HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
This week, our In Focus section highlights the Health Affairs article, Advancing Health Equity and Integrated Care for Rural Dual Eligibles, authored by Ellen Breslin, Samantha Di Paola, Susan McGeehan, Rebecca Kellenberg, and Andrea Maresca, Health Management Associates.
A public health crisis is growing more acute in rural America, disproportionately impacting individuals with both Medicaid and Medicare (the “dually eligible”). The rural health crisis is a health equity concern that affects all rural residents, including dually eligible individuals. There are 47 to 60 million people residing in rural areas. Twenty-one percent of dually eligible individuals live in rural areas—that’s about 2.6 million people. Based on these numbers, the authors calculate that the dual eligible population residing in rural communities accounts for about 5 percent of the total rural population. Dually eligible individuals living in rural areas are at risk of falling through the cracks.
Dually eligible individuals lack access to adequate medical, behavioral health, home-and community-based services (HCBS) and other social services; those living in rural areas face even steeper challenges. Since dually eligible individuals are among the poorest of all individuals covered under Medicare, they are at significant risk of paying a steep rural mortality penalty.
With these challenges there are opportunities for innovation for the dually eligible population living in rural communities. The US can reverse the mortality-disparity rate trajectory. Public and private entities are interested in revitalizing rural America, confronting the rural health crisis, and harnessing the power of rural communities. Investment in the rural health care sector is essential given it is a major economic driver of rural communities.
HMA is creating a toolkit with actionable solutions to improve access to services and integrated care and health equity for individuals dually eligible for Medicare and Medicaid who live in rural areas across the country. This project is a follow-on project to a previous HMA project supported by Arnold Ventures. In 2021, HMA prepared a brief, Medicare-Medicaid Integration: Essential Elements for Integrated Care Programs for Dually Eligible Individuals, to increase and promote enrollment in integrated care programs (ICPs) meeting dually eligible individuals’ needs and preferences. Interviewees including dually eligible individuals helped HMA to identify “access to needed services in rural areas” as an essential element of ICPs. In response, HMA started a new project to create a toolkit with actionable strategies to improve access to needed services and improve integrated care opportunities, specific to dually eligible rural residents’ needs.
HMA designed the toolkit around four values: 1) rural health equity is an imperative for dually eligible individuals, 2) actionable solutions and innovations must come from the community, 3) there is no single pathway to integration, and 4) Medicare and Medicaid flexibilities are critical to inspiring innovations to advance health equity, access, and integration. The toolkit will provide actionable solutions for states with and without integrated care programs for dually eligible individuals to increase access to needed supports and services, care coordination, and integrated care programs. We expect that states and rural communities will use the toolkit as a foundation for mapping a holistic plan to advance access to care coordination and integrated programs for dually eligible individuals residing in rural communities. Other states may employ contractual tools listed in the toolkit to expand access to providers and new services; strengthen partnerships among entities serving the community such as community-based organizations, providers, and health plans; and increase community-wide accountability for meeting dually eligible individuals’ whole person-centered needs. The toolkit is scheduled for an early 2023 release.
Dually eligible individuals covered under Medicare and Medicaid living in rural areas struggle to access the services, care coordination, and integrated care programs they need. To address these needs, HMA conducted multi-state roundtable discussions with diverse stakeholders to create The Health Equity & Access for Rural Dually Eligible Individuals (HEARD) Toolkit. During this webinar, our experts summarized and discussed the toolkit’s actionable solutions for improving health and social outcomes for rural dually eligible individuals.
Learning Objectives:
Understand why the voices of rural dually eligible individuals must drive planning efforts to generate innovations and prioritize investments to advance independent living and recovery goals.
Learn how experiences shared from New Mexico, North Dakota, and Tennessee can offer lessons.
Explore eight actionable solutions for improving health and social outcomes among rural dually eligible individuals as outlined in the HEARD toolkit.
Understand why community engagement and investment in rural capacity are essential to improving access to services and integrated care programs for rural dually eligible individuals.
Speakers
Arielle Mir, Vice President, Health Care, Arnold Ventures
Expert Panelists
Dr. Kevin Bennett, Professor of Family Medicine, University of South Carolina School of Medicine, Director of the Research Center for Transforming Health, and Director of the South Carolina Center for Rural and Primary Care Dennis Heaphy, Health Justice Advocate and Researcher, Massachusetts Disability Policy Consortium, Co-Chair, One Care Implementation Council, a One Care member, and MACPAC Commissioner Pamela J. Parker, Medicare-Medicaid Integration Consultant, SNP Alliance Tallie Tolen, Long-Term Services and Supports Bureau Chief, Medicaid, New Mexico Human Services Department
Today’s blog is the next in our series highlighting significant developments in the Medicare program. In our first article we covered the Centers for Medicare and Medicaid Services’ (CMS) calendar year 2023 Medicare Physician Fee Schedule (MPFS) proposed rule. This week we are highlighting a few key policy developments in the proposed rule that governs payment levels and policy updates for hospital outpatient departments and ambulatory surgical centers (ASCs).
As we discussed last week, this is a pivotal moment for the Biden Administration’s Medicare policy agenda. Because the rulemaking cycle takes about 18 months, CMS needs to begin the process of collecting input on new proposals this year if it intends to finalize proposals before the end of the President’s first term. Additionally, the CY2023 rule represents an important transition year for CMS as it navigates the COVID-19 related anomalies in the data used to calculate payment levels.
Health care plans, providers, and facilities are continuing to transition to value based payment strategies, making it increasingly important to assess the entire environment of Medicare payment rules as these payment systems are the basis of financial benchmarks, quality incentives, and other key components of value-based payments. In addition, these payment rules provide insight into the cost pressures, incentives, and areas of misalignment throughout the health care system.
HMA experts are analyzing and closely tracking several issues in the CY 2023 hospital outpatient prospective payment system (OPPS) proposed rule. A brief summary of some of the most important proposed policy changes for the outpatient hospital setting are included below and highlight many of the Administration’s top health care priorities.
Policies to sustain access and address health disparities in rural communities.
Enhancing Medicare’s behavioral health payment and access policies beyond the COVID-19 public health emergency.
Uncertainty in the hospital outpatient prospective payment system (OPPS) rate increase due to future implementation of changes in 340B payment.
Increasing transparency of consolidation and mergers in the marketplace to help advance quality and affordability.
The remainder of our post delves into these issues and other notable proposals. Our post also includes analysis of the implications of these policies for stakeholders deserving.
Key Action Items for Stakeholders
The CY 2023 OPPS Proposed Rule was published on July 15, 2022, and all comments from stakeholders are due to CMS by September 13, 2022. We anticipate CMS will release their Final Rule in late fall 2022, before the new rules are implemented January 1, 2023.
The public comment period is also an important window of opportunity during which stakeholders can analyze the impact of CMS’s proposed policies, assess the proposals against other applicable pending federal and state payment policies, and consider how the proposals may impact business decisions. Further, the public comment period is essential for CMS to deepen its understanding of the impact of its policies on stakeholders. The agency benefits from hearing stakeholder’s perspectives, viewing their quantitative and legal analyses, and understanding the general stakeholder environment.
Rural Emergency Hospitals: Definition and Payment
The Consolidated Appropriations Act of 2021 (CAA) established a new provider type called Rural Emergency Hospitals (REHs) beginning in 2023. REHs are facilities that convert from either a critical access hospital (CAH) or a rural hospital with less than 50 beds, by choosing to close their inpatient capacity. Instead, these facilities provide emergency department services, outpatient services, post-hospital extended care services, and other defined services.
While the statute specifies many foundational aspects of REHs, CMS was given the authority to further define REH eligibility status and to specify the unique reimbursement mechanisms for REHs. All of these components will be vital to a provider or entity’s decision to pursue REH status.
On June 30, CMS released the first component: Conditions of Participation (CoPs) for REHs, which defined REH status within the Medicare program. Within the CY 2023 OPPS Proposed Rule CMS proposed to define reimbursement and several other key components of REHs. Below we detail the key elements of REH reimbursement. In HMA’s blog next week we will offer greater detail on the COP and reimbursement policies.
REH policies proposed in the CY 2023 OPPS Proposed Rule:
REHs will receive a monthly facility payment of approximately $268,000 (or more than $3 million per year) beginning in CY 2023.
REHs will receive a 5 percent payment increase for all services covered under the Medicare OPPS.
REHs may provide outpatient services that are not otherwise paid under the OPPS (e.g., the Clinical Lab Fee Schedule) as well as post-hospital extended care services furnished in a unit of the facility that is a distinct part of the facility licensed as a skilled nursing facility (SNF).
Beneficiaries served at REHs will not be charged a copayment on the additional 5 percent OPPS payments, but standard OPPS cost-sharing requirements would still apply.
REHs must comply with all applicable provider enrollment provisions in order to enroll in Medicare.
REHs will have a unique quality reporting program distinct to REHs, in order to reduce reporting burden on these smaller facilities. CMS seeks feedback from stakeholders on the measures used for the REH quality reporting program.
REHs will be provided an exception from the Physician Self-Referral Law (commonly known as the “Stark Law”).
Takeaway: The creation of REHs is both a significant change for the Medicare program and potentially a unique opportunity for small rural hospitals and health systems which own/operate rural hospitals. The Congress and CMS believe this model will address access to care concerns and health disparities present in rural communities. Many assert that under the REH approach, hospitals and health system providers serving rural communities may have greater flexibility to support the rural communities they serve.
Look for our additional analysis of the set of proposed REH policies next week.
Mental Health Services Furnished Remotely by Hospital Staff
For CY 2023, CMS proposes several updates to its remote services policy to plan for a transition from temporary policies enacted during the PHE to when the PHE is declared over. CMS proposes to:
Allow clinical staff of a hospital to conduct remote mental health and substance abuse services and to designate these services as hospital outpatient department services for purposes of reimbursement. Patients will be permitted to be in the homes and hospital clinical staff must conduct the service from inside the hospital facility. Further, CMS proposes new hospital outpatient codes for these services, and CMS will not permit these outpatient services to be conducted (and billed) in tandem with physician fee schedule services.
The agency will require an in-person service within 6 months prior to the initiation of the remote service and then every 12 months thereafter. CMS will allow exceptions to the in-person visit requirement based on beneficiary circumstances.
The agency is also proposing that audio-only interactive telecommunications systems may be used to furnish these services when the beneficiary is not capable of, or does not consent to, the use of two-way, audio/video technology.
Takeaway: As CMS wrote in the proposed rule, many beneficiaries may be receiving mental health services in their homes from hospital or critical access hospital staff during the COVID-19 PHE. The policy update could help minimize disruptions in continuity of care that might otherwise occur following the end of the PHE. The proposals also reflect CMS’ desire to adapt to changing beneficiary preferences and new methods of providing services that have evolved during the COVID-19 PHE.
Hospitals and health systems may benefit from these proposals because it will maintain and expand patient-provider access points and care coordination after the patient has left the hospital. Stakeholders will need to continue to assess beneficiary utilization of services furnished remotely, potential staffing changes to support these services, and community-specific access needs for remote mental health services. Stakeholders may have important perspectives to offer CMS through the regulatory comment proceed as the agency determines whether to finalize a requirement that hospital clinical staff be physically located in the hospital when furnishing services remotely using communications technology.
Payment Policies
CMS is proposing to update OPPS payment rates for hospitals and ASCs that meet their respective applicable quality reporting requirements by 2.7 percent. This update reflects the following factors:
Projected hospital market basket percentage increase of 3.1 percent; and
A 0.4 percentage point reduction for projected multifactor productivity.
In the context of the OPPS, CMS proposes to increase the OPPS conversation factor by 2.7 percent from CY 2022 to CY 2023, from $84.18 to $86.79. CMS estimates this will increase OPPS payments to providers from CY 2022 to CY 2023 by $1.8 billion.
In the context of ASCs, CMS estimates a proposed increase to the ASC conversation factor by 2.7 percent from CY 2022 to CY 2023, from $49.91 to $51.31. CMS estimates this change will increase industry-wide payments from CY 2022 to CY 2023 by $130 million. In addition, CY 2023 is the final year in which CMS will apply the productivity-adjusted hospital market basket update to ASC payment system rates for an interim period of 5 years (CY 2019 through CY 2023).
Consistent with CMS’s methods for updating other Medicare prospective payment systems during the 2023 regulatory cycle, the agency proposes to use claims data from CY 2021 and hospital cost report data from the June 2020 Healthcare Cost Report Information System (HCRIS) to update payment rates for CY 2023. Some stakeholders have expressed concern during this regulatory cycle that claims data continue to include anomalous trends influenced by covid cases and the cost data do not accurately reflect covid-related costs because the data primarily are associated with pre-COVID time period.
340B Payment Policy
CMS’s proposed rule acknowledges the recent Supreme Court decision in American Hospital Association v. Becerra (No. 20-1114, 2022 WL 2135490), which will have a significant impact on the 340B program. However, given the recency of this decision the agency formally proposed to maintain the current payment rate of Average Sale Price (ASP) minus 22.5 percent for drugs and biologics acquired through the 340B program.
In response to the decision, CMS stated that the agency will adjust 340B payment rates within the CY 2023 final rule. In its recent ruling, the Supreme Court held that HHS may not vary payment rates for drugs and biologicals among groups of hospitals without having surveyed hospitals’ acquisition costs. The decision relates to payment rates for CYs 2018 and 2019 but has implications for the CY 2023 rates.
CMS also stated that it anticipates applying a 340B payment rate of ASP plus 6 percent for specified drugs and biologics in the CY 2023 final rule. This would likely result in a budget neutrality reduction approaching 5% in the OPPS conversion factor.
Takeaway: Hospitals and federally qualified health centers (FQHCs) receiving 340B reimbursements will view the court ruling and potential increase to 340B payment rates as positive. However, it remains unclear at what exact level 340B payments will be set. Therefore, stakeholders may want to comment on the CY2023 policy options CMS is considering. Additionally, stakeholders should plan for CMS to conduct a survey of acquisition costs as it considers newly proposing changes to the payment rates. It remains possible that CMS will continue to apply the 340B cut for 2023 in light of a 2020 survey of hospital acquisition cost that it conducted. Future budget neutrality adjustments may also be necessary for any payments that are returned to hospitals due to the overturning of the 340B cut for 2018 and 2019.
Additional Issues for Stakeholder Consideration
In addition to the financing and policy issues discussed above, the wide-ranging rule contains numerous other policy proposals with direct and indirect implications on Medicare providers, beneficiaries, and other stakeholders. Table 1 provides a snapshot of some of the issues that warrant further consideration.
Table 1. Other Notable Proposed Changes Impacting Health Care Providers and Stakeholders
Topic
Summary
Provider Transparency
CMS issues a request for information linked to the President’s July 2021 Executive Order (E.O.) on Promoting Competition in the American Economy. CMS currently manages a database of nursing homeowners and operators, and the agency has begun to leverage that data to support hospital and nursing home patients and their families. The agency solicits feedback on whether it should release additional data that is already being collected “to help identify the impact of provider mergers, acquisitions, consolidations, and changes in ownership on the affordability and availability of medical care.” CMS also invites comments on whether the agency should release similar data for other types of providers. The solicitation represents the next phase in CMS’ expansive portfolio of work to address the impact of market consolidation on health care prices, consumer costs, and quality in the healthcare industry writ large. Medicare providers and stakeholders should be tracking how federal health care regulators, including CMS, are working to respond to the E.O. There is a strong likelihood that CMS will begin to include data on other types of providers and stakeholders will need to understand this shifting landscape and how it could impact their current and potential future business decisions.
SaaS
CMS discusses its desire to address the novel and evolving nature of Software as a medical Service (Saas) procedures. The agency is seeking comments on the specific payment approach we might use for these services under the OPPS as SaaS-type technology becomes more widespread. We are also concerned about the potential for bias in algorithms and predictive modeling, and are seeking comments on how we could encourage software developers to prevent or mitigate the possibility of bias in new applications of this technology.
Inpatient Only List
Removes ten services from the Inpatient Only (IPO) list.While the IPO list has previously been targeted for major reforms, this year’s narrower set of proposed changes signal CMS’ is deprioritizing IPO list reform.
Payment for surgical N95 Respirators
CMS recognizes that hospitals may incur additional costs when purchasing domestic NIOSH-approved surgical N95 respirators. CMS is proposing payment adjustments under the IPPS and OPPS that would reflect, and offset, the additional marginal resource costs that hospitals face in procuring domestically made NIOSH-approved surgical N95 respirators. Under this proposal, these payments would be provided biweekly as interim lump-sum payments to the hospital and would be reconciled at cost report settlement. The rule outlines the information providers need to include on the cost report to determine payments for cost reporting periods beginning on or after January 1, 2023.
Ambulatory Surgery Centers
CMS requests stakeholder feedback on methods that could be implemented to collect cost data from ASCs that minimize reporting burden.This could be the beginning of a process to implement cost reports for ASCs.
The HMA Medicare team will continue to analyze these proposed changes. We have the depth and breadth of expertise to assist with tailored analysis, to model policy impacts, and to support the drafting of comment letters to this rule.
On June 30, 2022, the Centers for Medicare & Medicaid Services (CMS) released a proposed regulation establishing the Conditions of Participation (CoPs) for a new hospital provider type, Rural Emergency Hospitals (REHs). The REH concept was first developed by the Medicare Payment Advisory Commission (MedPAC) and subsequently mandated by Congress through the Consolidated Appropriations Act (CAA) of 2021 to address the growing concern over closures of rural hospitals.
REHs provide an opportunity for Critical Access Hospitals (CAHs) and rural hospitals to improve the way care is delivered in their communities, maintain access, and avert potential closure by choosing to focus on the service offerings that are most essential to their communities, such as emergency services, observation care, and additional medical, behavioral, and maternal outpatient services. Importantly, the REH concept enables facilities to maintain a hospital designation absent inpatient capacity thereby ensuring that rural communities retain access to services. This proposed regulation is a significant milestone in CMS’ work to implement the REH designation and their novel payment methodology by their mandated start date of January 1, 2023.
The REH concept is expected to help address the observed health inequities that arise when rural communities lack access to hospitals and other providers. Obtaining an REH designation could be an opportunity for many independent hospitals and delivery systems to strategically reshape themselves in line with their community’s needs while receiving payments from Medicare for doing so.
Within CMS’ proposed regulation, the agency proposes to establish a novel set of REH CoPs which will define the parameters of the REH designation. The REH CoPs closely align with the current CAH CoPs in most cases, while considering the uniqueness of REHs and the statutory requirements. In some instances, the proposed REH policies closely align to the current hospital and ambulatory surgical center standards, such as the polices for outpatient services’ requirements and life safety code, respectively.
As a part of this proposed regulation, CMS seeks input from the rural community on a few key aspects of the REH designation, including:
The specific proposed REH standards, including the ability of an REH to provide low-risk childbirth-related labor and delivery services and whether the agency should require REHs to provide outpatient surgical services in the event that surgical labor and delivery intervention is necessary.
Whether it is appropriate for an REH to allow a physician, physician associate, nurse practitioner, or clinical nurse specialist, with training or experience in emergency medicine, to be on call and immediately available by telephone or radio contact and available on site within specified timeframes.
Updates to CoPs for Critical Access Hospitals
Also within this draft regulation CMS proposes to update the CoPs for CAHs by: (1) adding a definition of primary roads to the location and distance requirements; (2) establishing a patient’s rights CoP; and (3) allowing CAHs that are a part of a larger health system (containing other hospitals and/or CAHs) to unify and integrate their infection control and prevention and antibiotic stewardship programs, medical staff, and quality assessment and performance improvement programs (known as QAPI) to ensure consistent and safe care.
What’s Next
CMS is accepting comments on this rule until August 29, 2022. CMS intends to propose additional policies related to Medicare enrollment, payment, and quality reporting in the upcoming Calendar Year 2023 Outpatient Prospective Payment System/Ambulatory Surgery Center proposed rule. CMS will develop final policies for this program later this year.
For more information about this proposed regulation including how to submit comments and how the REH concept may impact the hospital industry and patients in rural communities please contact our Medicare team who have knowledge in Congressional, MedPAC and CMS policy and operations featured below.
A life sciences manufacturer was seeking approval for a new formulation of an existing drug and needed to better understand reimbursement issues facing this new formulation under Part B of the Medicare program.
BACKGROUND
The HMA Medicare team was asked to apply our subject matter expertise—and access to Medicare claims information—to provide a fully formed picture of the reimbursement process for this new drug formulation. Our work involved researching other precedents and the implications of those precedents for the reimbursement of this new formulation, as well as the existing product.
APPROACH
HMA’s Medicare team has significant expertise in helping life sciences manufacturers understand and address the policy challenges affecting market access of new drugs and biologics. A key aspect of the Medicare’s team’s expertise is their ability to understand how various policies interact, causing unexpected outcomes. For this client, we helped educate various internal stakeholders on the pricing implications for their new formulation—and its legal and regulatory issues that could cause the pricing for their new product to be blended with the prior version of the product, potentially creating access problems because of the required higher numbers of units for the new formulation. Our work was aided by research into local coverage documents by Medicare administrative contractors—and analysis of claims data to provide evidence for the hypothesis that coverage for the new formulation could be available under Medicare Part B’s coverage of physician services, even though the prior formulation is covered under the pharmacy benefit.
RESULTS
Conventional wisdom in product development teams often paints an incorrect and outdated picture of the policy environment. HMA’s expert consultants can provide appropriate context to aid these teams in their planning as new products get closer to market, because of their work to monitor and understand up-to-the-minute changes to the policy landscape. Some reimbursement challenges can be mitigated or eliminated if they are addressed early enough in the development process for new technologies. Once certain approval pathways are set, it may no longer be possible for manufacturers to avoid a link between the prices of different formulations of a drug.
The HMA Medicare team was able to educate the client about Medicare’s intricate reimbursement rules, where the same drug, but a different formulation may be reimbursed under different rules. Rather than focusing on the various reimbursement silos, we provided a holistic view of the drug reimbursement landscape, so the client was able to understand that factors such as how many patients are able to self-administer the drug will affect the ultimate reimbursement for both the new and old formulation.
A major pharmaceutical manufacturer was preparing to launch a new oncology drug. This drug, a self-administered oral drug with a multi-week dosing regimen, was provided through the pharmacy benefit. The client was concerned about patients not being able to access the drug at hospitals and in post-acute care settings, where institutions received bundled payment for the care.
BACKGROUND
Bundled payment can serve as a disincentive to provide high-cost drugs, so the client was interested in pursuing reimbursement policy options that would ensure appropriate reimbursement to these facilities, thus ensuring patient access to the drug during the treatment regimen.
APPROACH
HMA helps physician associations, device manufacturers, and drug companies understand billing practices, reimbursement challenges, and patient outcomes, enabling them to make informed decisions.
For this analysis, the client wanted to learn about the likelihood that patients receiving their cancer treatment would be admitted to the hospital and then to other post-acute settings during the treatment window. Using our in-house library of Medicare claims data including claims for inpatient, outpatient, physician office, skilled nursing facility, home health, and other post-acute settings, we tracked patients with the specific cancer from diagnosis forward for several months. We were able to see how often patients were hospitalized, what prompted the hospitalization, how many were discharged for post-acute care, and how long treatment continued.
Our analysis provided data-driven insights that supported the client’s strategic decision-making and planning. Using the information from our claims analysis and overlaying the typical treatment regimen under the new cancer drug, the client was able to determine where their patients might face barriers to treatment. For example, most drugs provided in the inpatient setting are bundled into the payment the hospital receives, giving hospitals a disincentive to provide higher cost drugs. While the number of patients receiving their drug that would likely be admitted to the hospital during the treatment period was not high, the company wanted to remove as many barriers to access as possible, and is now considering pursuing a new technology add-on payment (NTAP) for the drug when used in the inpatient setting. The claims analysis also found that some of the cancer patients of interest receive home health care during the treatment window, but since patients are able to continue to receive drugs through their pharmacy benefit while also receiving home health care, the patients would be able to continue their oncology treatment. The patient journey analysis allowed the company to focus attention on settings where access could potentially be disrupted, to ensure that patients are able to continue their cancer treatment.
RESULTS
We identified patients with this specific type of cancer and tracked these patients to see how often they accessed different care settings and identified any potential reimbursement challenges. We further analyzed the volume of patients of interest receiving care in each setting and calculated the average cost per user within the approximate dosing regimen. This allowed us to identify any reimbursement risks for the drug associated with each care setting. Armed with concrete information on the treatment path of these oncology patients, the client was able to make an informed decision about whether to pursue an NTAP for inpatient use of their drug. The company was also able to educate providers and patients providing information on both the benefits of the new treatment, and the reimbursement scenarios in the various care settings.
A coalition of CAR T manufacturers and their trade association joined together to advocate for appropriate reimbursement of Chimeric Antigen Receptor T-cell (CAR T) therapies. They requested that policy options be developed by non-partisan experts that would best benefit the industry making the drugs, Medicare and Medicaid programs paying for the treatments, and the Medicare beneficiaries receiving these transformative therapies.
BACKGROUND
CAR T therapies first entered the market in late 2018. These transformative treatments for certain types of cancer involve modifying a patient’s own cells to fight the cancer—producing a long term, potentially curative response. Initially, CAR T therapy was administered to patients in the inpatient hospital, where Medicare payments are bundled so that the hospital gets a single payment for the entire hospital stay. The cost of the CAR T therapy greatly exceeded the payment rate the hospital would receive, leading to concerns that hospitals would be reluctant to provide CAR T.
APPROACH
The emergence of CAR Ts represented a new reimbursement problem that required very careful consideration because these new treatments were just the beginning of a series of new, expensive, but essentially curative treatments. Solving the CAR T problem would have implications for the future, as other new therapies entered the market. Finding the right solution involved a real rethinking of the inpatient payment system. The client had to recognize how CAR T cases were similar to past precedents — and how some key differences about these cases required fundamental changes to how these cases are paid. Solving CAR T access and reimbursement issues required different types of expertise and approaches. The client needed a very deep understanding of the intricacies of the payment system, as well as a broad view of the policy landscape to find the right balanced response.
The HMA Medicare team had two vital sets of skills that were necessary for the work. First, we have an in-house library of Medicare claims and the data analysis skills needed to use the data to answer policy questions. This includes our model of the Inpatient Prospective Payment System (IPPS) rate setting and payment methodologies, so we could model the policies as they stood, as well as alternative policies to explore which options maximized the goals of the coalition members while minimizing negative outcomes. Second, we have a deep understanding of the policy issues at play, the history of the policy space, and the understanding of the interplay between many policy factors.
HMA worked with the coalition to monitor Medicare claims to get an accurate picture of the hospitals performing CAR T therapy and the payments they were receiving. We also explored how potential changes to the IPPS could provide better reimbursement for CAR T cases. Using our expert-level understanding of the intricacies of the payment methodology, we modeled many different policies to pinpoint the option that would balance the need for more appropriate payments with the needs of the rest of the system—understanding that there was a pipeline of additional CAR T therapies poised to enter the market in the coming years. This process also involved communicating with the policymakers at the Centers for Medicare and Medicaid Services (CMS) to ensure that the policies being advanced were politically viable and sustainable.
RESULTS
The work culminated in the creation of a new payment category for CAR T cases, with changes to the typical rate setting and payment methodology to account for both clinical trial and non-clinical trial cases. In addition, the work of the coalition prompted CMS to increase payments in the New Technology Add-on Payment program for all products, not just CAR T therapies. As a result, patient access to CAR T therapies has been maintained, and CMS has a framework to work from as new cell and gene therapies become available to Medicare patients. We have seen the volume of CAR T claims increase more than 9-fold over the 6 years the therapies have been available.
At the urging of the CAR T coalition and other stakeholders, CMS created a new MS-DRG (payment category) for CAR T claims, bumping the base payment rate for the cases from ~$40,000 to ~$240,000. In addition, NTAP payments increased from a maximum of 50% of the cost of the product to 65% of the cost of the product—this applies for all NTAP eligible claims, not just CAR Ts.
This work involved years of analysis and collaboration that is continuing. While inpatient reimbursement has improved, concerns are arising now around access to CAR T in the community setting.
The Nevada Division of Health Care Financing and Policy (DHCFP) engaged HMA to evaluate Nevada’s Medical Assistance for the Aged, Blind, and Disabled (MAABD) program and the needs of its participants. A targeted focus of the evaluation was on home and community-based services (HCBS) within the Nevada MAABD population, including Nevada’s Frail Elderly (FE) and Physically Disabled (PD) waiver.
The project included:
Data analyses of Nevada’s population and long term services and supports (LTSS) landscape, the state’s ongoing efforts to rebalance LTSS dollars from institutional to HCBS services and demographic and other information about the MAABD population
Stakeholder engagement, including three focus groups that engaged 55 stakeholders and individual interviews, to provide stakeholders a greater voice in the MAABD improvement process
Evaluation of the MAABD structure and administration
Program recommendations to help inform and guide DHCFP’s considerations for better serving the FE and PD MAABD populations throughout the state
The report made recommendations to enroll the MAABD population aged 65 and older into a combination MLTSS/FIDE-SNP (managed long-term services and supports/fully integrated dual eligible special needs plan) program, implement Program of All-Inclusive Care for the Elderly (PACE) as a targeted nursing home diversion strategy and strengthen Nevada’s Medicaid quality framework to better deliver and ensure improved quality of care for the MAABD population.
Over the past decade, the U.S. has seen significant federal and state policy initiatives to improve and expand assistance for the millions of family members who help care for older adults, and those who support people with intellectual and developmental disabilities (I/DD) across the lifespan. The pandemic, combined with workforce shortages, accelerated these efforts. In this webinar with national family caregiving experts, we discussed policy and practice advances and their potential impact on enabling more Americans to live at home and in the community.
Learning Objectives:
Review evidence that supporting family members improves outcomes for older adults and people with I/DD.
An overview of current federal and state implementation of the 2022 National Strategy to Support Family Caregivers and the 2022 National Agenda for Supporting Families with a Member with I/DD.
Share evolving opportunities for improving policy and practice in family caregiving initiatives.
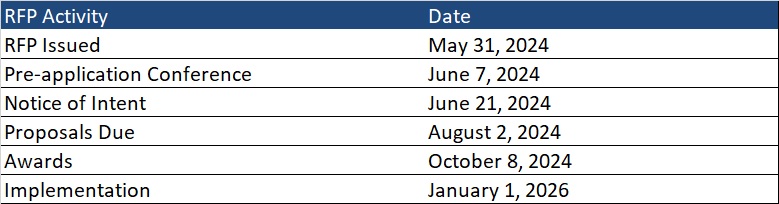
This week’s In Focus section delves into the Next Generation MyCare Ohio managed care program, spotlighting the request for applications (RFA) that the Ohio Department of Medicaid (ODM) released on May 31, 2024. The MyCare Ohio Program, which serves people who are dually eligible for both Medicaid and Medicare, is undergoing a substantial transformation. Transitioning from the financial alignment initiative (FAI) demonstration model used in 29 counties, it is evolving into a statewide, fully integrated dual eligible special needs plan (FIDE-SNP) model. This shift is more than procedural; it signifies a pivotal moment of transition to new federal D-SNP requirements.
Background
The MyCare Ohio Program launched in May 2014 as a Centers for Medicare & Medicaid Services (CMS) FAI demonstration. MyCare Ohio integrates Medicare and Medicaid benefits for dually eligible members enrolled in competitively selected MyCare Ohio managed care plans, providing one care coordinator and streamlined communication and services. It serves 150,000 individuals in 29 counties.
CMS is sunsetting all FAI demonstration programs on December 31, 2025, prompting ODM to convert to the FIDE-SNP model.
Next Generation RFA
The MyCare Ohio Program will convert to the Next Generation MyCare Ohio Program in January 2026. ODM is modeling portions of the program after the state’s Next Generation Medicaid managed care program. The Next Generation MyCare Ohio Program initially will be implemented in the 29 currently participating counties and then expand statewide, covering a total of 250,000 eligible individuals. Medicaid managed care organizations (MCOs) that serve the program will need to become CMS-approved FIDE-SNPs. MCOs awarded a Next Generation MyCare Ohio contract will need to notify CMS of their intent to establish a statewide FIDE-SNP in Ohio by fall 2024 to begin operations in January 2026.
ODM anticipates selecting up to four Next Generation MyCare Ohio MCOs to serve enrollees statewide, though a decision on the number of plans will be finalized as awards are made and based on what is most advantageous to the state.
MCOs will need to develop a member-focused strategy with care coordination as a priority. MCOs will also increase focus on behavioral health coordination. According to ODM, goals for the Next Generation program include:
Focusing on the individual
Improving individual and population wellness and health outcomes
Creating a personalized care experience
Supporting providers in continuously improving care
Improving care for people with complex needs to promote independence in the community
Increasing program transparency and accountability
Next Generation MyCare will advance these goals through a population health approach, designed to address inequities and disparities in care.
The program will enroll dually eligible individuals ages 21 and older. This is a change from the current program, which enrolls dual eligibles who are 18 years old and older. The eligible age increase is being made to align with the Medicaid early and periodic screening, diagnostic, and treatment (EPSDT) benefit.
The new program also will continue to offer all the same services available through Ohio’s home care, PASSPORT (long-term services and supports), and assisted living waivers.
Evaluation
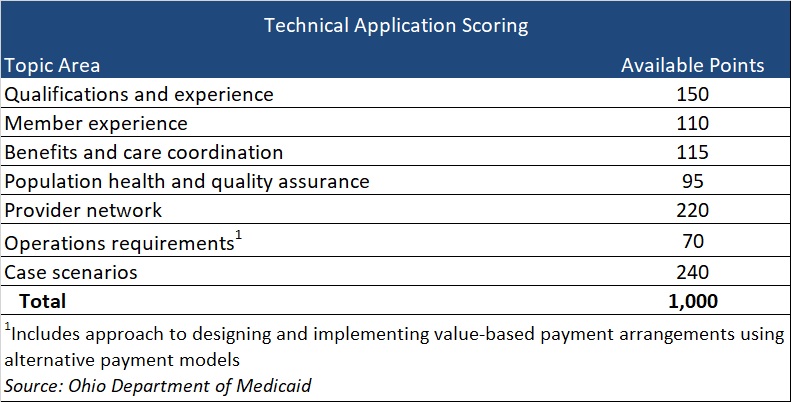
Applications initially will be reviewed to confirm the applicant meets the mandatory requirements. Applicants who meet the mandatory requirements will proceed to review and evaluation of responses to application questions that fall into seven topic areas, with a total of 1,000 available points (see Table 1). Of note, if an applicant is not currently serving as either a Next Generation MCO or a MyCare Ohio MCO, the applicant will receive zero points for qualifications and experience. Organizations that have yet to participate in at least one of these programs should consider the effect on their total score.
Table 1
Current Market
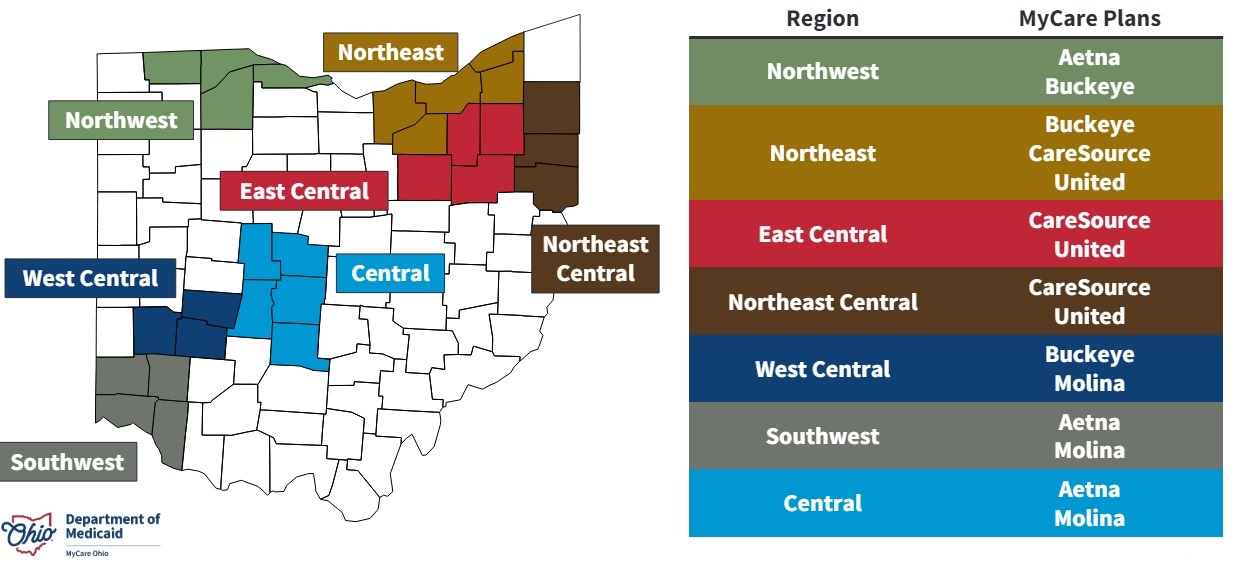
Five MCOs—CVS/Aetna, CareSource, Centene/Buckeye, Molina, and United—participate in the current MCOP, with two or three of them participating in each of the seven regions.
Timeline
MCOs should submit a notice of intent to apply by June 21. Proposals are due August 2, and awards will be issued October 8. Implementation is scheduled for January 1, 2026.
Ohio is one of several states transitioning from a FAI demonstration at the end of December 2025. Additionally, the 2025 Medicare Advantage Final Rule includes new policies affecting D-SNPs that could reshape the integrated care plan landscape in many states.
Health Management Associates (HMA) will host a webinar on June 20, 2024 titled “D-SNP growth and integration: key implications of the 2025 CMS final rule” to review the current landscape and federal changes that will affect D-SNPs in 2025 and beyond. The session will feature an analysis of the new regulations and a discussion of the critical strategic and product impacts on Medicare organizations that offer D-SNPs or are considering offering D-SNPs. Attendees also will have the opportunity to engage with the panelists during a Q&A session. Watch the replay now.
Contact our experts below for details about the nationwide D-SNP rules and landscape.
Watch our informative webinar where HMA experts reviewed the upcoming changes from the 2025 Final Rule that will impact Dual Special Needs Plans (D-SNPs) in 2025 and beyond. The session featured an analysis of the new regulations and a discussion of the critical strategic and product impacts on Medicare organizations offering D-SNPs or considering offering D-SNPs. Attendees also had the opportunity to engage with the panelists during a Q&A session.
Learning Objectives
Understand the impact of the 2025 Final Rule on D-SNPs as CMS promotes the integration of Medicare and Medicaid for dually eligible individuals.
Gain a high-level understanding of the federal changes, the timelines for implementation, and the impact on your D-SNP strategy and growth opportunities.
HMA recently released a report on the Medicare Physician Fee Schedule (PFS) with background on the structure of the program, and recommendations for reforms that could be considered. This webinar provided background and context about the PFS for interested parties who may be less familiar with the payment system and why the stakeholder community got to the point of needing to “fix” the fee schedule. We discussed pressing policy and payment concerns, provided an overview of key structural issues within the PFS that should be considered and balanced when making policy changes to the payment system, highlighted different stakeholder perspectives, and offered recommendations within CMS authority.
Learning Objectives:
Understand the background, context and function of the PFS including its relationship to other payment systems.
Highlight key policy developments over time leading to the current focus on “fixing” the payment system.