The Medicare Stars program is a year-round endeavor for Medicare Advantage (MA) plans. That being said, all MA plans intensify their Stars campaign during the fourth quarter of each year. The most important aspect of the fourth quarter push is to know where to focus. MA Star ratings are more than a quality score—they shape the financial and operational success of MA plans.
Some measures may no longer apply in the fourth quarter. Once the Consumer Assessment of Healthcare Providers & Systems (CAHPS) survey has been completed, the fourth quarter becomes a time to continue the effort to enhance and improve consumer experience for next year’s CAHPS survey. For example, post discharge follow-up is time limited and going back to earlier quarters is not possible. Adherence measures work similarly; if a member has already lost 80% of days covered, coverage cannot be made up during the fourth quarter. The message should be “focus only on measures where you can make a difference.”
Mammograms and colorectal exams can occur any time of year. These two measures should definitely be the focus of a fourth quarter push. A constraint may be provider capacity since all MA plans are focused on the same measures. Measures with low denominators like the osteoporosis management measure may be an important element in fourth quarter strategies.
Star Ratings and Operational Excellence
Operational excellence begins with robust, accurate, and actionable data, and even using lean six sigma principles to drive process improvement. Advanced analytics platforms are needed to aggregate and analyze vast amounts of healthcare data and operational data. Accurate risk adjustments, quality measurement, and operational metrics like appeals are essential. Data discrepancies or delays result in penalties, lower Star ratings, and incorrect payments. MA plans must develop processes to validate via quality assurance process and audit data regularly against CMS requirements.
Operational excellence also relies on a well-trained engaged workforce. Training should focus on fostering a culture of continuous improvement, where every team member is aligned with the organization’s goals of improving quality and operational performance.
Star ratings are a byproduct of strategic, data-driven approaches to care management, quality improvement, and operational efficiency. Success lies in the ability to optimize data integrity, streamline care coordination, and proactively resolve member concerns.
Accelerating Star Rating Performance
The HMA Stars Accelerator Solution offers a comprehensive, results-oriented approach to Star Rating performance improvement that addresses the multifaceted challenges faced by health plans and makes sure that your intensified 4th quarter effort is productive. The HMA Stars Accelerator Solution analytics provides information to plans about prioritizing measures during the fourth quarter push. It examines your plans leadership structure, operational processes, technology, reporting, member-centric engagement, provider partnerships, and develops a strategy for your organization using a data-driven approach for continuous improvement. Multiple “what-if” scenarios are developed that identify top priorities. Measure thresholds that are too far to reach are replaced by measures that are within reach during the final months of the year. The Accelerator approach includes “all-hands-on-deck” – care coordination, customer service, network development, marketing, analytics, and others. Accelerator plans introduce provider and member incentives and/or fee schedule adjustments to increase interest. These plans also provide information to providers on those attributed members who have measure gaps to facilitate provider outreach that is coordinated with plan outreach.
As the fourth quarter push occurs in the middle of the Annual Enrollment Period, lessons learned can be applied immediately. The HMA team can backstop your organization during this very busy time, avoiding missed opportunities. The fourth quarter push does not end until midnight January 31st of each year.
The HMA Stars Accelerator Solution will create a permanent change in your organization that is designed to yield a 4-star rating or higher each year. The Accelerator is a cultural transformation designed to strengthen star performance. Click here to learn more about the HMA Stars Accelerator Solution’s capabilities, where you can request a copy of the HMA Stars Accelerator Playbook. Let’s have a conversation about how your fourth quarter push is designed and unfolding.
We are also holding two webinars that may be of interest:
Falling Stars: Who’s Who in the 2025 Star Ratings
November 7, 2024 – 3:30 PM ET
Register now
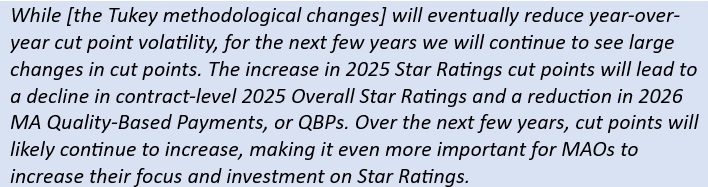
Colleagues from Wakely Consulting Group, an HMA Company, will discuss trends in Overall Star Ratings, the appeals and lawsuits filed in response, and future changes to the Star Rating program that are likely to depress Star Ratings even further over the next few years.
Mastering Star Performance: Strategies from the HMA Stars Accelerator Program
November 13, 2024 – 12:00 PM ET
Register now