T-MSIS data, contact Matt Powers and Shreyas Ramani.
Executive Branch Actions Target Drug Affordability in New Pricing Models
The federal drug pricing landscape continues to undergo significant transformation as executive branch agencies advance an ambitious suite of regulatory and model testing initiatives intended to lower the costs associated with the Medicare and Medicaid programs. In response to ongoing concerns about rising out-of-pocket costs, increasing pressure to align US prices with those paid internationally, and the continued implementation of the Inflation Reduction Act (IRA), federal agencies are reshaping how prescription drugs are priced, reimbursed, and negotiated in federally financed programs.
The current policy environment reflects a growing emphasis on benchmarking drug prices to those in peer nations, referred to as “most favored nation” (MFN) benchmarks, and accelerating actions that require or encourage manufacturers to offer lower net prices. Health Management Associates (HMA), is tracking these developments in the public payer space, replicating Centers for Medicare & Medicaid Services (CMS) payment methodologies, and modeling alternative policies to assist life science companies, payers, and other stakeholders.
In this article, we review the administration’s recent efforts to reduce Medicare and Medicaid spending on drugs and biologics, including confidential manufacturer negotiations and three new models that together could reshape pricing dynamics across federal programs.
Executive Branch Negotiations Seek to Drive Access to MFN Discounts
In 2025, the administration issued an Executive Order directing federal agencies to pursue strategies to establish MFN pricing, linking US prices for certain drugs to the lowest (or second lowest) adjusted net prices among a targeted set of peer countries. Following the order, federal officials sent letters to 17 major pharmaceutical and biotechnology manufacturers, urging them to negotiate agreements that would voluntarily align prices with MFN-based benchmarks.
To date, 14 manufacturers have signed agreements, though full details remain confidential. These agreements are understood to accomplish the following:
- Provide state Medicaid programs with access to MFNbased discounts
- Require that new drugs be launched in the United States at MFNaligned prices
- Offer certain drugs at discounted directtoconsumer prices through a forthcoming “TrumpRx” program, expected to launch later this year
Reports suggest that manufacturers entering these MFN-related arrangements may receive exemptions from several federal actions, including the Center for Medicare and Medicaid Innovation (Innovation Center) demonstration models described below and certain tariff-related policies.
MFNLinked Models Designed to Lower Drug Costs Across Medicare and Medicaid
Along with the negotiation efforts, the CMS Innovation Center has proposed three models that would test MFNbased pricing through structured rebate mechanisms. Each model targets different segments of the market while testing how international benchmarks could be integrated into federal drug payment policy.
New Models Test Alternatives to Inflation Rebates
Announced in December 2025, the Global Benchmark for Efficient Drug Pricing (GLOBE) Model and the Guarding US Medicare Against Rising Drug Costs (GUARD) Model are designed to test alternative approaches to the Inflation Reduction Act’s (IRA) inflation penalty policies. CMS plans to test the models’ potential for market driven price reductions if manufacturers choose to lower list prices instead of paying MFN-based rebates.
Key features of the GLOBE Model are as follows:
- Applies to 25 percent of Medicare fee-for-service (FFS) beneficiaries using certain Part B drugs
- Beginning in October 2026, becomes mandatory for select drugs and targets highspending, physicianadministered Part B categories, excluding products already subject to IRA negotiations, generics, biosimilars, and certain lowspend products
- No changes to physician and hospital reimbursement, although beneficiaries expected to see reduced cost sharing
The GUARD Model will similarly test whether applying MFN-based rebates to Medicare Part D drugs will lower Medicare costs. Key aspects of this model include:
- Fiveyear model that would start January 1, 2027
- Target therapeutic categories with more than $69 million in annual Part D spending
- No impact on plan bids and beneficiary cost sharing
These models rely on pricing data from 19 countries. Manufacturers that voluntarily submit net price information would trigger quarterly benchmark updates; otherwise, CMS will use a fixed list price based benchmark for the entire pilot period.
CMS is seeking comments on whether additional categories, for example cell and gene therapies, should be excluded from GLOBE. GUARD is also open for comment through February 23, 2026.
GENErating cost Reductions fOr US Medicaid (GENEROUS) Model
The GENEROUS model, expected to begin in 2026, creates a voluntary pathway for state Medicaid programs and manufacturers to enter supplemental rebate agreements tied to MFNaligned prices. MFN pricing under this model is based on the second lowest net price in G7 countries plus Denmark and Switzerland. GENEROUS is also expected to align with pricing commitments negotiated through the administration’s manufacturer agreements.
Key Considerations and Potential Impacts
The combined effect of federal negotiations and Innovation Center models could be substantial, though outcomes will depend on manufacturer participation, benchmark stability, and operational feasibility. Key considerations include:
- State Medicaid savings, especially the extent to which MFN‑linked rebates exceed existing supplemental rebates
- Reduced Medicare beneficiary cost sharing for Part B included in GLOBE
- Shifts in manufacturer pricing strategies, including potential changes to US launch prices
- Interactions with the IRA, particularly Part D redesign and Part B inflation penalties
Connect with Us
HMA experts continue to track the federal drug pricing landscape closely as comments, operational details, and implementation timelines evolve across these initiatives. Our team replicates CMS payment methodologies and models alternative policies using the most current Medicare FFS and Medicare Advantage (100%) claims data.
For more information and questions about the policies described in this article, please contact our experts below.
Preparing for Medicaid Community Engagement Requirements—Key Steps and Opportunities for States and Plans
On December 8, 2025, the Centers for Medicare & Medicaid Services (CMS) issued anticipated guidance on Medicaid community engagement requirements, as established in the 2025 budget reconciliation legislation (P.L. 119-21, referred to as OBBBA). This guidance arrives at a pivotal moment, as states begin budget planning and legislative sessions.
Health Management Associates (HMA) reviewed the guidance in the context of other policy and financing shifts that are affecting the Medicaid program. This article highlights key takeaways, addresses considerations for implementation, and issues for policymakers and healthcare organizations to track.
Brief Background
Generally speaking, Section 71119 of OBBBA requires states to implement community engagement requirements as a condition of Medicaid eligibility for individuals in the expansion population ages 19−64 who are neither pregnant nor enrolled in Medicare or any other mandatory Medicaid group. The guidance explains the statutory requirements related to how states verify community engagement, notify applicants and beneficiaries, ensure compliance with federal standards as the January 2027 deadline approaches, and other core components of the policy.
Starting January 1, 2027, states must require certain Medicaid expansion applicants to demonstrate community engagement for at least one month and may require up to three consecutive months immediately prior to the month of application. If compliance or exemption status is unverifiable at the time of application, states must provide notice and an opportunity to respond. These enrollees will maintain coverage during the response period. States are also expected to establish clear documentation standards and proactive communication processes for applicants and enrollees.
Three Key Takeaways from the Initial Guidance
1. Organizations must understand the key dates leading up to January 1, 2027
Limited new funding and tight timelines make January 1, 2027, a critical deadline for implementation. Medicaid organizations need to consider, however, the full sequence of events leading up to that date, including providing required advance notification to individuals about the changes and their eligibility status. Documentation and progress tracking are essential, both for compliance and to demonstrate that CMS deadlines are being met.
Although the guidance outlines notice and response requirements, it leaves open critical questions about how states will prevent procedural disenrollments, manage increased appeals volume, and mitigate due process legal risk if eligibility and verification systems fail at scale.
2. Medicaid managed care organizations (MCOs) have a limited role in decision-making but are key to engagement
Medicaid managed care organizations are prohibited from making the determination that an individual has met the community engagement requirement; however, they have an opportunity to support individuals in a range of ways. Recent changes under OBBBA give plans clearer authority to conduct proactive outreach on eligibility and renewal requirements, which strengthens their ability to help members navigate deadlines, reporting expectations, and documentation needs. This capacity will be important because a lack of predictability in enrollment and churn can meaningfully affect the risk profile of plans and, as a result, increase volatility in provider negotiations.
Plans, providers, community organizations, and state and local agencies can collaborate to develop effective engagement strategies, aligned messaging, and ongoing touch points. Helping members understand what is required—and when—and connecting them with resources to take action will be essential for successful implementation.
3. States and partner organizations need a global view of IT changes and functionality
CMS emphasizes that the eligibility determinations for the community engagement requirements should function seamlessly with new and existing system functionality. Meeting this expectation requires states to have a deep understanding of whether and how policies can be operationalized in their systems without adding administrative burden for individuals and others that engage with the systems.
Meeting federal expectations may be particularly challenging for states with county-based Medicaid systems, as implementing these requirements across multiple jurisdictions may necessitate a longer transition period. The OBBBA includes $200 million in total grant funding for implementation activities in 2026, and states can apply for enhanced federal IT funding at the 90/10 or 75/25 rates for certain costs and activities. Federal resources are otherwise limited, so it is critical that states and partner organizations establish a well-defined strategy to maximize available funding to support the system changes required to implement OBBBA eligibility requirements.
What to Watch
The guidance arrives as many governors begin releasing their budget proposals and planning for upcoming legislative sessions. Although the guidance provides clear information on the overarching parameters and a preliminary road map, certain critical details are forthcoming. State budgets should reflect the requirements and anticipate the need for rapid system and process development.
CMS will issue an interim final rule by June 1, 2026, and states must implement the community engagement requirement no later than January 1, 2027. States must comply with these requirements and act quickly to develop, pay for, and implement new systems, policies, and processes—ideally before the latter half of 2026.
CMS is developing additional guidance in several areas, including:
- Use of reliable data sources and how to satisfy the definition of engagement
- Implementation of the requirement to conduct renewals every six months for certain individuals
- Specific documentation requirements for community engagement
- Potential role that managed care plans can play unrelated to determining beneficiary compliance
States and Medicaid organizations should closely monitor these developments and be prepared to adjust their strategies as new information becomes available.
Connect with Us
HMA’s experts are trusted problem solvers, partnering with states to navigate the complexities of community engagement planning, even as requirements and details continue to evolve. Drawing on deep state and federal experience, as well as lessons learned from previous large-scale eligibility reforms, our team helps Medicaid-focused organizations quickly design and implement practical, context-specific strategies that align with OBBBA requirements. Whether it’s strategy development, system design, or crafting effective messages, HMA brings a flexible, solutions-oriented approach to maximize continuity of coverage and meet each client’s unique needs.
Contact our featured experts below to discuss how we can support your team in navigating these changes and building effective engagement strategies.
Five Key Takeaways from the 2025 National Association of Medicaid Directors (NAMD) Conference
At the National Association of Medicaid Directors (NAMD) 2025 Fall Conference, planned federal health policy changes dominated conversations among attendees, including state Medicaid directors, health plans, and providers. With major changes on the horizon for Medicaid and Affordable Care Act (ACA) Marketplace programs, stakeholders are preparing for transition and transformation in 2026.
A team from Health Management Associates (HMA) attended the conference and returned with valuable insights on the emerging opportunities, state-specific priorities for 2026 and beyond, and early strategies to address and mitigate the challenges ahead. Among the topics discussed were the Rural Health Transformation Program (RHTP), Medicaid eligibility and community engagement policy changes, drug costs and financing, upstream drivers of health, and data infrastructure.
Five major takeaways about the work state Medicaid agencies, health plans, providers, and industry partners will focus on in the year ahead were as follows.
1. Medicaid leaders are preparing for new eligibility and community engagement policies under tight timelines.
The 2025 budget reconciliation act (P.L. 119-21, OBBBA) requires certain adults ages 19–64 enrolled in Medicaid to complete at least 80 hours per month of community engagement (CE) to maintain coverage. Exemptions to the CE requirement apply to people with disabilities, pregnant individuals, and caregivers. States must now develop processes and information systems that track and verify compliance with CE requirements, manage exemptions, and support members through this policy change.
Medicaid CE and other new eligibility requirements, including more frequent eligibility checks, were a frequent topic of discussion throughout the event. Implementation of these requirements is a major operational lift with significant program integrity implications. State leaders discussed the tight timelines, resource constraints, and the need to coordinate across agencies, health plans, and providers. They are already planning to mitigate the risk of coverage losses for at-risk populations and to minimize administrative burden for all stakeholders. The urgency and complexity of these changes underscore the need for strategic planning and cross-sector collaboration.
2. Coordinated communication and stakeholder engagement remain critical.
States are increasingly relying on multiple forms of communication and feedback channels to engage stakeholders, including Medicaid members. Clear, timely communication is essential to ensure people understand their options and know what they need to do and when to do it. Medicaid leaders described the value of embedding vital eligibility information into workflows at all levels and applying lessons from the COVID-19 public health emergency unwind to new outreach and education initiatives.
Several states emphasized the effectiveness of convening all stakeholders to ensure unified messaging. Other common themes included the importance of plain-language materials, hands-on support through case managers and navigators, and engaging providers to integrate new eligibility and work-related requirements into their workflows, as policies evolve.
3. States are eager to begin implementing initiatives in their rural health transformation plans.
Medicaid leaders are actively discussing their RHTP applications with CMS, preparing to move quickly once awards are announced. Many states are focused on enhancing existing efforts, while others are preparing to invest in systems, technology, and organizations that will better integrate rural providers into the broader healthcare system, including Medicaid.
Federal and state leaders and their partners discussed the opportunity for RHTP funding to strengthen rural health infrastructure, workforce development, education, and outreach—especially in underserved areas. States are positioning themselves to leverage these funds to address persistent disparities and improve access to care for rural populations.
4. States are seeking to balance cost and access to GLP-1s and other prescription drugs.
Federal and state leaders extolled the benefits of new and innovative prescription drug products and therapies, including GLP-1s. Centers for Medicare & Medicaid Services (CMS) Administrator Dr. Mehmet Oz highlighted the administration’s announcements about drug pricing, including the new GENEROUS (GENErating cost Reductions fOr US Medicaid) model, which is focused on drug costs in the Medicaid program. These discussions reinforced CMS’s focus on new drug pricing models and the importance of involving Medicaid experts in these nuanced development and implementation conversations.
Attendees gained a deeper appreciation for the administration’s intent to have GLP-1s and other therapies play a significant role in addressing chronic disease, including obesity. State Medicaid agencies—and their Medicaid managed care plans and partners—should plan to inform discussions about coverage and financing of these novel products as well as for cell and gene therapies. The intersection of innovation, affordability, and access will remain a central challenge.
5. Medicaid agencies are working on multiple technology interoperability and quality initiatives.
Although Medicaid eligibility policy changes and CE requirements drew significant attention, many discussions also focused on other upcoming deadlines, including:
- New federal interoperability and prior authorization rules that go into effect in 2027
- State implementation of Medicaid and CHIP Quality Rating System requirements before the end of 2028
- The transition to digital quality measurement (dQM) by 2030
Medicaid agencies are collaborating with managed care and provider organizations to understand the operational, clinical, and technical dimensions of these initiatives.
Connect with Us
HMA’s expert consultants provide advanced policy, technical, and operational support, and can help your organization navigate and succeed in the evolving regulatory landscape. Our team brings deep experience and practical solutions to help clients anticipate challenges, leverage opportunities, and achieve their program goals. For more information or technical assistance on these and other emerging Medicaid priorities, contact the HMA’s featured experts below.
MassHealth Signals Continuity Mixed with Uncertainty as 1115 Waiver Renewal Process Begins
The Massachusetts Executive Office of Health and Human Services has begun early stakeholder engagement for the next Section 1115 demonstration waiver from 2028 to 2032, which will reflect the priorities of MassHealth, the Commonwealth’s Medicaid and CHIP (Children’s Health Insurance Program) system. The program covers roughly two million residents and operates with a budget of more than $20 billion in annual state and federal spending.
In two public meetings November 10 and 17, 2025, senior officials from MassHealth—Ryan Schwarz and Caitlin Towey—outlined MassHealth’s early thinking for the next 1115 demonstration in the “Roadmap for MassHealth’s 2028–2032 1115 Demonstration Extension,” released in October 2025. They emphasized the Commonwealth’s commitment to preserving core programs while acknowledging a more challenging federal landscape than in prior waiver cycles.
The roadmap highlights the 28-year trajectory of progress enabled by Massachusetts’ 1115 authority—from establishing the Accountable Care Organization (ACO) model and expanding substance use disorder (SUD) treatment, to strengthening safety net providers and driving the uninsured rate to 3 percent, the lowest in the nation. More recent demonstration cycles have deepened primary care investments, expanded the behavioral health continuum, advanced health equity incentives, and integrated housing and nutrition supports into ACO benefits.
Nonetheless, the roadmap also underscores the significant headwinds that are shaping the next waiver. The federal budget reconciliation act (P.L. 119-21, OBBBA) signed in July 2025 is projected to result in coverage losses for up to 300,000 Massachusettsresidents and as much as $3.5 billion in lost annual federal healthcare funding. Meanwhile, new federal policy stances, such as rescinding health-related social needs (HRSN) guidance and discontinuing approval of continuous eligibility authorities, will require Massachusetts to rethink elements of its current demonstration. State budget pressures are also a factor. MassHealth now accounts for nearly one-third of total state spending.
A major source of uncertainty is the lack of federal guidance on several core elements of the existing waiver. During November’s stakeholder sessions, state leaders said they are still awaiting direction from the Centers for Medicare & Medicaid Services (CMS) on several issues, including budget neutrality, hospital transformation funding, and HRSN services.
- HRSN: Current HRSN initiatives were enabled by guidance issued under the Biden Administration, which has since been rescinded. MassHealth officials said they intend to request approval for HRSN-like services in the upcoming waiver, even if the program must be redesigned or authorized through different mechanisms.
- Workforce Initiatives: Workforce funding, currently about $40 million over five years, will not be allowed under 1115 authority moving forward. State officials said they must identify alternative pathways to sustain or reconfigure workforce efforts if they are to continue.
- ACO & MCO Programs: Stakeholders asked for updates to the ACO and managed care organization (MCO) programs. MassHealth confirmed that the current ACO contracts run through December 31, 2027; however, they did note that Tufts Health Plan will exit the MCO program at the end of 2025, though this will have no effect on MassHealth’s two ACOs. Future ACO and MCO re-procurements could lead to changes, but those decisions remain several years out.
- Behavioral Health: Behavioral health policy also drew substantial interest. The state is assessing its behavioral health diversion system to determine which components require continued 1115 authority and where changes may be needed. Officials also confirmed that they intend to request continued 1115 authority for the Program for Assertive Community Treatment (PACT)—a multidisciplinary service for individuals with serious mental illness.
- Primary Care: Officials described a “crisis in primary care access”, driven by provider shortages and prolonged underinvestment. Although Massachusetts has historically led the nation in primary care spending, state leaders noted that the 1115 waiver alone cannot resolve these challenges. Gov. Maura Healey’s administration has convened a new task force to assess primary care access and financing, and MassHealth indicated it intends to align with that panel’s work.
- Cost Containment: Cost containment remains a priority. Officials said managing rising program costs is a theme that will be embedded throughout the renewal process.
As that effort unfolds in 2026, the State appears to be focused on maintaining core programs, adapting to uncertain federal guidance, and preserving flexibility. Officials said they are evaluating whether some current initiatives may need to shift from waiver authority to the State Plan, depending on forthcoming CMS policies. They are also closely monitoring other states’ expiring waivers to understand what CMS may approve under the current administration.
HMA experts have extensive expertise in helping to draft, implement, and evaluate 1115 demonstrations across the country. Our team in Massachusetts will be following the Commonwealth’s efforts closely and are available to answer your organization’s questions on how to navigate these new developments.
State Medicaid Programs Face New Challenges: Findings from the 2025 Medicaid Budget Survey
KFF and Health Management Associates (HMA), on November 13, 2025, released the annual Medicaid Budget Survey, A View of Medicaid Today and a Look Ahead: Balancing Access, Budgets and Upcoming Changes Results from an Annual Medicaid Budget Survey for State Fiscal Years 2025 and 2026. Now in its 25th year, this report offers a window into the evolving landscape of state Medicaid policy, financing, and operations across the United States. The survey was conducted in collaboration with the National Association of Medicaid Directors (NAMD), with 48 states providing survey responses by October 2025.
Released before the NAMD 2025 Fall Conference, Medicaid directors’ insights and the challenges, priorities, and innovations shaping Medicaid programs in fiscal years (FYs) 2025 and 2026 will figure prominently at this event. A team of HMA experts will be in attendance and available to address new developments and opportunities in state Medicaid policy and financing.
Key Trends and Challenges
Fiscal Pressures and Budget Uncertainty
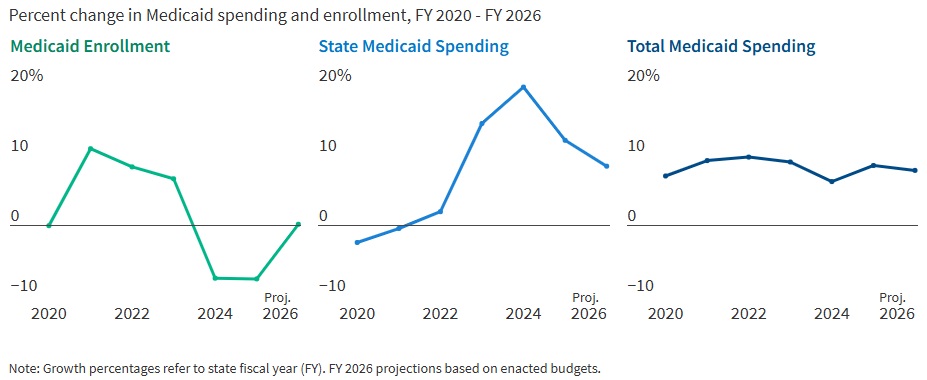
States are entering FY 2026 with slower revenue growth and rising healthcare costs. In FY 2025, Medicaid enrollment dropped by 7.6 percent as pandemic-era continuous coverage policies ended, but spending continued to climb. In fact, total Medicaid spending grew 8.6 percent in FY 2025 and is projected to rise another 7.9 percent in FY 2026. State Medicaid spending growth is expected to slow from 12.2 percent in FY 2025 to 8.5 percent in FY 2026. Nearly two-thirds of Medicaid directors, however, thought the odds of a Medicaid budget shortfall in FY 2026 was “50-50,” “likely,” or “almost certain.” Cost drivers include increases in provider rates, higher acuity enrollees, greater long-term care and behavioral health utilization, and rising pharmacy costs, especially for specialty drugs.
Figure 1. Medicaid Spending and Enrollment Trends Since the COVID-19 Pandemic Began
Federal Policy Changes and Provider Taxes
States are preparing for major federal policy changes under the 2025 budget reconciliation law (OBBBA), which will reduce federal Medicaid funding and impose new eligibility requirements. On November 14, 2025, the Centers for Medicare & Medicaid Services issued guidance regarding the OBBBA’s restrictions on states’ ability to use healthcare-related provider taxes to finance Medicaid programs (see CMS Provider Tax Guidance Places New Pressures on Medicaid Budgets). States are now generally prohibited from enacting new provider taxes or increasing existing ones after July 4, 2025, and must comply with new rules by the end of FY 2026 or FY 2028, depending on the tax type. In particular, beginning in federal FY 2028, the OBBBA gradually reduces the safe harbor provider tax limit for states that have adopted the ACA Medicaid expansion by 0.5 percent annually until the safe harbor limit reaches 3.5 percent of net patient revenues in federal FY 2032. These changes will reduce states’ flexibility to use provider taxes as a source of non-federal Medicaid funding, potentially leading to budget gaps and reductions in provider payments if lost revenue cannot be replaced.
Policy Changes and Priorities
Managing Risk in Managed Care Programs
A total of 46 states operate some form of managed care, and capitated managed care remains the predominant delivery system for Medicaid in most states. Most states that contract with capitated managed care organizations (MCOs) reported imposing a minimum medical loss ratio (MLR) requirement, requiring remittance payments when an MCO falls short of the minimum MLR requirement, and using risk corridors to manage financial risk and ensure value. States are also grappling with the growing use of artificial intelligence, particularly in the context of managed care prior authorization. Early policies focus on transparency, oversight, and ensuring human review to address concerns about bias, inappropriate denials, and privacy risks.
An Uptick in Provider Rate Reductions and Provider Tax Restrictions on the Horizon
Most states implemented fee-for-service rate increases for at least one provider category in FY 2025 and FY 2026. The number of increases is slowing, however, and there was an increase in states reporting provider rate restrictions compared with previous years. States continue to target rate increases for nursing facilities and home and community-based services more than other provider types.
Provider taxes remain a key source of the non-federal share of Medicaid funding, with all states except Alaska having at least one tax. These taxes accounted for a median 18 percent of states’ FY 2026 non-federal Medicaid financing, but new federal restrictions enacted in the OBBBA will limit states’ ability to use or expand these taxes going forward. As of July 1, 2025, 31 Medicaid expansion states reported having a non-exempt provider tax greater than the 3.5 percent of net patient revenues and therefore subject to the OBBBA’s phase down requirement.
Strong Benefit Enhancements and Scrutiny of Prescription Drugs
New Medicaid benefits and benefit enhancements continued to outpace benefit cuts and limitations. In all, 37 states reported new or enhanced benefits in FY 2025, and 36 plan to add or enhance benefits in FY 2026. More specifically, states reported expanding services across the behavioral health care continuum and for prenatal, delivery, and postpartum services. Most states reported at least one new or expanded initiative to contain prescription drug costs, including participation in the Centers for Medicare & Medicaid Services (CMS) Cell and Gene Therapy Access Model. State responses also reflected a waning interest in expanding Medicaid coverage for costly obesity drugs (GLP-1s), with some states restricting coverage because of budget pressures.
Challenges and Priorities
Many states are confronting more difficult fiscal conditions while also preparing for future fiscal uncertainty driven, in part, by the OBBBA. Medicaid leaders also expressed concern about the complexity of implementing new federal requirements, including work requirements and more frequent eligibility determinations. At the same time, state Medicaid leaders reported that they continue to pursue a variety of program priorities to expand access, especially to behavioral health and long-term care services, implement initiatives targeting specific populations (e.g., people who are pregnant, justice-involved, and at risk of homelessness), reform and strengthen delivery systems, modernize IT systems and infrastructure, and expand program integrity efforts.
Connect with Us
States face a challenging fiscal environment as they balance cost containment, quality, and access in their Medicaid programs. The combination of rising healthcare costs, new federal restrictions on provider taxes, and anticipated funding reductions will require states to make decisions about coverage, benefits, and provider payments. Nonetheless, states remain committed to maintaining quality and access for Medicaid beneficiaries, using available resources, and pursuing innovative approaches to care delivery.
For more information about the key takeaways from the KFF report and HMA’s Medicaid solutions, contact our experts below.
Keep up to date with the
HMA Weekly Roundup.
We deliver timely, expert-driven updates to help you stay informed and ahead of the curve.
CMS Provider Tax Guidance Places New Pressures on Medicaid Budgets
The Centers for Medicare & Medicaid Services (CMS) issued a letter on November 14, 2025, which provides preliminary guidance on healthcare-related taxes affected by Sections 71115 and 71117 of the Budget Reconciliation Act of 2025 (OBBBA, P.L. 119-21)—the portion of the legislation that focuses on new limitations on provider assessments.
Although this letter does not change federal regulations, it signals an important policy shift that will affect how states fund their Medicaid programs. CMS is working to incorporate these interpretations into rulemaking through the federal notice and comment process.
Health Management Associates (HMA) reviewed the letter specific to these provisions and in the context of other policy and financing changes that are affecting the Medicaid program. This article highlights key clarifications in the letter, the impact of the preliminary guidance on states, and the potential for the guidance to shape Medicaid budgets, financing strategies, and future policy reforms.
Guidance Clarifies the Meaning of “Enacted” and “Imposes”
OBBBA prohibits states from establishing new provider taxes after July 4, 2025. Existing provider taxes may be grandfathered if they meet specific criteria, but most taxes in expansion states—except those on nursing and intermediate care facilities—will be phased down starting October 1, 2027. To qualify for grandfathering, a tax must be both “enacted” and “imposed” by July 4, 2025, as defined by CMS.
CMS interprets enacted and imposed in the following way.
- Enacted: CMS defines enacted based on two components. First, the state or local government must have completed the legislative process to authorize the tax by July 4, 2025. Second, any necessary tax waiver of the broad-based and uniformity requirements must be approved no later than July 4, 2025. This interpretation will present challenges for some states as any pending tax waiver requests and approvals issued after July 4, 2025, will not qualify for grandfathering.
- Imposed: In addition to the enacted requirements, a state must have been actively collecting revenue for the new tax as of July 4, 2025. CMS does appear to allow for instances in which a state’s routine collection and billing practices require the tax be paid on a delayed schedule—a common practice across states.
CMS may continue to approve pending state proposals for new and revised tax structures; however, with the approvals, CMS is also notifying states that any tax structure that is ineligible for grandfathering must be revised by October 1, 2026, to comply with Section 71115 of the OBBBA.
Guidance Sets Preliminary Timeline for Compliance with New Broad-based and Uniformity Requirements in Section 71117
The OBBBA and a separately proposed rule published in May 2025 provide CMS with additional flexibility to tighten requirements for waivers that allow states to impose provider taxes that are not broad-based and uniform (i.e., the tax is levied on providers in a class at a common rate). CMS believes states have used a strategy to pass the prescribed statistical test for these waivers while shifting a disproportionate share of tax burden to high Medicaid providers.
The November 14 letter also includes a preliminary timeline for states to restructure their taxes to comply with the new requirements related to waivers of the broad-based and uniformity tests.
- MCO taxes: States that levy a higher tax rate on Medicaid managed care organizations (MCOs) than on other MCOs must submit a revised tax structure applicable to the state fiscal year (SFY) starting in calendar year (CY) 2026.
- Taxes on all other provider types: States with a similar tax structure on another provider class would need comply by the conclusion of the SFY, ending in CY 2028.
CMS notes that the preliminary timeline for the MCO taxes is the minimum transition period, and the final rule may allow for a transition period of up to three fiscal years.
What It Means for States
All states except Alaska rely on one or more provider tax(es) to fund their Medicaid programs. These additional limitations on the uses of provider taxes—including those now in place—will put a significant strain on state budgets, beginning as early as October 1, 2026. States may need to reduce provider reimbursement and/or enrollee benefits to address these losses.
States and providers should start planning for the changes in revenue now. Strategic planning for provider tax sustainability and close monitoring of upcoming CMS rulemaking are essential.
Connect with Us
The potential impact will vary by state, and each tax structure should be individually assessed to fully understand the implications of this new guidance. HMA has designed, developed, and helped implement provider taxes across the country and is uniquely positioned to support states, MCOs, and providers as they navigate the evolving landscape.
For details about the federal guidance and considerations for your organization, contact our experts below.
Keep up to date with the
HMA Weekly Roundup.
We deliver timely, expert-driven updates to help you stay informed and ahead of the curve.

Webinar Replay – Redefining Revenue: Building Financial Resilience in an Era of Policy and Payment Change
This webinar was held on December 11, 2025.
As healthcare organizations face sweeping shifts in Medicaid funding, workforce costs, and payer expectations, leaders must think beyond short-term cuts and find sustainable ways to protect access, quality, and mission.
During this webinar, HMA experts Jose Robles, Juan Montanez, and Kristina Ramos-Callan discussed how hospitals, health systems, and providers can reimagine revenue strategy for the next decade.
Learning Objectives:
- Understand the financial and operational implications of OBBBA and related regulatory changes on healthcare delivery.
- Identify strategies to stabilize payer mix, manage revenue volatility, and mitigate the effects of coverage loss.
- Explore technology and operational levers that enhance financial performance, including data analytics, automation, and care delivery redesign.
- Examine how innovation and mission-driven decision-making can strengthen organizational resilience and maintain equity in care.
- Apply insights to develop forward-looking plans that align fiscal responsibility with community health priorities.
25th annual KFF state Medicaid budget survey released
The 25th annual Medicaid Budget Survey conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD), was released on November 13, 2025 in the report A View of Medicaid Today and a Look Ahead: Balancing Access, Budgets and Upcoming Changes: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2025 and 2026.
Following years of significant changes in Medicaid spending, enrollment, and policy during the COVID-19 public health emergency and the subsequent Medicaid unwinding period, state Medicaid programs returned to more routine operations in state fiscal year (SFY) 2025 and were focused on an array of other priorities, including improving access to care or addressing social determinants of health.
Heading into SFY 2026, however, states were facing a more tenuous fiscal climate and beginning to prepare for another major set of policy changes to the Medicaid program. The 2025 federal budget reconciliation law (OBBBA) includes substantial Medicaid policy changes and reductions in federal funding, though the impacts vary by state. While many of the provisions do not take effect until FY 2027 or later, states are anticipating the upcoming changes, assessing budgetary and programmatic impacts, and preparing for the implementation of multiple and complex policy changes.
In addition to navigating state budget challenges and implementing new federal policies, the report also addresses other Medicaid program priorities including expanding access, implementing initiatives that target specific populations (e.g., pregnant individuals, justice-involved), continuing delivery system efforts, and improving administrative systems and functions.
Serving over one in five people living in the United States and accounting for nearly one-fifth of health care spending (and over half of long-term care spending), Medicaid represents a large share of state budgets and is a key part of the overall health care system.
The report was prepared by Kathleen Gifford, Aimee Lashbrook, and Carrie Rosenzweig from HMA; and by Elizabeth Hinton, Elizabeth Williams, Jada Raphael, Anna Mudumala, Robin Rudowitz from KFF. The survey was conducted in collaboration with NAMD.
Other links:
2025 Press Release
Medicaid Enrollment & Spending Growth: FY 2025 & 2026
Evaluation of the CareSource JobConnect program quantifies ROI for States
HMA recently released a report analyzing the impacts of the CareSource JobConnect Program, which provides employment assistance to non-elderly adults enrolled in Medicaid. CareSource is a national, nonprofit managed care organization dedicated to transforming healthcare for those served by government-sponsored health care programs. The program helps individuals prepare for a job search, obtain employment, and succeed in the workplace. HMA was engaged due to our significant expertise in Medicaid to evaluate the program’s impacts in 3 of the 6 states where it is currently active: Indiana, Georgia, and Ohio. HMA conducted an economic impact analysis to assess outcomes for members participating, a cost–benefit analysis, and a return-on-investment (ROI) assessment, examining the direct and indirect financial benefits to participants, the broader economic impact on the state and healthcare spending, and the total program operation costs incurred by CareSource.
The recently enacted OBBBA law established new federal standards that require states to verify that certain Medicaid enrollees are meeting minimum work or community engagement hours as a condition of continued coverage. Past efforts by states to establish work requirements as a condition of enrollment in Medicaid have resulted in coverage losses because of bureaucratic hurdles that made it difficult for people to comply. A program like CareSource JobConnect can provide support and assistance to those enrolled.
The analysis aimed to help CareSource understand the advantages of this program on those participating, as well as the broader impact on the state’s economy, and demonstrates potential gains for the state, the job seekers, and CareSource’s program if more people took advantage of the program’s benefits.
The report shows significant economic and workforce outcomes, particularly in Ohio and Indiana.
- Ohio led with the highest number of participants and employed workers, generating a return-on-investment of 13:1.
- Indiana showed impressive efficiency, with a strong return-on-investment of 12:1.
- Georgia’s results were still positive with a 5:1 ROI, but there are opportunities for improvement in employment success and economic return that could improve the success for the Georgia program.
HMA examined direct benefits to those newly employed through the program, including annual earnings and earnings supplements such as tax credits; indirect benefits, such as key elements of social determinants of health like food security and safe and affordable housing; new spending: new worker spending due to employment enhanced by the multiplier (defined as the ripple effect that occurs as new jobholders spend a large portion of their earnings, which creates income for local businesses and nonprofit organizations); the Benefit-to-Cost Ratio: The sum of direct and indirect benefits and the multiplier effect, divided by the cost incurred by the organization making the investment. These things together help determine the full ROI for the program.
As more participants receive job placements over time and their incomes increase, earning supplements will decrease, and other indirect benefits will decrease as participants earn more than the maximum amounts for eligibility. Each of the three states saw a net gain to their state budgets in the form of state sales and income taxes as members earn more and are able to spend their wages on goods and services.
| Indiana | Georgia | Ohio | |
| 2024 Participants with Employment through the Program | 87 | 28 | 198 |
| 2024 Participants in the Program | 220 | 188 | 566 |
| Aggregate New Worker Spending | $1,688,001 | $537,923 | $3,110,462 |
| Multiplier Effect | 5 | 5 | 5 |
| Aggregate Benefit to Participants and the Local Economy (new worker spending times multiplier) | $8,440,004 | $2,689,615 | $15,552,308 |
| Estimated Cost Per Participant | $2,938 | $2,230 | $1,988 |
| Benefit—Cost Ratio | 13:1 | 6:1 | 14:1 |
| Return-on-Investment | 12:1 | 5:1 | 13:1 |
To learn more about the program and to download the whitepaper, click here.
HMA has more than 40 years of experience in helping to shape and improve Medicaid programs, and supports organizations nationwide to develop, implement, and evaluate programs for state agencies, local governments, health plans, and other community-based partner organizations. Learn more about how HMA supports Medicaid and our efforts in Housing and Health.
Related resources: