
February 25, 2026
Outlook 2026: Medicare Advantage Advance Notice—What It Means for the 2027 Market
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
Outlook 2026: Medicare Advantage Advance Notice—What It Means for the 2027 Market

This webinar was held on March 11, 2026 at 12pm ET.
This webinar offered a timely, strategic overview of the recently released proposed 2027 Notice of Benefit and Payment Parameters and what it signals for the evolving coverage landscape. We unpacked the key policy changes, operational requirements, and market assumptions embedded in the rule, with a focus on implications for the individual and small group markets beginning in 2026 and extending beyond.
Participants gained insight into how proposed updates may affect plan design, rate development, risk adjustment, enrollment operations, and health insurance regulation dynamics. We also explored the broader policy direction reflected in the proposal and what organizations should be monitoring now to prepare for implementation and potential downstream impacts.
Learning Objectives:
You can also download the related Wakely Summary of Provisions in HHS’s Proposed 2027 Notice of Benefit and Payment Parameters and Other Key Regulations

On February 11, 2026, the Congressional Budget Office (CBO) released The Budget and Economic Outlook: 2026 to 2036 report. The publication, which represents the first time CBO has released Medicare and Medicaid spending baseline projections since January 2025, reflects the impact of the 2025 Budget Reconciliation Act (P.L. 119-21, OBBBA), recent changes to Medicare reimbursement for skin substitute products, and the latest Medicare Part D and Medicare Advantage bids.
CBO’s baseline serves many functions, including serving as the official “scorekeeping” benchmark used for cost estimates of proposed legislation under consideration in Congress.
Changes to CBO’s Medicaid Baseline
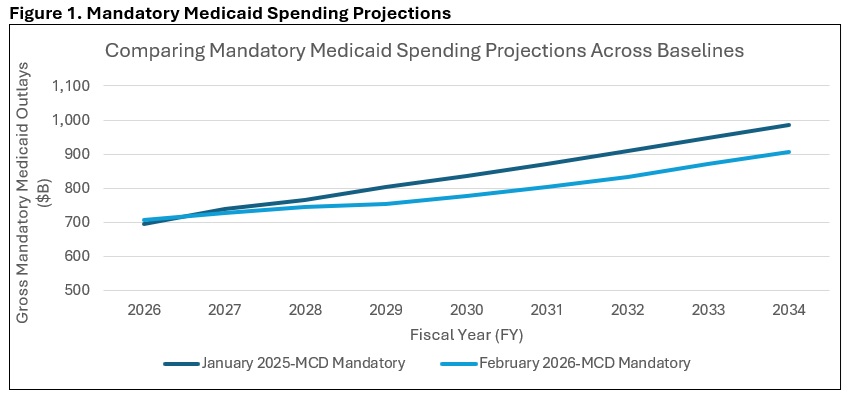
CBO decreased its projections of 2026–2035 Medicaid mandatory outlays by approximately $514 million from its January 2025 baseline update. The main driver of that reduction is the impact of the Medicaid provisions in the 2025 Budget Reconciliation Act, which CBO expects will reduce total Medicaid enrollment by 13.1 million people in 2035. The drop in Medicaid spending from the OBBBA-related enrollment reductions was partially offset by technical changes CBO made to the Medicaid baseline.
Medicaid costs per enrollee grew by 16 percent in 2025, which was more than CBO had anticipated. The agency attributes the cost per enrollee growth to a reported decrease in the average health status of Medicaid enrollees following the end of the COVID-era continuous eligibility policy.
CBO anticipates that payment rates for Medicaid managed care plans will begin to rise in 2026 because of this decrease in the average health status of enrollees, and the agency has updated the Medicaid baseline accordingly (see Figure 1).
Changes to CBO’s Medicare Baseline
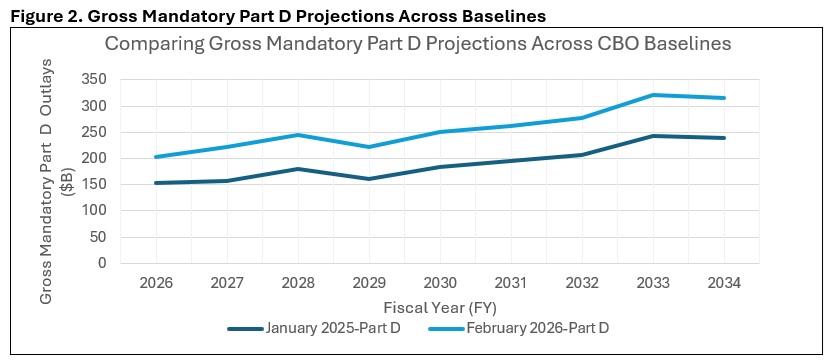
Compared with its January 2025 baseline, CBO increased its projections of Medicare’s 2026–2035 mandatory outlays by about $1 trillion (roughly $942 billion, by Health Management Associates (HMA) calculations). The main driver of that increase came from CBO’s updates to its Medicare Part D spending projections, which were increased to reflect higher than expected 2026 bids from private insurance plans that administer the Part D benefit. According to their 2026 bids, Part D plans anticipate a 35 percent increase in their annual per enrollee costs in 2026—a trend that CBO was not expecting and wants to study further. Part D spending per beneficiary in 2035 is now projected to exceed $4,000, up from less than $3,000 in the January 2025 baseline (See Figure 2).
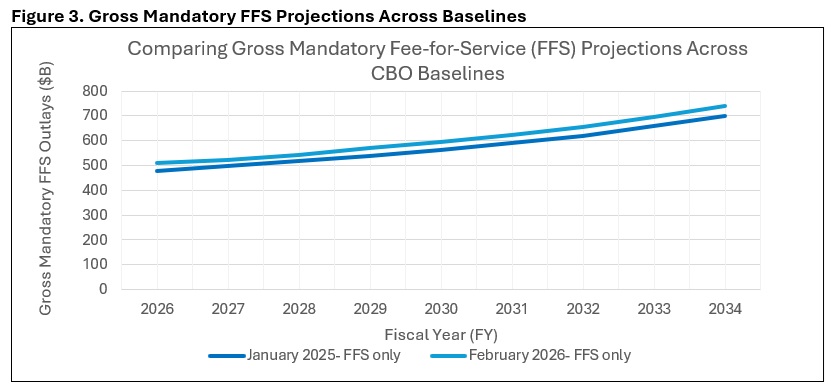
The agency’s Medicare Part A fee-for-service (FFS) spending projection increase was the result of larger than expected increases in 2025 enrollment and per enrollee spending. Those trends were also seen in Medicare Part B FFS but were partially offset by the Centers for Medicare & Medicaid Services’s (CMS) recent reimbursement changes to skin substitute products. Overall, CBO estimates that the skin substitute reform issued in CMS’s Medicare Physician Fee Schedule (MPFS) and Outpatient Prospective Payment System (OPPS) CY 2026 final rules will save $245 billion over the 2026–2035 period, including the effects on the Medicare Advantage (MA) program (see Figure 3).
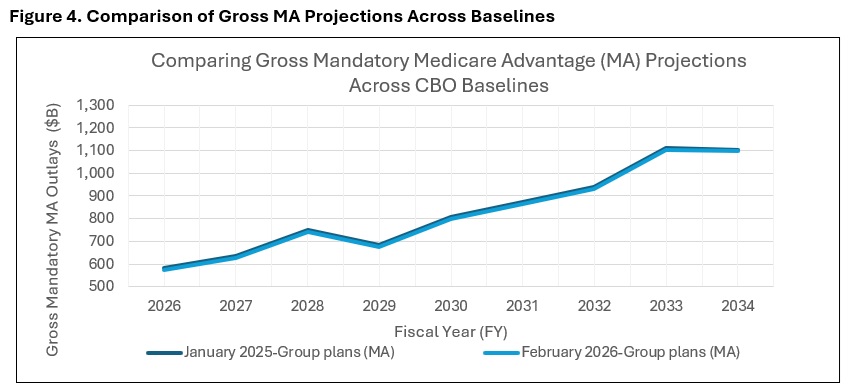
Finally, CBO reduced its spending projections for MA compared to the January 2025 baseline. This change was made to reflect lower-than-expected Medicare Advantage enrollment in 2025, although the spending implications of lower enrollment were partially offset by higher-than-expected bids in 2026 by providers of MA plans (see Figure 4).
Contact an HMA Expert Today
Interested in understanding how CBO’s latest baseline update affects the federal budgetary implications of certain Medicare or Medicaid policy topics or proposals? Contact our experts, Mark Desmaris and Rachel Matthews, to learn more about HMA’s “CBO-style” federal budgetary scoring work, which relies on The Moran Company’s long-standing methodology. [1]
Beyond federal budget scoring, HMA is working with states, health plans, and providers to assess how changes in enrollee health status are affecting utilization, costs, and payment rates—and what those trends may mean for Medicaid and MA organizations and providers. Our teams support states in evaluating managed care rate setting and program design, help Medicaid and MA plans anticipate risk and bid implications, and assist providers in understanding how changes in patient acuity could affect care delivery, contracting, and financial performance.
[1]Specifically, we apply our understanding of CBO precedents to predict how CBO will likely evaluate the budgetary impact of the legislation in question. We use our best judgment to adopt the assumptions CBO would tend to use, with the understanding that any variance in the assumptions CBO ultimately adopts could cause our estimate to differ from theirs.
Updates on Federal Funding for Rural Communities through the Rural Health Transformation Program
The Long View
On December 29, 2025, The Centers for Medicare & Medicaid Services (CMS) announced the highly anticipated funding awards to states for the Rural Health Transformation Program (RHTP)—a five-year, $50 billion federal initiative designed to stabilize and transform rural health systems across the country. This new federal investment marks a pivotal moment for states and their partners to address long-standing challenges in rural healthcare while laying the foundation for broader transformation. It provides an opportunity to reimagine care delivery, strengthen infrastructure, and build sustainable models that address entrenched gaps in rural health.
Directing Resources to Rural Communities
RHTP is designed with a focus on rural communities, where residents face persistent challenges such as provider shortages, hospital closures, and limited access to care. RHTP investments will support infrastructure development, IT system implementations and trainings, workforce recruitment and retention, and innovative care models tailored to rural community needs. The long-term goal is to create lasting capacity and resilience in rural health systems and promote better health outcomes for residents.
But the vision doesn’t stop there.
Catalyzing Statewide Transformation
While rural communities are the primary beneficiaries, we believe the impact of the RHTP will extend beyond rural borders. The program’s design encourages states to develop initiatives that can serve as pilots and start-ups, creating scalable solutions that can be adopted statewide. Workforce development programs, for example, may begin by focusing on rural providers and community health workers (CHWs) and training these individuals but, over time, strengthen the healthcare workforce across entire states and regions.
Much of the federal funding will enable states and their partners to invest in technology modernization, telehealth expansion, and integrated care models. These improvements assuredly will enhance access and quality for rural residents. And these same technologies can be deployed to enhance efficiency and coordination across entire health systems, laying the groundwork for broader system transformation and health improvement. The focus on chronic care management and innovative care arrangements has the potential to improve outcomes for all populations.
Collaborative Pathways for States and Partners
States and their partners—including health systems, community-based organizations, and technology innovators—have a valuable opportunity to collaborate on initiatives. In our review of state applications and the initial wave of state driven funding solicitations, we identified efforts to tackle long-standing system challenges, including:
Looking Ahead
RHTP is more than a funding stream. It is a catalyst for innovation and collaboration, providing an important avenue to address the chronic inequities in quality, access, and outcomes that people living in our nation’s rural communities often experience. But it also could foster improvement statewide. Program evaluation and performance monitoring of the small, community-based programs and the large-scale, multi-site, multi-year initiatives will provide insights that inform strategic decision-making at the local, state and federal levels. By scaling effective rural health-focused initiatives and investing in new and feasible tools, strategies, and programs, states can create models that improve care delivery for all their residents in the future. This is a moment for states, providers, and partners to think big and design programs that deliver lasting impact.
Health Management Associates (HMA) offers support to state agencies, health systems, and community partners shaping rural-first pilots that are designed for scalability—from maternal and perinatal care networks, EMS community care models, caregiver and CHW pipelines, to telehealth modernization and behavioral health integration. Our rural expertise and our unique ability to combine expertise in clinical, operational, policy, and data reforms for care improvement are well-suited to the goals of RHTP.
With the RHTP funding advancing to state partners early in 2026 and annual recalculations of state awards tied to performance, the time to design rural pilots that become statewide programs is now.
For questions about the RHTP opportunities for your organization and the solutions HMA can tailor to meet the needs of your state, contact Kathleen Nolan and Andrea Maresca.
Connecting the Dots: A new blog series for 2026
Connecting the Dots is a monthly HMA blog series that brings together insights from our experts to examine the major policy, program, and market forces shaping healthcare coverage, delivery systems, and financing in 2026. The posts look beyond individual changes, instead connect emerging developments across programs and markets to help leaders understand what’s changing, why it matters, and how their decisions shape the path ahead.
The Centers for Medicare & Medicaid Services (CMS) issued a memo January 27, 2026, with updates on the agency’s approach to checking whether Medicare Advantage (MA) plans are being paid correctly. These reviews are conducted through Risk Adjustment Data Validation (RADV) audits, which help CMS confirm that the diagnoses MA plans report are supported by medical records.
The January 2026 memo signals that CMS intends to honor its commitment to strengthen oversight of MA payments, including accelerating and expanding the use of RADV audits and using AI (artificial intelligence) to streamline human coding reviews. MA organizations must now prepare to respond to the RADV audit notice within the required five-month window, while balancing their other risk-adjustment programs.
In this article, we explain the rapidly evolving landscape affecting RADV audits. Wakely, an HMA company, addresses what these changes mean for MA organizations and key considerations to ensure they are prepared for the upcoming enhancements to federal program integrity initiatives.
Overview of CMS’ RADV Refresh
CMS announced a major shift in May 2025: All MA plans will undergo RADV audits—not just a small sample as before. These audits look for cases in which diagnosis information submitted by a plan does not match the documentation in the patient’s medical record. When this happens, CMS may decide the plan was overpaid and require repayment. Historically, CMS audits have identified widespread diagnosis-code documentation errors, resulting in significant revenue recoupment from MA plans.
The 2025 announcement creates a framework for additional risk for MA plans, which could shift to risk-bearing provider groups. As we explained in an earlier article, key components of that announcement include:
Both the use of extrapolation and the removal of the FFS adjuster were later challenged in court.
Legal Challenge
In September 2023, Humana sued CMS in federal court, arguing that the 2023 RADV final rule, which allowed extrapolation and removed the FFS adjuster, was put into place without following proper federal rulemaking procedures. On September 25, 2025, the court agreed with Humana and vacated certain parts of this final rule, meaning certain parts of the rule are no longer in effect.
CMS appealed the ruling on November 1, 2025, which has created uncertainty about how RADV audits will work in future years.
Navigating the Legal and Regulatory Changes in Early 2026
The court did not say that extrapolation or elimination of the FFS adjuster is illegal—only that CMS did not follow the required process for changing the rules. Hence, the 2023 RADV final rule cannot take effect unless CMS wins its appeal or reissues the policy using the proper steps.
In its January 2026 Health Plan Management System (HPMS) memo, CMS stated that it will comply with the order while it is in effect.
The pending litigation does not diminish CMS’s broader commitment to increased audit activity and heightened scrutiny of MA risk-adjustment practices.
Effect of the Ruling. During RADV audits, CMS selects a sample of enrollees and requests corresponding medical records from the MA plan. These records are reviewed to confirm that the documented diagnoses meet CMS requirements. If unsupported diagnoses are found, CMS may recalculate payments and recover overpayments from the health plan. This audit process maintains program integrity and ensures accurate payments.
Plans that submit incomplete records could owe significant repayments to CMS.
CMS’s January 2026 memo clarifies how the agency plans to roll out additional RADV audits starting with PY 2020. CMS also addresses the agency’s plans to:
Preparing for What’s Next
Given CMS’s stated direction and the still unsettled litigation environment, MA plans should remain vigilant and audit ready.
Key steps include:
Connect with Us
Wakely assists plans with their RADV initiatives and development of robust RADV playbooks. For more information about Wakely’s RADV playbooks, contact Debbie Conboy.

This report synthesizes insights from multiple efforts to support the financial sustainability of HealthySteps sites in California, including federally qualified health centers (FQHCs), community clinics (non-FQHCs), private practices, and other settings. Led by the HealthySteps National Office and Health Management Associates (HMA), the technical assistance (TA) elevated challenges, strategies and best practices to achieve sustainability informed by learning collaboratives, individualized TA sessions, and financial modeling exercises. This report complements additional resources that the HS National Office and HMA developed which are available via the HealthySteps (HS) Sustainability website.
On February 3, 2026, Congress finalized federal funding for fiscal year (FY) 2026, with the House passing the Consolidated Appropriations Act (CAA), 2026, with a vote of 217-214, following Senate approval last week. The president signed the CAA (H.R. 7148) shortly thereafter. The law provides full-year appropriations for the Departments of Health and Human Services (HHS), Housing and Urban Development, Labor, and several other departments.
This year’s HHS funding bill is notable not only for what it includes, but also for what it omits. It restores or maintains funding for key public health and research agencies previously proposed for elimination in the president’s FY 2026 budget request, extends several healthcare programs, and contains a significant package of pharmacy benefit manager (PBM) reforms. All of this activity comes as the Administration announces new grant programs and policy efforts related to its signature priorities.
In this article, we review the major funding and policies approved in the HHS spending bill. We also address key considerations for healthcare organizations as they anticipate downstream funding and policy developments and develop advocacy initiatives for federal FY 2027 bills.
HHS Funding Levels and Direction
The bill provides $116.8 billion for HHS, an increase of $210 million over FY 2025, and rejects large-scale structural reorganizations proposed in the president’s FY 2026 budget. This provision preserves funding for the Agency for Healthcare Research and Quality (AHRQ), Centers for Disease Control and Prevention (CDC), Health Resources & Services Administration (HRSA), and the Substance Abuse and Mental Health Services Administration (SAMHSA)
Table 1. HHS Agency Funding Highlights, FY 2026
| Agency | FY 2026 Funding | (+/-) Compared with FY 2025 |
| Administration for Strategic Preparedness and Response (ASPR) | $3.7 billion | +$58 million |
| CDC | $9.2 billion | level funding |
| Centers for Medicare & Medicaid Services (CMS), administrative expenses only | $3.7 billion | level funding |
| HRSA | $8.9 billion | +$415 million |
| National Institutes of Health (NIH) | $48.7 billion | +$929 million |
| SAMHSA | $7.4 billion | +$65 million |
The bill also extends mandatory funding for community health centers, special diabetes programs, the National Health Service Corps, and Teaching Health Center Graduate Medical Education.
PBM Reforms in the Package
In one closely watched area of federal policymaking, the FY 2026 package includes a substantial set of PBM-related reforms that largely mirror the bipartisan package negotiated but not enacted in December 2024. These reforms have implications across Medicare Part D, commercial insurance, and employer-sponsored plans.
The legislation contains the following PBM reforms:
These provisions position 2026 as a consequential year for PBM regulation, increasing transparency, strengthening plan leverage, and heightening HHS oversight.
Healthcare Extenders and Program Reauthorizations
The bill includes a broad set of Medicaid, Medicare, and public health program extenders, affecting providers, patients, states, and managed care plans.
Medicaid
Medicare
Congress extends several key programs and payment provisions, including:
Behavioral Health Policy
The appropriations bill was finalized as the administration announced new funding and policy initiatives to support behavioral health, crisis services, workforce expansion, and youth mental health—efforts mirrored in SAMHSA’s increased appropriations.
SAMHSA’s $7.4 billion budget includes:
Considerations for Stakeholders
Federal funding and policy developments affect state budget dynamics as many states are now releasing 2026–2027 budget proposals as well as the operational and growth plans of healthcare organizations and partners.
A few key takeaways from the FY 2026 funding bill include:
Connect with Us
If you would like deeper analysis or state and stakeholder-specific effects, HMA’s policy experts are available to assist.
On January 28, 2026, the Centers for Medicaid & Medicare Services (CMS) released its second national snapshot of 2026 Affordable Care Act (ACA) Marketplace Open Enrollment (OE) activity. While this update is not a final accounting of enrollment activity, it is likely to be the last OE federal data release for some time and offers an early look at how enrollment trends are shifting in the wake of expired enhanced premium tax credits and new eligibility standards under the 2025 budget reconciliation act (P.L. 119-21, OBBBA).
In this article, Health Management Associates (HMA) and Wakely, an HMA company, highlight findings from their analysis of the 2026 OE activity and compare this activity with 2025 data. This analysis builds on the findings in their January 2026 analysis (here) and will provide important context for the 2027 plan year.
Overall Enrollment Trends
CMS reports that 2026 plan selections decreased by 5 percent from 2025, with enrollment declining across both new and returning consumers. New sign-ups dropped by 14 percent and renewals fell by 3 percent (Table 1). State-based Marketplace (SBM) enrollment dipped modestly, though many SBMs were still enrolling consumers in late January.
Table 1. Comparison of 2026 and 2025 Open Enrollment
| 2026 | 2025 | Net Change | |
| Total | 22,973,219 | 24,166,491 | (1,193,272) |
| New Consumers | 3,382,189 | 3,938,907 | (556,718) |
| Returning Consumers | 19,591,030 | 20,227,584 | (636,554) |
Variation Across State-Based and Federally Facilitated Marketplaces
Enrollment patterns varied substantially across states.
SBMs:
Federally Facilitated Marketplace (FFM) States:
What This Tells Us—and What It Doesn’t Tell Us Yet
FFM data are as of January 15, 2026, and measure plan selections after the OE period ended. Within the FFM, state-by-state enrollment activity varied significantly. Some of this variation is surprising and not readily explainable from the available data and will be a focus of future HMA and Wakely analyses.
The data include neither effectuated enrollment nor paid enrollment—data which will be key to fully understanding 2026 enrollment trends and the impact of changing federal policies, including the ePTC expiration and changing eligibility standards introduced in 2026 as the result of OBBBA.
Early SBM data suggest significantly higher cancellation and disenrollment rates than in previous years.
SBMs are sharing that they expect substantial affordability-driven voluntary and nonpayment terminations over the first half of 2026.
Monitoring paid enrollments, attrition, and grace period dynamics, including retro-terminations, will be key to understanding market dynamics and 2027 pricing.
Connect with Us
HMA and Wakley experts have considerable experience working with states, insurers, and federal policymakers with jurisdiction over the Marketplace. We work with these entities to inform, analyze, and shape federal policies and conduct impact analyses on pricing, enrollment, administration, and operations. HMA also provides strategic and project management support for the implementation of finalized policies.
Please contact Michael Cohen, Taylor Gehrke, or Zachary Sherman with questions, follow-up, or if you would like expert assistance exploring any of the issues discussed in this post.
On January 28, 2026, the Centers for Medicaid & Medicare Services (CMS) posted a national snapshot detailing 2026 Open Enrollment (OE) results. Although this report is neither a complete nor final picture of 2026 Marketplace enrollment activity, it is likely to be the last OE data CMS publishes for some time. A comparison of 2026 and 2025 Open Enrollment results can be found in Table 1.
Table 1. Comparison of 2026 and 2025 Open Enrollment
| 2026 | 2025 | Net Change | |
| Total | 22,973,219 | 24,166,491 | (1,193,272) |
| New Consumers | 3,382,189 | 3,938,907 | (556,718) |
| Returning Consumers | 19,591,030 | 20,227,584 | (636,554) |
A summary of our analysis on these 2026 OE results and how they compare with 2025 data can be found below. This analysis builds on the findings in Wakely’sIndividual ACA Open Enrollment Insights So Far from January 2026.
HMA and Wakley experts have considerable experience working with states, insurers, and federal policymakers with jurisdiction over the Marketplace. We work with these entities to inform, analyze, and influence federal policies and conduct impact analyses on pricing, enrollment, administration, and operations. HMA also provides strategic and project management support for the implementation of finalized policies.
Please contact Taylor Gehrke at [email protected], Michael Cohen at [email protected], or Zachary Sherman at [email protected] with questions, follow-up, or if you would like expert assistance exploring any of the issues discussed in this post.
Related Resources: