This week, our In Focus section comes from HMA Medicaid Market Solutions (MMS) Managing Director Matt Powers and Senior Consultant Desmond Banks. On January 30, 2020, the Centers for Medicare & Medicaid Services (CMS) convened an event titled, Transforming Medicaid: A New Opportunity for Better Health, in Washington, DC, during which CMS Administrator Seema Verma announced the Healthy Adult Opportunity (HAO), an optional Section 1115 Medicaid Demonstration initiative. Commonly referred to as, “block grant” or “spending cap” model, the HAO seeks to provide states with enhanced flexibility to design and administer parts of their Medicaid program. Administrator Verma articulated the HAO to be an important step to support the fiscal sustainability of Medicaid and invited state Medicaid directors to submit waiver applications.
Background
Medicaid block grant and spending cap models have been debated and proposed for nearly 40 years:
- In 1981, President Ronald Reagan’s proposal for Medicaid block grants was rejected by Congress.
- In 1995, a Republican-controlled Congress advanced Medicaid block grants, but the measure was vetoed by President Bill Clinton.
- In 2004, Congress did not act upon President George W. Bush’s proposal for Medicaid block grants.
- In 2011 and 2012, Medicaid block grants were approved by a Republican-controlled House, however, a Democrat-controlled Senate did not act on the House budget plan, and it died in 2013.
- In 2017, Multiple Congressional bills that attempted to change provisions in the Affordable Care Act (i.e. Repeal and Replace bills) were debated and had block grant-like provisions for Medicaid. They included proposed global waivers and per capita spending caps for different Medicaid eligibility categories. None of these bills became law.
Despite not gaining traction for four decades, several significant steps related to a block grant model were displayed in 2019:
- On March 11, 2019, the Trump Administration endorsed Medicaid block grants within its FY 2020 budget, “The Administration recognizes that the only way to reform Medicaid and set it on a sound fiscal path is by putting states on equal footing with the Federal Government to implement comprehensive Medicaid financing reform through a per capita cap or block grant.” (p 43)
- On June 16, 2019, Alaska awarded a $100,000 contract for researchers to assess the feasibility of converting its Medicaid program to a block grant program; the paper was reportedly due to the state by June 30, 2019 but has not been publicly released.
- On September 17, 2019, Tennessee submitted a Medicaid block grant waiver. Tennessee’s proposal is the most comprehensive to date to request capped spending for a Medicaid program.
Key Questions & Answers
What are key HAO provisions?
Much of the flexibility proposed under the HAO is already available through Section 1115 demonstration authority. HAO and current Section 1115 waivers include ability for states to do the following:
- Adopt elements of a closed pharmacy formulary
- Share in savings achieved under the demonstration if the state agrees to reinvest the savings into the Medicaid program
- Support more independent state Medicaid authority to make administrative changes
- Reimburse federally qualified health centers (FQHCs) via value-based payment methodologies
- Propose alternatives to processes required under Medicaid managed care regulations
Who is covered?
The HAO applies almost exclusively to Affordable Care Act (ACA) Medicaid Expansion adults who:
- Are ages 19-64
- Do not qualify for Medicaid on the basis of disability or need for long-term services and supports
- Are not Medicare eligible
States may limit program eligibility to a targeted subset of the ACA Medicaid Expansion population including the following:
- Populations with income +/-133 percent federal poverty level (FPL) with specified clinical conditions
- Populations within geographic boundaries which may open the door for certain counties or municipalities to explore a Medicaid Expansion coverage waiver covered by local resources
Of note, 90 percent federal match is only available if full Medicaid expansion is implemented.
What services are covered?
Benefits offered under the HAO must align with the individual health insurance market, including coverage of essential health benefits (EHBs), at minimum. States may vary benefits offered to populations covered under a HAO waiver from those provided under the Medicaid State Plan and are not required to meet wraparound service requirements such as transportation. States may also opt to provide coverage for additional services which would enhance coverage, improve health outcomes, and address “determinants to promote independence.”
How is state funding calculated?
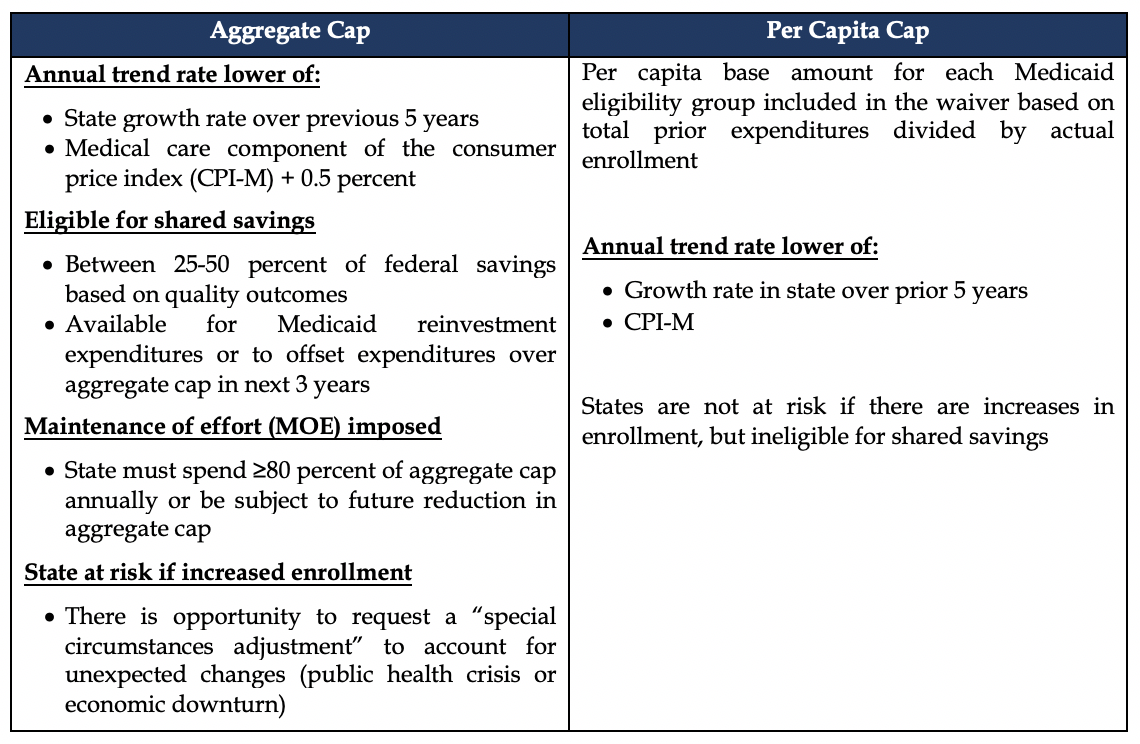
As illustrated in Table 1, states may select an aggregate or per capita funding model. Under both models, the base payment rate is determined by the last eight quarters of expenditures attributable to the proposed HAO waiver population, with the exception of: disproportionate share hospital (DSH) payments, administrative expenses, public health emergency expenditures, services available at the 100% federal match, and certain supplemental and pool payments.
Table 1. Comparison of HAO Funding Options
How many states have expressed interest in pursuing the HAO?
Four states have expressed at least some interest in pursuing the HAO or general block grant principles. Oklahoma announced interest in the HAO opportunity. Arkansas is reviewing the opportunity and has state legislation requiring pursuit of a block grant. Alaska has previously expressed interest in a block grant model. Alabama has expressed concerns regarding how to fund expansion and has indicated they “will certainly look at the [HAO].”[1] Notably, Tennessee already had a broad block grant proposal submitted to CMS which differs significantly from the policies announced in the HAO guidance.
Is the HAO susceptible to legal challenges?
Although the HAO affords states greater flexibility for their Medicaid programs, it is not what has been historically presented as a block grant. Perhaps in anticipation of legal challenges, HAO has:
- Prohibited inclusion of State Plan populations
- Required states to provide baseline performance on “Adult Core Set”
- Incorporated financial components already available through 1115 waiver authority
HAO will likely be challenged under the overarching premise of whether HAO furthers Medicaid goals and objectives.
Conclusion
Similar to other recently approved 1115 waiver policies, the HAO represents an additional attempt to give states authority over their Medicaid programs. The ultimate impact of the HAO will likely be shaped by the willingness among states to accept some financial risk in exchange for greater autonomy over the operation of their Medicaid programs and by potential litigation.
For more information, please contact our experts below.
Link to Healthy Adult Opportunity
[1] ABC News. What could President Trump’s new Medicaid funding model mean for Alabama? Accessed February 4, 2020.
