Rare Disease Day is observed globally each year on February 28 to raise awareness, access, and diagnosis to therapies for people with rare diseases. Today HMA releases a report titled Analyzing the Impact of Policies to Exclude Certain Orphan Drugs from the Drug Price Negotiation Program of the Inflation Reduction Act, that examines how many orphan drugs the ORPHAN Cures Act might affect and the percentage of Medicare Part B and Part D spending that is attributable to these drugs. Using that information, we estimated how the legislation would affect federal spending, applying the same assumptions and methodology that the Congressional Budget Office (CBO) uses in a 10-year budget score.
252 Results found.

State Cost Growth Benchmarking Programs: An Evaluation of Eight States’ Experiences and the Lessons Stakeholders Have Learned
Background
In 2024, Health Management Associates (HMA) evaluated programs implemented by eight states (California, Connecticut, Delaware, Massachusetts, New Jersey, Oregon, Rhode Island, and Washington) aimed at controlling healthcare cost growth. In recent years, these states have tried to address the trend of escalating healthcare costs using an approach referred to as cost growth benchmarking (CGB). This is the act of setting a target for annual healthcare cost growth and measuring actual performance against the target. Since 2018, the Peterson-Milbank Program (PMP) for Sustainable Health Care Costs has invested in state-based CGB efforts by funding program development, implementation, and technical assistance. HMA evaluated the Peterson Center on Healthcare’s cost growth benchmarking efforts across the eight states.
Methodology
HMA’s evaluation for the Peterson Center on Healthcare included a detailed landscape review for each of the eight states and interviews with 45 state officials, providers, payers, and other stakeholders in these states. The HMA team synthesized findings from the landscape review and the key informant interviews and produced an internal evaluation report.
Analytic Approach
The landscape review captured the state’s CGB program chronology, governance structure, growth targets, enforcement authority, and performance against the target. The interviews examined the contextual factors, stakeholder influence, implementation developments, capacity to control costs, facilitators and barriers to developing cost control capabilities, and the lessons learned based on the states’ experience. The interview discussion guide included a scoring component which enabled quantitative analysis in addition to the qualitative findings. HMA analyzed these findings by state, category of interviewee (state officials, payers, providers, or others) and implementation stage (early vs. more recent adopters).
Findings
States’ efforts to engage and gather stakeholders, establish cost growth targets, collect and report data, and identify cost drivers have been successful, but states have had challenges to date in developing policies aimed at containing costs.
Utility
The findings from this analysis can be useful to the existing states in enhancing their CGB programs and to states interested in launching new CGB initiatives.
Medicare Hospital Inpatient Device-Intensive Payment Policy
Medicare’s fee-for-service (FFS) payment system includes payment policies that support providers’ use of innovative medical device technologies. The continued evolution of these policies is necessary to keep pace with current and future medical innovation. In this report, HMA summarizes models testing the implementation of a newly proposed policy for the hospital inpatient system which aims to eliminate systemic bias that may slow hospitals’ adoption of innovative technologies. HMA concludes that targeted policies that eliminate the use of the hospital wage index to standardize device costs can result in more accurate reimbursement for hospitals and increase beneficiary access to innovative technologies.
340B Duplicate Discounts: Enforcement Inconsistent and Weak Due to Lack of Data Transparency and Despite Federal Prohibition
At the intersection of the federal 340B Drug Pricing program and the federal Medicaid Drug Rebate Program (MDRP), a potentially large set of Medicaid claims are generating duplicate discounts, which pharmaceutical manufacturers provide to eligible entities such as hospitals and health centers. These two complex federal programs were designed to reduce the costs of prescription drugs for providers that serve low-income patients, but both state Medicaid agencies and federal policymakers have been actively working to eliminate the unintended overlap of these two programs. To gain deeper insights into why duplicate discounts continue to occur, the scope of this concern, and to identify considerations of future policymaking, HMA conducted interviews with Medicaid officials and drug policy experts across several states.
Duplicate discounts occur when for a single sale a manufacturer is required to: (1) prospectively reduce the price of the product (a discount) they sell to a 340B covered entity in advance of the delivery of care to the patient; and (2) provide a retrospective payment (a rebate) to a state Medicaid program or managed care plan under the MDRP after care is delivered to a Medicaid enrollee. When duplicate discounts occur the manufacturer’s product is discounted twice for the same sale, contravening federal law, which prohibits duplicate discounts.
Despite the statutory prohibition, duplicate discounts remain a concern. Both state and federal policymakers have been actively addressing duplicate discounts but have been unable to identify clear and consistent policy solutions that neutralize this inefficiency. On the state level, Medicaid agencies and state legislatures have implemented policies to address duplicate discounts. On the federal level, the Health Resources and Services Administration (HRSA) and the Centers for Medicare & Medicaid Services (CMS) have conducted audits and published best practices for states to eliminate duplicate discounts. Nonetheless, duplicate discounts persist.
To gain deeper insights into how Medicaid agencies navigate duplicate discounts, Health Management Associates (HMA) conducted semi-structured interviews with former and current Medicaid directors and pharmaceutical policy experts in 14 states. Interviewees were asked about the frequency of duplicate discounts, the extent to which Medicaid agencies devote resources to tracking them, the policies states have implemented to address them, and the extent to which state or federal authorities are working to eliminate duplicate discounts.
Based on interviews, four key themes emerged:
- Duplicate discounts remain a problem, the scope of the problem is unclear, and better data collection from covered entities is necessary.
- The opacity and complexity of duplicate discounts create a burden for state Medicaid agencies, influencing the policies they implement, resulting in variable state policy strategies.
- Contract pharmacies add an additional layer of complexity, exacerbating the burden that duplicate discounts create.
- State and federal authorities could take more decisive action to address duplicate discounts.
Policymakers should consider that the environment for addressing duplicate discounts may become more complex in the future, which may increase the need for a federally coordinated policy solution. The complexity of the environment may deepen due to the increasing presence of contract pharmacies, the increasing presence of managed care in Medicaid programs, and the implementation of the drug pricing policies of the Inflation Reduction Act of 2022. Policy action coordinated across the various stakeholders (e.g., HRSA, CMS, state Medicaid agencies, covered entities, and manufacturers) may represent the best opportunity for success in eliminating duplicate discounts.

CMS Releases Final 2026 Marketplace Benefit and Payment Parameters
Trump Administration and Congress to Consider Policy Changes
This week, our In Focus section reviews the final Notice of Benefit and Payment Parameters (NBPP) for 2026. The Centers for Medicare & Medicaid Services (CMS) rule, released January 13, 2025, describes the policy and payment parameters for issuers that participate in federally facilitated and state-based marketplaces in 2026.
The NBPP is particularly notable given that marketplace enrollment is at an all-time high. Last week, CMS reported that 24.2 million people joined a marketplace plan during 2025 Open Enrollment, exceeding last year’s historically high enrollment levels by more than 2 million people.[1] With millions more individuals covered in the individual market, this final rule presents several opportunities for the healthcare industry to improve the well-being of covered individuals and families and the financial health of participating organizations.
Marketplace policies are under scrutiny, however, from new Trump Administration officials and congressional leaders. Subsidies, eligibility, and reimbursement are among the topics receiving the greatest attention.
Key highlights from the final rule and considerations for stakeholders in the changing healthcare landscape follow.
Consumer Protections
The final rule further strengthens consumer protections, consistent with the policies advanced during the Biden Administration. CMS finalized policies to achieve the following:
- Protect consumers from agents and brokers seeking to make unauthorized changes to their healthcare coverage
- Allow the agency to take enforcement actions against lead insurance agents for violations of marketplace standards
- Expand the agency’s authority to immediately suspend an agent or a broker’s ability to make transactions within the marketplace if the information creates an unacceptable risk to the accuracy of marketplace eligibility determinations, operations, applicants, or enrollees, or marketplace IT systems
- Update the model consent form, which helps agents and brokers document consent from consumers to assist with their marketplace enrollments and submission of marketplace eligibility applications
Revisions to Marketplace User Fees
The enhanced premium tax credits are the driving force behind the increase in nationwide marketplace enrollment to more than 24 million today from 11.4 million in 2020. If not extended, or if Congress takes no action by July 31, 2025, CMS will increase the user fees collected to pay for administration of HealthCare.gov as follows:
- Increase fees to 2.5 percent of monthly premiums in 2026 for federally facilitated marketplaces (FFM) states, up from 1.5 percent in 2025
- Increase fees to 2.0 percent of monthly in 2026 for state-based marketplaces on the federal platform (SBM-FPs)—up from 1.2 percent in 2025
CMS also is finalizing an alternative set of user fee rates. If enhanced premium tax credit subsidies are extended through the 2026 benefit year by July 2025 at the current or a higher level the following user fees rates will apply:
- 2 percent for FFM states
- 1.8 percent for SBM-FPs
CMS originally proposed a March 2025 subsidy extension deadline for activating the lower user fee. Insurer should take into account the higher user fees when setting their 2026 premiums—SBMs as they finalize their 2026 user fee levels and FFM states considering the costs of staying in Healthcare.gov or transitioning to a SBM.
Premium Payment Threshold Options
CMS finalized new options for insurers to avoid triggering late payment grace periods for members who make most but not all their premium payment. The new threshold options are intended to minimize termination of coverage for people who owe small amounts. The options include:
- For the first month’s premium payment to effectuate coverage—or binder payments—the only option is to use a net premium threshold as low as 95 percent
- For all other premium payments after the first month’s payment, the options include:
- Net premiums as low as 95 percent or a fixed dollar threshold of up to $10
- Gross premiums percent of as low as 98 percent or fixed dollar threshold of up to $10
Fixed dollar thresholds will be adjusted for inflation.
Information Sharing and Transparency
CMS is finalizing policies designed to increase transparency and promote program improvements by publicly releasing state marketplace operations data, including spending on outreach and additional open enrollment customer service metrics, such as for call center performance surveys and website visits. The final rule clarifies that CMS will not publicly release each SBM’s annual State-based Marketplace Annual Reporting Tool (SMART), a reversal from what was proposed.
In addition, CMS is finalizing that it will share aggregated, summary-level Quality Improvement Strategy (QIS) information publicly on an annual basis starting January 1, 2026, with data submitted during the 2025 qualified health plan application period.
What’s Next/Key Considerations
The new leadership at the US Department of Health and Human Services (HHS) and CMS will likely conduct a thorough review of these payment and policy changes. In consideration of potential repeals or modifications, states and marketplace plans will need to consider the following:
- Uncertainty around extending or modifying Affordable Care Act subsidies
- Potential statutory changes approved by Congress and regulatory changes from the Trump Administration
- Review of existing operations and policies in light of the new regulations and the changing policy environment
Connect With Us
Health Management Associates experts support states, managed care organizations, consumer groups, and other interested stakeholders to achieve success in the operation of and participation in the marketplaces. Our team has the broadest historical perspective on the challenges and opportunities in this market and can support every step of the planning and execution processes to optimize markets as they continue to evolve in the coming months and years. If you have questions or want to discuss the final rule, contact our experts below.
[1] Centers for Medicare & Medicaid Services. Over 24 Million Consumers Selected Affordable Health Coverage in ACA Marketplace for 2025. January 17, 2025. Available at: https://www.cms.gov/newsroom/press-releases/over-24-million-consumers-selected-affordable-health-coverage-aca-marketplace-2025.
CMS Stays the Course with Proposed Payment Updates for Medicare Advantage and Part D Services in 2026
Trump Administration will Issue Final Policies
This week, our In Focus section examines the Centers for Medicare & Medicaid Services (CMS) calendar year (CY) 2026 Advance Notice for the Medicare Advantage (MA) and Medicare Part D programs, published January 10, 2025. That same day, CMS also released draft CY 2026 Part D Redesign Program Instructions. This regulatory guidance includes CY 2026 payment updates as well as additional technical and methodological changes to MA and Part D for the coming plan year.
The release of the CY 2026 Advance Notice—along with the complementary CMS policy and technical proposed rule released in November 2024—represent the last major Medicare regulations of the Biden Administration, and these annual payment and policy updates will be finalized under the incoming Trump Administration. As a result, the proposed MA and Part D payment policies could be modified before finalization in April 2025.
Comments on the Advance Notice are due by February 10, 2025, leaving a tight timeline for MA plans and other stakeholders to provide formal feedback and written comments to CMS. Following are brief summaries of the major proposals in the Advance Notice and key considerations for stakeholders as they analyze the proposals.
Payment Impact on Medicare Advantage Organizations
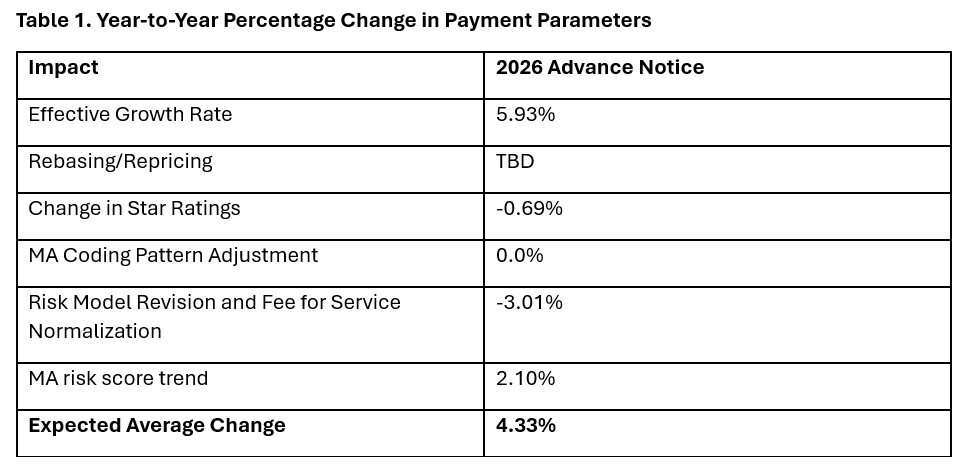
In the Advance Notice, CMS projects that federal payments to MA plans will increase by 4.33 percent from 2025 to 2026—which represents a $21 billion increase in expected payments to MA plans next year. CMS estimates that federal payments to MA plans in 2026 will total $590.9 billion.
The proposed increase in payments accounts for several factors, including growth rates in underlying costs, changes to MA Star Ratings, continued implementation of the new risk adjustment model, and MA risk score trends. The estimated growth rate considers demographic changes in MA enrollment, including projected increases in the number of enrollees.
The Advance Notice estimates represent the average increase in payments to MA plans and actual payments will vary from plan to plan. Below, Table 1 provides estimates of the impact of proposed policy changes on net MA plan payments.
MA Risk Adjustment Changes
CMS intends to complete the three-year phase-in of the MA risk adjustment model that was first published in the CY 2024 Rate Announcement. Specifically, CMS proposes to calculate 100 percent of the risk scores using the new MA risk adjustment model, referred to as the 2024 hierarchical condition categories (CMS-HCC) framework. CMS maintains that the changes to the methodology for calculating risk have improved the predictive accuracy of the model while ensuring risk-adjusted payments to MA plans are accurate.
In addition, CMS has been working to calibrate the risk adjustment model based on MA encounter data, and CMS proposes to begin phasing in an encounter-based MA risk adjustment model as soon as CY 2027.
CMS also proposes to apply the statutory minimum MA coding pattern difference adjustment factor of 5.90 percent for CY 2026.
Technical Adjustment to Cost Calculations Related to Medical Education Costs
Similar to changes in the MA risk adjustment model, CMS plans to complete the three-year phase-in of technical adjustments to the per capita cost calculations related to indirect and direct medical education costs associated with services delivered to MA beneficiaries. This technical adjustment—finalized in the CY 2024 Rate Announcement—has reduced growth rates for MA plans because of the removal of MA-related medical education costs from the benchmarks.
MA Star Ratings
CMS reiterates its continued focus on moving toward a “Universal Foundation” of measures with the goal of creating metrics that center on clinical care, patient outcomes, and improved patient experiences and are aligned across CMS programs. In addition, CMS is soliciting initial feedback on both substantive measure specification updates as well as comments on new measure concepts. CMS also is seeking stakeholder feedback on modifications to the Health Equity Index, including adding social risk factors and geography (urban or rural) to the reward factor. Any specific changes to MA Star Ratings measures, including modifications to the Health Equity Index, would occur through the formal rulemaking process.
Medicare Part D Provisions
The CY 2026 Advance Notice and the CY 2026 Draft Part D Redesign Program Instructions include several payment and benefit updates as required in the Inflation Reduction Act (IRA) of 2022. The CY 2026 updates include:
- The CY 2026 annual out-of-pocket cost threshold for Part D covered drugs is $2,100, which is the original out-of-pocket cap of $2,000 adjusted for the annual percentage increase in average expenditures for Part D covered drugs
- Establishment of the selected drug subsidy program
- Changes to the liability of enrollees, plan sponsors, drug manufacturers, and CMS in the standard Part D benefit design, specifically to account for the start of the Medicare Drug Price Negotiation Program in 2026
- Guidance on the successor regulation exception to the IRA’s formulary inclusion requirement for selected drugs under the Medicare Drug Price Negotiation Program
Other previously implemented IRA reforms will continue in CY 2026, including no cost sharing for Medicare beneficiaries for Part D covered drugs in the catastrophic phase, which begins after the annual out-of-pocket threshold of $2,100 is reached; a $35 monthly cap on enrollee cost sharing for insulin; no cost sharing for adult vaccines recommended by the Centers for Disease Control and Prevention’s (CDC’s) Advisory Commission on Immunization Practices and covered under Part D; and the requirement for Part D plans to offer the Medicare Prescription Payment Plan to beneficiaries.
What to Expect
The CY 2026 Advance Notice includes important technical, programmatic changes and payment updates for MA and Part D plans, which will be finalized when CMS publishes the final CY 2026 Rate Announcement on or before April 7, 2025. MA plans and other stakeholders have a rigid timeframe to provide formal input and written comments to CMS before the February 10 deadline.
Like the policy and technical changes included in the MA proposed rule, the CMS Advance Notice payment updates will be finalized under the incoming Trump Administration. MA plans and other stakeholder can anticipate that the new leadership at the US Department of Health and Human Services and CMS will closely examine and take a fresh look at the proposed payment and policy changes. Though the current CMS leadership maintains that payment updates included in the Advance Notice are sufficient to support stability in MA premiums and benefits, proposed payment policies can be modified or delayed as the new leadership takes shape.
For example, officials in the Trump Administration could seek to delay the phase in of the risk adjustment changes as well as the technical adjustment regarding medical education costs, which CMS estimates would result in an additional $10.4 billion in payments to MA plans.
Connect With Us
Medicare experts at Health Management Associates, will continue to assess and analyze the policy and political landscape, which will determine the final policies included in the CY 2026 Rate Announcement. HMA experts have the depth of knowledge, experience, and subject matter expertise to assist organizations that engage in the rulemaking process and to support implementation of final policies, including policy development, tailored analysis, and modeling capabilities.
For details about the CY 2026 MA Advance Notice and its impact on MA and Part D plans, providers, and beneficiaries, contact our featured experts below.
MyCare Ohio: The Next Generation’s Impact on the Ohio Medicare and Medicaid Landscape
This week, our In Focus section also reviews the significant efforts under way in Ohio to transform how the state provides healthcare services to its Medicare and Medicaid dual-eligible population. Effective January 1, 2026, MyCare Ohio will transition to the Next Generation of its program for people who are dually eligible for both programs.
Overview of Ohio’s Transition to Next Generation MyCare Ohio
This evolution moves Ohio to a fully integrated dual-eligible special needs plan (FIDE-SNP) model that seeks to achieve several key goals through a population-based health approach designed to address inequities and disparities in care for dual-eligible individuals. Examples include:
- Improved Care Coordination: Strengthening integration between Medicare and Medicaid services to provide seamless, holistic care for individuals, thereby reducing fragmentation and ensuring comprehensive management of medical, behavioral, and social needs
- Personalized Care: Applying data analytics and technology to create more tailored care plans, with a focus on proactive care to address the unique health needs of each individual, especially people with chronic conditions
- Expanded Access to Services: Increasing accessibility, particularly through telehealth and digital tools, to reach underserved populations and improve accessibility, particularly for people living in rural or remote regions
- Enhanced Quality of Care: Shifting focus from service volume to outcomes, encouraging providers to deliver high-quality care and improve patient satisfaction, while incentivizing preventive care to reduce hospital admissions and other high-cost interventions
- Technology Integration: Leveraging advanced technologies like mobile apps, predictive analytics, and telemedicine to monitor patient health, improve communication between patients and providers, and deliver care more efficiently
The MyCare program currently is offered in 29 counties across Ohio but will transition to a statewide program as a part of the Next Generation changes. In addition, coordination only dual-eligible special needs plans (CO-DSNP) will no longer be permitted.
After the Ohio Department of Medicaid (ODM) publicly released the request for applications and evaluated submitted proposals, the agency selected four managed care organizations (MCOs), which will become the Next Generation MyCare plans. The ODM awarded contracts to the following MCOs that will serve MyCare members beginning in January 2026: Anthem Blue Cross and Blue Shield, Buckeye Health Plan, CareSource, and Molina HealthCare of Ohio.
Considerations for the Market
The shift to the FIDE-SNP model and selection of four participating health plans will have a considerable impact on the competitive landscape for Medicare and Medicaid managed care in Ohio. The resulting changes may affect both selected and non-selected participants in different ways, including:
- Increased competition among MyCare MCOs: MCOs will need to focus on enhancing their care coordination systems, adopting new technologies, and developing personalized care plans to compete not just in terms of the volume of services provided, but also to the quality and effectiveness of healthcare delivery. Those plans that can best integrate services, offer proactive care management, and improve patient outcomes through value-based care and advanced technology initiatives will gain the competitive advantage, potentially attracting more beneficiaries.
- Strategic responses of nonparticipating MCOs to counter potential membership and financial losses: MCOs that lose members because they were not selected or are unable to offer CO-DSNPs moving forward, will likely strategize to gain membership through other product lines or benefit design to offset losses. Strategies may vary but might include tactics such as: enhancing benefits or decreasing member cost sharing to entice member movement across carriers for non-D-SNP plans; finding innovative ways to further reach different segments of the Medicare population, such as Special Supplemental Benefits for the Chronically Ill (SSBCI) packages or Chronic Condition SNP plans; or shifting their focus to product lines outside of Medicare Advantage and Medicaid.
Connect with Us
Ohio is one of many states transitioning to a FIDE model beginning January 2026. Health Management Associates, Inc. (HMA), has successfully supported participating and nonparticipating carriers throughout the transition process and continues to be a dedicated partner to organizations navigating Medicare and Medicaid changes across the country.
Contact our featured experts below, to learn more about the Ohio FIDE-SNP initiative and HMA’s capabilities and expertise to support states, carriers, and other key partners with these transitions.
CMS Announces Medicare Advantage Value-Based Insurance Design Model Will End After 2025
The Centers for Medicare & Medicaid Services (CMS) announced on December 16, 2024, that it will be terminating the Medicare Advantage Value-Based Insurance Design (VBID) model at the end of 2025 because of the model’s “substantial and unmitigable costs to the Medicare Trust Funds.” This In Focus article delves into the factors driving CMS’s decision and considerations for policymakers, Medicare Advantage Organizations and other interested stakeholders.
VBID Outcomes
VBID, run by the CMS Innovation Center, is not a permanent part of the Medicare Advantage (MA) program. Innovation Center models are required to be modified or terminated if they are a cost to the program.
CMS found that costs for the VBID model totaled $2.3 billion in calendar year (CY) 2021 and $2.2 billion in CY 2022, an unprecedent amount for an Innovation Center model. CMS concluded that these substantial expenses—driven by increased risk score growth and Part D expenditures—were unmitigable through policy modifications. Therefore, consistent with statutory requirements, CMS took action to terminate the model by the end of 2025. Earlier this year, CMS announced it would discontinue the part of VBID that allowed MA plans to offer hospice services.
Next year, the VBID model will have 62 participating MA plans and is projected to offer 7 million Medicare beneficiaries additional benefits and/or rewards, including those designed to address social determinants of health and reduce cost-sharing for prescription drugs used to treat and manage chronic conditions. As part of the announcement, CMS pledged to support a stable transition for all enrollees in MA plans participating in the MA-VBID model and emphasized that key benefits available under the model will continue to be widely available, including supplemental benefits that address the whole-person healthcare needs of beneficiaries. In addition, CMS noted beneficiary cost-sharing for prescription drugs will be reduced as the result of the expansion of the low-income subsidy program under the Inflation Reduction Act and the CMS Innovation Center’s Medicare $2 Drug List Model, which is slated to begin in 2027.
As part of the announcement, CMS released an executive summary of a forthcoming evaluation report, with the full report expected to be released in early 2025.
Key Considerations
Since the MA-VBID model’s launch in 2017, the program has experienced significant growth through a series of legislative and model changes, including requirements in the Bipartisan Budget Act of 2018 that expanded eligibility to MA plans in all 50 states and allowing all types of MA special needs plans to participate in MA-VBID. Previous CMS evaluations found that the MA-VBID model led to improvements in the quality of care for beneficiaries and promoted greater adherence to prescription drugs used to treat and manage chronic conditions. Though CMS has concluded that excess costs require the termination of MA-VBID by the end of 2025, the incoming Trump Administration can be expected to closely examine this decision and look at the entire Innovation Center portfolio.
Connect with Us
Health Management Associates, Inc. (HMA), Medicare experts will continue to assess and analyze the response to CMS’s announcement, including the incoming administration’s views on the decision and potential alternatives. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist MA organizations and interested stakeholders in analyzing and adapting to the marketplace as the MA-VBID program ends.
For further analysis of the MA-VBID decision and its impact on the market, contact our experts below.
Congress Continues Negotiations on 2025 Spending and End-of-Year Package
This week, our In Focus section reviews the year-end legislative package congressional leaders announced as part of the stopgap funding to prevent a government shutdown. The package, which was unveiled December 18, 2024, would extend expiring Medicaid and Medicare policies, reauthorize health and human services programs, and extend federal funding for discretionary programs through March 14, 2025. The existing temporary funding measure expires December 20, 2024.
Following is a summary of several major healthcare policies that, if approved, will inform the shifting federal policy landscape and state and local programs in 2025.
Pharmacy Benefit Managers
The healthcare package includes policies that reflect several years of increased scrutiny on pharmacy benefit managers (PBMs), including:
- Prohibiting PBMs from charging a Medicaid managed care organization more for a drug than the amount that a PBM pays a pharmacy (i.e., spread pricing)
- Requiring consistency and additional transparency in contracts between Part D plans and PBMs
- Prohibiting Medicare Part D plans from linking payments to drug list prices
- Adding report requirements for PBMs
Medicaid Policies and Programs
The legislative text includes 13 separate sections that address Medicaid policies, including extensions on expiring policies, establishment of new programs, and plans to codify certain other policies related to Medicaid eligibility and renewals. These policy changes include:
- Medicaid Disproportionate Share Hospital (DSH) allotment: Eliminates reductions for fiscal year (FY) 2025; delays the effective date of the two remaining years of Medicaid DSH allotment reductions until January 1, 2027; and changes the definition of the Medicaid shortfall component of the Medicaid DSH cap to include costs and payments for patients who have Medicaid as their primary source of coverage and for patients who are dually eligible for Medicare and Medicaid.
- Home and community-based services (HCBS) waiver: Establishes a three-year, five-state Medicaid HCBS waiver program, which would allow states to cover these services for individuals who need them but do not meet the current statutory requirement of needing “institutional level of care.” States will have an opportunity to apply for planning grants.
- Services for juveniles leaving public institutions: Delays by 12 months the requirement that state Medicaid programs provide screenings, diagnostic services, and targeted case management services for eligible juveniles within 30 days of their scheduled date of release from a public institution following adjudication.
Medicare Payments
The compromise package also increases the Medicare Physician Fee Schedule conversion factor by 2.5 percent in 2025 to partially offset a 2.83 percent cut that the Centers for Medicare & Medicaid Services (CMS) finalized in November. Providers consider this a short-term fix, however, and Congress, provider advocates, and other interested parties are engaged in discussions about making broader changes to Medicare physician pay in 2025.
Notably, the agreement includes a payment policy consistent with a bill that the House of Representatives passed earlier this year—the Lower Cost More Transparency Act—to provide enhanced information about payment differentials between off‐campus outpatient departments and other outpatient facilities. The provision requires each off-campus outpatient department to obtain and bill for services under a unique national provider identifier.
Other notable Medicare policies include:
- Telehealth: Extends Medicare telehealth flexibilities through December 31, 2026; establishes special rules for telehealth services provided by Federally Qualified Health Centers and Rural Health Clinics for prospective payment and all-inclusive rates; adds modifiers for telehealth services provided incident-to other services and those offered via contracts with virtual platform vendors; expands services that can be provided via telehealth; and enhances tracking of telehealth use
- Payment extensions: Extends the Medicare low-volume hospital payment adjustment and Medicare-dependent hospital program through December 31, 2025; Medicare ground ambulance add-on payments through December 31, 2026; incentive payments for advanced alternative payment models through payment year 2027 at an adjusted amount of 3.53 percent; and Qualifying Participant eligibility thresholds in effect for performance year 2023 through payment year 2027
- Hospital at-home program: Extends the Acute Hospital Care at Home initiative through December 31, 2029
- Part D: Prohibits cost sharing for generic drugs for Part D beneficiaries who are eligible for the low-income subsidy
- Provider directories: Requires Medicare Advantage plans to maintain accurate provider directories on a public website beginning in plan year 2027
- Screening: Adds multi-cancer early detection screening tests as a covered benefit beginning in 2029
- Home infusion: Allows coverage of home infusion treatments by classifying certain approved infusion treatments as Durable Medical Equipment (DME)
Other Notable Provisions
- Reauthorizes and revises the Second Chance Reauthorization Act of 2024, including allowing substance use disorder (SUD) services to be provided through the State and Local Reentry Demonstration Projects program
- Reauthorizes and modernizes several aspects of child welfare programs
- Provides mandatory funding for community health centers and the National Health Service Corps through FY2026, the Teaching Health Center Graduate Medical Education Program through FY2029, and the Special Diabetes Programs (SDP) for Type I diabetes and the SDP for Indians through FY2026
- Reauthorizes through FY 2029 the SUPPORT for Patients and Communities Act, which includes a range of mental health and SUD prevention, treatment, and recovery programs
- Reauthorizes Older Americans Act programs
- Reauthorizes several programs and authorities related to preparedness and response through FY2026, including the Public Health Emergency Preparedness Program and the Hospital Preparedness Program
What’s Next
Funding for the federal government expires December 20, 2024. Congress will need to approve another temporary measure to avert a government shutdown. The length and scope of such an extension remains under discussion, though the current continuing resolution would push the funding deadline into the first few months of the incoming Trump Administration and new Congress. Healthcare stakeholders, including payers, state and local governments, providers, and community organizations, should continue to monitor the congressional negotiations and be prepared to analyze the impact of legislation that Congress ultimately approves.
Connect with Us
Health Management Associates, Inc. (HMA) experts will continue analyzing the implications of the funding and policy updates in the December 18 package and ongoing congressional discussions to reach an agreement. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist organizations with navigating these changes and the impact for health and health adjacent sectors. Please contact Laura Pence and Andrea Maresca to connect with our experts.
MyCare Ohio: The Next Generation’s impact on the Ohio Medicare & Medicaid landscape
The transition of MyCare Ohio to the Next Generation of its program on January 1, 2026, marks a significant evolution in the way Ohio provides healthcare services to its dual-eligible population – those who qualify for both Medicaid and Medicare services. This evolution moves Ohio to a Fully Integrated Dual Eligible Special Needs Plan model (FIDE SNP) that aims to achieve several key goals through a population health approach, designed to address inequities and disparities in care for dual-eligible individuals. These goals include:
- Improved Care Coordination. Strengthening integration between Medicare and Medicaid services to provide seamless, holistic care for individuals, reducing fragmentation and ensuring comprehensive management of medical, behavioral, and social needs.
- Personalized Care. Utilizing data analytics and technology to create more tailored care plans, with a focus on proactive care to address the unique health needs of each individual, especially those with chronic conditions.
- Expanded Access to Services. Increasing accessibility, particularly through telehealth and digital tools, to reach underserved populations and improve convenience for patients, particularly those in rural or remote areas.
- Enhanced Quality of Care. Shifting focus from service volume to outcomes, encouraging providers to deliver high-quality care and improve patient satisfaction, while incentivizing preventive care to reduce hospital admissions and other high-cost interventions.
- Technology Integration. Leveraging advanced technologies like mobile apps, predictive analytics, and telemedicine to monitor patient health, improve communication between patients and providers, and enable more efficient care delivery.
The current MyCare program is offered in 29 counties across Ohio but will transition to a statewide program as a part of the Next Generation changes. Additionally, Coordination Only Dual Eligible Special Needs Plans (CO DSNP) will no longer be permitted.
After the Ohio Department of Medicaid (ODM) publicly released the request for applications (RFA) and evaluated submitted proposals, they selected four Managed Care Organization (MCOs) that will become the Next Generation MyCare plans. The ODM awarded the following MCOs to serve MyCare members beginning in January 2026: Anthem Blue Cross and Blue Shield, Buckeye Health Plan, CareSource, and Molina HealthCare of Ohio.
The shift to the FIDE SNP model and selection of four participating health plans will have a considerable impact on the competitive landscape for Medicare and Medicaid managed care in Ohio. The resulting changes can affect both selected and non-selected participants in different ways, including:
- Increased competition among chosen MyCare MCOs. MCOs will need to focus on enhancing their care coordination systems, adopting new technologies, and developing personalized care plans to compete not just on the volume of services provided but also on the quality and effectiveness of care. Those who can best integrate services, offer proactive care management, and improve patient outcomes through value-based care and advanced technology initiatives will gain the competitive advantage, potentially attracting more beneficiaries.
- Strategic responses of nonparticipating MCOs to counter potential membership and financial losses. MCOs that lose membership by not being selected, or are unable to offer CO DSNPs moving forward, will likely strategize how to gain membership through other product lines or benefit design to offset losses. Strategies may vary but could include tactics such as enhancing benefits or decreasing member cost shares to entice member movement across carriers for non-DSNP plans; finding innovative ways to further reach different segments within the Medicare population, such as Value Based Insurance Design (VBID) packages or Chronic SNP plays; or shifting focus to product lines outside of Medicare Advantage and Medicaid.
Ohio is one of many states transitioning to a FIDE model beginning January 2026. Health Management Associates (HMA) has successfully supported participating and non-participating carriers throughout the transition process and continues to be a dedicated partner to organizations navigating Medicare and Medicaid changes across the country. Contact one of HMA’s many experts for more details on how to navigate this evolution in health care.
Major changes to Medicare Advantage and Part D proposed by CMS for 2026
This week’s In Focus section examines a comprehensive proposed rule that the Centers for Medicare & Medicaid Services (CMS) released on November 26, 2024. These highly anticipated regulations—which represent the last major Medicare regulations from the Biden Administration—include several significant and far-reaching proposals designed to strengthen plan oversight and enhance beneficiary protections for millions of Medicare beneficiaries who have coverage through Medicare Advantage and Medicare Part D plans beginning in contract year 2026. The rule also comprises proposals with fiscal and policy implications for state Medicaid programs.
Comments on the proposed rule are due by January 27, 2025, and the incoming Trump Administration could make significant changes before finalization. New administration officials may choose to delay certain provisions, scale back, or eliminate certain proposed policy changes when they finalize the regulations next year.
This article explains several of the proposed policies, considerations for healthcare stakeholders, and developments that Health Management Associates (HMA) experts will be tracking in the coming weeks.
Coverage of Anti-Obesity Medications Under Medicare Part D and Medicaid
In the proposed regulations, CMS seeks to expand coverage of anti-obesity medications (AOMs) under the Medicare Part D and Medicaid programs. Under current Medicare Part D coverage rules, medications used exclusively for weight loss are excluded from the definition of a Part D covered drug. Through the proposed change, CMS is seeking to align Medicare and Medicaid coverage policy with the prevailing medical consensus that recognizes obesity as a chronic disease.
Under the proposed reinterpretation, CMS would expand eligibility for Part D coverage of AOMs for Medicare beneficiaries with obesity. AOMs used for weight loss or chronic weight management would continue to be excluded from Part D coverage under the proposed regulation.
As it relates to Medicaid, CMS’s proposed reinterpretation would require Medicaid coverage for anti-obesity medications when used for weight loss or chronic weight management for the treatment of obesity. State Medicaid programs would continue to have discretion to use preferred drug lists and prior authorization (PA) to establish certain limitations on the coverage of these drugs, consistent with existing statutory requirements.
CMS estimates the proposal would increase federal costs by $24.8 billion as the result of expanded Part D coverage and $14.8 billion because of expanded Medicaid coverage over a 10-year period.
Key considerations: Though expanded access to innovative medications may improve access and outcomes for obese patients, these considerations may need to be balanced against the proposal’s considerable fiscal costs. In addition, key health nominees put forth by President-Elect Donald J. Trump have different views about how best to prevent and treat chronic disease, creating additional uncertainty about whether this proposed expansion will go forward.
Strengthening Prior Authorization and Utilization Management Guardrails
The proposed rule includes a series of recommendations for reforming Medicare Advantage PA, utilization management (UM), and coverage decisions, which include:
- Defining the meaning of internal coverage criteria to clarify when MA plans may apply UM
- Ensuring MA plans’ internal coverage policies are transparent and readily available to the public
- Requiring plans to inform beneficiaries of their appeal rights
- Revising the current metrics for the annual health equity analysis on the use of PA to require more detailed and granular reporting to allow CMS to determine whether MA plans disproportionately deny certain services
Key considerations: Continued scrutiny of MA plans’ PA practices and strong bipartisan support for reforms increase the likelihood that certain changes will be made to these policies within the next year.
Enhancing Medicare Plan Finder to Include Information on Plan Provider Directories
Another notable proposal would require MA plans to make provider directory data available to CMS for inclusion in Medicare Plan Finder (MPF), the online tool that allows beneficiaries to compare coverage options, including Medicare Advantage and Part D plans. At present, provider directories must be accessible on MA plans websites.
CMS seeks to enhance MPF with searchable provider information for all MA plans while requiring plans to attest to the accuracy of the provider directory data, including updating data within 30 days of receiving notification that provider information has changed. CMS would ensure compliance with this expectation by requiring plans to meet data compliance and quality checks, which will be detailed in upcoming technical guidance.
Improving Access to Behavioral Health Care
The proposed rule furthers federal policymakers’ initiatives to address the nation’s behavioral health crisis. CMS proposes to establish the following three standards to ensure that beneficiary cost sharing in Medicare Advantage is no greater than in Traditional Medicare:
- A 20 percent coinsurance or an actuarially equivalent copayment rate for mental health specialty services, psychiatric services, partial hospitalization, and outpatient substance abuse services
- No cost sharing for opioid treatment programs
- All (100 percent) of the estimated Traditional Medicare cost sharing for inpatient psychiatric services
Improve Oversight and Administration of Supplemental Benefits
MA plans may offer a variety of supplemental benefits such as vision, dental, and gym memberships, which have come under increasing scrutiny by CMS. CMS proposed several actions to reduce misuse of these benefits, including:
- Outlining proper usage by MA organizations and enrollees
- Adding disclosure rules for transparency
- Ensuring enrollees can access covered services through alternative methods
- Requiring real-time electronic links between debit cards and covered services
- Defining acceptable over-the-counter products.
Key Considerations: CMS officials in President-Elect Trump’s first administration expanded flexibility for plans to offer supplemental benefits. Incoming policy officials may seek an opportunity to fully review the Biden Administration’s proposals. Data and experience-informed comments from MA plans and stakeholders can support such discussions.
Improve Care Experience for Dual Eligibles
CMS proposed the following two new federal requirements for Dual Eligible Special Needs Plans (D-SNPs) that are applicable integrated plans (AIPs):
- AIP D-SNPs will need to have integrated member ID cards for their Medicare and Medicaid plans.
- D-SNPs will be required to conduct an integrated health risk assessment for Medicare and Medicaid, rather than separate ones for each program.
Key Considerations: These proposals further CMS’s multi-year work to advance integrated care by applying Medicare-Medicaid Plan features into D-SNP requirements. States and MA and Medicaid plans should plan for operational and policy changes if the proposals are finalized.
Formulary Inclusion and Placement of Generics and Biosimilars
CMS proposes to require Part D formularies to provide beneficiaries with broad access to generic, biosimilar, and other low-cost drugs while also ensuring that tier placement and UM practices do not limit access to these drugs as compared with more expensive brand name and reference products.
Key considerations: If finalized, the proposal would require MA-PD and Part D plans to update their approach and considerations for plan formulary development. Consumer groups and other stakeholders should consider the possibility that the proposal will improve access to lower cost products.
Other Topics in the Proposed Rule
In addition, the proposed rule calls for the following:
- Guardrails for artificial intelligence to protect access to health services, such as requiring that MA plans ensure services are provided equitably, regardless of delivery method or origin (i.e., human or automated systems)
- Changes to MA and Part D medical loss ratio (MLR) reporting to improve the meaningfulness and comparability of MLR across plan contracts
- Expanded Part D medication therapy management eligibility criteria
- Adding and updating measures addressed in this proposed rule, beginning with the 2028 Star Ratings
- Promoting community-based services and enhancing transparency of in-home service providers, including new definitions and standards for community-based organizations
- Codifying existing guidance related to implementation of the Medicare Prescription Payment Plan, which is part of the Inflation Reduction Act (IRA)
What to Watch
During the lame duck session, Congress could advance legislation related to some proposals in this rule. Specifically, PA has been an area of significant bipartisan interest, along with access to and cost of GLP-1 products. CMS will need to ensure the final MA and Part D policy and technical rule for contract year 2026 reflects approved statutory changes.
In addition, HMA is watching key appointments within the US Department of Health and Human Services, including individuals selected to lead CMS’ Medicare and Medicaid centers. These appointments will provide valuable insights on the emerging policy agenda of the incoming administration.
Connect with Us
HMA’s Medicare and Medicaid experts will continue to assess and analyze the policy and political landscape, which will determine the final policies in the MA and Part D policy and technical rule for contract year 2026. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist organizations that engage in the rulemaking process and to support implementation of final policies, including policy development, tailored analysis, and modeling capabilities, as well as quality improvement initiatives and plan benefit design.
For further analysis of the MA and Part D proposed rule and potential impact on MA and Part D plans, Medicaid programs, providers, and beneficiaries, contact our featured experts below.

Has Medicare’s Drug Policy Struck the Right Balance Between Access and Cost?
Kevin Kirby, managing director at Health Management Associates, gives a closer look at the evolution of Medicare’s drug coverage and the policies that have transformed patient access and affordability. From Clinton era ideas, to the launch of the Medicare Modernization Act and then the Affordable Care Act, Kevin has advised clients as these significant milestones have shaped and reshaped Medicare’s drug benefits. He discusses the implications of the Inflation Reduction Act, raising important questions about sustainability and cost control. The episode will explore how these pivotal policies will impact access to treatment and the sustainability of Medicare in a rapidly changing healthcare landscape.