1314 Results found.

The New Uninsured: State Policy Options for Californians Losing Medi-Cal Coverage
HMA’s new report for the California Health Care Foundation explains how recent federal and state policy changes could cause up to two million Californians to lose Medi-Cal coverage. These changes will place new strains on the state budget and safety-net system. The report outlines practical short-term program paths California could use to preserve access to care while full-scope coverage is restored. It summarizes the policy and fiscal context (including work requirements, more frequent eligibility checks, and immigrant eligibility restrictions), describes stakeholder-informed design goals (statewide access, privacy protections, fiscal prudence, scalability, and safety-net stability), and presents two illustrative coverage alternatives with modeled cost ranges and key trade-offs in benefits, provider payment rates, cost sharing, and bridge-period design.

Outlook 2026: A Conversation on Medicare Draft Payment Rules
As the Centers for Medicare & Medicaid Services (CMS) advances through the 2027 Medicare payment rule cycle, stakeholders across Medicare Advantage (MA) and the provider community are assessing how proposed changes could affect payment, utilization, and longer-term revenue. To better understand what to watch as draft rules move toward finalization, Jen Colamonico, Vice President, Strategy and Communications at Health Management Associates (HMA), caught up with Rachel Stewart, Senior Consulting Actuary with Wakley, an HMA Company. Of particular interest was CMS’s decision to eliminate the Inpatient Only List (IPO) over a three- year period.
Q: As CMS begins releasing draft payment rules for 2027, what stands out most to you from a budgetary perspective?
Rachel: Timing and uncertainty really stand out. These policies don’t operate in isolation. Changes to Medicare fee-for-service (FFS) payment ultimately affect Medicare Advantage benchmarks, provider contracting, and long-term revenue expectations. Because bids, budgets, and contracts are set before rules are finalized, modeling different scenarios becomes essential.
Q: One issue that has garnered significant interest is CMS’s decision to phase out Medicare’s Inpatient Only (IPO) policy, which is a list of procedures and services that must be provided on an inpatient basis. In 2026, CMS eliminated nearly 300 services, mostly musculoskeletal services, from the IPO list. How are Medicare Advantage plans thinking about the Inpatient Only list specifically?
Rachel: Historically, many MA plans have followed the IPO policy even though they weren’t required to do so, largely because it simplified operations and aligned with Medicare fee-for-service payment systems. Plans do have flexibility in how they contract with providers, and we see a wide range of approaches in the market. Some contracts closely mirror FFS, while others incorporate more customized arrangements or risk sharing. Because of that, the direct impact of IPO changes will vary significantly across plans and provider relationships.
Q: Where do you see the biggest potential impact for Medicare Advantage?
Rachel: I think the bigger impact may be indirect rather than tied to individual contract changes. Medicare Advantage benchmarks are driven by underlying fee-for-service spending trends. If CMS anticipates lower overall inpatient spending as procedures move to outpatient or ambulatory surgical center settings, that expectation could show up in benchmark growth rates. Even relatively small changes in benchmark growth can affect plan revenue, rebates, and benefit flexibility.
Q: Are you already seeing signs of that in the data?
Rachel: We do see lower inpatient trends reflected in the 2027 and 2028 US per capita cost projections. It’s still unclear what’s driving those trends—whether its assumptions related to the IPO list removal or other factors. We’ve asked CMS for more clarity. From an actuarial standpoint, understanding what’s baked into those projections is critical, because so many MA financial decisions flow from them.
Q: How does this uncertainty affect provider planning, especially for hospitals?
Rachel: Providers are understandably concerned about potential revenue shifts if cases move out of the inpatient setting. But in Medicare Advantage, the picture is more nuanced than in fee-for-service. Many MA arrangements include risk sharing, medical loss ratio targets, and quality incentive payments. If overall costs decline, providers may share in savings through those mechanisms. So, while there may be pressure on inpatient revenue, it’s not necessarily a one directional loss.
Q: Does that mean the overall impact may be less dramatic than it appears?
Rachel: Potentially, yes—especially for organizations already participating in value-based arrangements. A reduction in unit costs doesn’t automatically mean a reduction in total provider revenue in MA. The redistribution of dollars through shared savings and quality bonuses can offset some of that pressure. That’s why understanding contract structure is just as important as understanding the policy itself.
Q: What about quality and patient safety as procedures move to lower cost settings?
Rachel: Quality is always central in Medicare Advantage, and plans are already managing a lot of complexity related to Star ratings and quality measurement. We haven’t yet seen specific quality safeguards tied to the IPO list changes, but I would expect more discussion in the forthcoming proposed rules. From the MA side, contracting remains a key lever. Plans still have flexibility to ensure procedures are performed in appropriate settings and to align incentives with quality outcomes.
Q: What steps do you recommend to stakeholders to prepare for the final rule and for 2027?
Rachel: Modeling helps organizations understand the range of possible outcomes rather than betting on a single assumption. We’re looking at different utilization scenarios, site of care shifts, and benchmark growth trajectories. For providers, modeling can inform contract negotiations and capital planning. For plans, it helps assess revenue risk and benefit design flexibility. It doesn’t eliminate uncertainty, but it helps organizations make informed decisions.
Q: If you could change one thing about how these policies are rolled out, what would it be?
Rachel: Transparency. The more clarity CMS can provide around cost projections and assumptions—especially those affecting benchmarks—the better positioned actuaries, plans, and providers will be to respond. So much of Medicare Advantage pricing relies on understanding how fee-for-service is expected to evolve. Greater transparency helps everyone plan more responsibly.
HMA’s Medicare Practice Group Can Help
As CMS moves closer to finalizing the 2027 payment rules, actuarial modeling will continue to be an important tool for translating policy direction into financial strategy. For MA plans and providers alike, early analysis and scenario planning can help mitigate risk and identify opportunity as Medicare’s payment landscape continues to evolve.
For additional insights, listen to Rachel Stewart and Zach Gaumer on HMA’s Vital Viewpoints podcast. Learn more about our Medicare services and solutions.
Early Signals from a Pivotal ACA Enrollment Year
On April 15, 2026, Wakely Consulting Group, an HMA company, published “Who Paid, and Who Stayed? Early 2026 Enrollment Trends in the Individual Market,” the first comprehensive nationwide look at 2026 enrollment trends in the Affordable Care Act (ACA) market. While the Centers for Medicare & Medicaid Services (CMS) has released 2026 plan selection data, the Wakely report addresses who retained coverage and who did not, what we still don’t know, and what we should be watching for throughout the rest of the 2026 plan year.
This article highlights key findings in the report, related state-level data, impacts and takeaways, and actions states and other interest-holders should consider as they look to mitigate further coverage losses and address market stability in& plan year 2027 and beyond.
Key Findings from the ACA Marketplace Early Enrollment Trends Report
The Who Paid, and Who Stayed report is based on analysis of data from the Wakely National Risk Adjustment Reporting (WNRAR) project, which includes summary data from participating ACA-compliant individual market plans. WNRAR includes data from over 75 issuers representing nearly 80 percent of enrollment the individual market. Key national findings in the report include:
- Only 86% of enrollees paid their January 2026 premium.
- State variation is significant, ranging from as low as 63% paid in January to as high as 99%.
- The overall average enrollment decrease is estimated to be between 17% and 26% lower than 2025, with morbidity projected to worsen by 2.9–6.5%.
The report highlights shifts in plan choice activity driven by affordability pressures, which resulted in considerable migration away from richer benefit plans to plans with lower premiums and higher out-of-pocket maximums. Examples include:
- Silver plan enrollment fell approximately 17% from 2025.
- Bronze enrollment increased by more than 10%.
- More than 13% of 2025 Gold plan enrollees selected a lower priced, Bronze tier plan in 2026.
The report also demonstrated the importance and value of outreach, operational excellence, and state-level affordability mitigation strategies. Examples include:
- Enrollment decreases are lower in states with state-based marketplaces (SBMs) and expected to stay lower than Healthcare.gov states, largely because of proactive outreach and marketing initiatives, lower net premium increases, and state affordability programs.
- States with premium alignment and silver-loading as a policy lever for improving gold plan affordability are seeing results. Gold plan enrollment increased by 10 percentage points in states where gold plans cost less than silver plans, whereas gold enrollment did not materially change in states where silver plans cost less. For states, this provides a lever to assist consumers seeking to shift into plans with lower cost-sharing without increasing premiums.
State-Reported Early Enrollment Results
Many states warned of coverage losses as a result of changing federal policies and the expiration of enhanced premium tax credits (ePTCs). State-specific reporting for 2026 validates the findings in the Wakely report. The recently released state-level data from SBMs affirms that the drop-off in enrollment through cancellations and dis-enrollments is significant. It also illustrates that state efforts to mitigate and address affordability gaps have worked to some extent but have not been enough on their own to head off coverage losses in 2026. Examples are as follows:
- In Georgia—the only SBM without Medicaid expansion—enrollment fell 27% from an estimated 1.3 million in April 2025 to approximately 950,000 in April 2026.
- In New Jersey—a state with state-funded premium subsidies, a reinsurance program, and a mandate that residents have health insurance—enrollment has decreased by more than 11% since April 2025.
- In California—another state with premium subsidies, facilitated enrollment, and an individual mandate—effectuated enrollment decreased by 7% from February 2025 to February 2026.
- Overall, SBMs are reporting that coverage drops were 24% higher from January to March 2026 than during the same period in 2025 and that the rate of plan shifting from Silver to Bronze increased significantly, quadrupling in six states.
Downstream Impact on Healthcare Access and Uncompensated Care
While not yet apparent in the early enrollment data, the downstream impact of 1) coverage losses, 2) increased enrollment in plans with higher cost-sharing, and 3) a worsening risk pool on the health of consumers, as well as the healthcare system, will be significant. Consumers may decide to postpone or forgo necessary care, which could lead to avoidable and more costly healthcare conditions. Increases in the number of people who uninsured and underinsured will have a direct and negative economic impact on provider finances, which are already strained, and uncompensated care and demands on patient assistance programs will increase accordingly.
Looking Ahead
The individual market will continue to evolve and change in the coming years as a result of future regulatory and operational changes. A shortened Open Enrollment Period, increased Medicaid redetermination requirements, and new pre-enrollment verification requirements are notable initiatives that are expected to roll out in the coming years.
Healthcare organizations and government agencies should consider the effect of these changes, including further coverage losses and instability in the individual market driven by the administrative complexity of these changes.
In addition, there are potential federal changes such as expanded availability of catastrophic plans, the introduction of non-network plans, and additional eligibility changes, which could put further strain on ACA Marketplace operations and the individual market.
Getting ahead of these changes will be critical to mitigating coverage losses and ensuring the long-term stability and viability of the individual market. In a federal policy environment that has largely deferred acting on ACA affordability, we expect policymakers, issuers, and other interest-holders to increasingly look to governors and state legislatures for decisive action. State subsidy and reinsurance programs are established affordability mechanisms that can provide consumers with affordability relief quickly, assuming state funding is available.
These investments can pay off for consumers from an economic perspective as well. For every additional dollar spent on state subsidies or reinsurance to maintain or increase coverage, states can expect to see reductions in uncompensated care, less reliance on patient assistance programs, and decreases in the number of consumers who forgo or delay care. In addition, investments in enrollment operations and assistance, outreach, and education will be critical to ensuring consumers are aware of the changes ahead and the actions they need to take to access and stay covered.
Connect with Us
Health Management Associates, Inc. (HMA), and Wakely colleagues are closely tracking federal policy activity and state actions to address these challenges. Our experts support states, issuers, consumer groups, and other interest-holders to achieve success in the operation of and participation in the marketplaces. Our team has broad historical knowledge of the challenges and opportunities in this market and can support every step of the planning and execution processes to improve affordability and stability as it evolves in the coming months and years.
Contact our experts below with questions about the report and to discuss opportunities to address the trends and forthcoming changes in the market.
To read more about the changes ahead, see the following reports:

Webinar Replay – ACA Enrollment Declines: Implications and Options for State and Federal Policymakers
This webinar was held May 21, 2026.
Recent and future policy changes are reshaping the ACA market. A recent Wakely report finds that only 86% of ACA enrollees nationwide paid their first premium at the start of the year, raising important questions about affordability, access, and market stability. Additionally, the 2027 Notice of Benefits and Payment Parameters (NBPP) is expected to be finalized this Spring which will have additional implications for consumers, issuers, and other stakeholders. As policymakers and state leaders consider how to respond to the shifting market composition and future policy changes, this discussion will focus on the policy implications of these shifts and the options to address affordability and coverage options to improve market stability.
During this webinar, HMA’s ACA team had a policy-focused conversation on what these projected changes mean for marketplace dynamics, including impacts to risk pools, premiums, and issuer participation. The session explored emerging federal and state policy responses and offered insight into how today’s decisions may shape 2027 rates, plan offerings, and long-term market sustainability.
Learning Objectives:
- Analyze policy drivers: Examine how changes to federal subsidy policy are influencing ACA marketplace enrollment, affordability, and coverage continuity.
- Evaluate policy tradeoffs: Assess how enrollment declines impact market stability, including risk pools, premiums, and issuer participation.
- Inform policy strategy: Identify state and federal policy options to mitigate coverage losses and support a stable, competitive marketplace heading into 2027.
CMS Proposes Modest Hospital Payment Updates and Signals Expanded Use of Mandatory Value-Based Models
On April 10, 2026, the Centers for Medicare & Medicaid Services (CMS) released the proposed rule for the Fiscal Year 2027 Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System (LTCH PPS). The proposal combines a modest net increase in hospital payments with policy signals around quality reporting and mandatory episode-based payment models—most notably a proposed nationwide expansion of the Comprehensive Care for Joint Replacement (CJR) model.
These proposed updates underscore CMS’s continued emphasis on value-based purchasing, episode accountability, and alignment across quality programs. In addition, CMS resurfaces ongoing debates with hospital stakeholders about the adequacy of Medicare payment updates amid rising costs and coverage disruptions.
This article reviews several key provisions in the FY 2027 proposed rule.
Hospital Payment Updates: Headline Increase Masks Net Impact
Under the proposed rule, CMS would increase base IPPS and LTCH PPS payment rates by 2.4 percent in FY 2027. However, after accounting for proposed reductions to uncompensated care payments for disproportionate share hospitals (DSH) and changes in outlier payments for extraordinarily high-cost cases, CMS estimates the effective payment increase would be closer to 1.2 percent.
In aggregate, CMS projects the proposed update would translate to approximately $1.4 billion in additional payments to acute care hospitals next year. Hospital industry groups—including the American Hospital Association (AHA) and the Federation of American Hospitals (FAH)—have pushed back, arguing that the proposed update does not sufficiently reflect medical inflation, workforce pressures, or anticipated growth in the uninsured population.
These concerns reflect a long-standing dynamic in annual hospital payment rules: CMS seeking to balance statutory updates and budget neutrality constraints against the hospital industry’s concern that Medicare payments are lagging behind underlying costs.
Quality Reporting and Program Alignment
The proposed rule would also make notable updates to the Hospital Inpatient Quality Reporting (IQR) Program. CMS proposes adding three new quality measures to be phased in during 2029 and 2030, while modifying eight existing measures to include Medicare Advantage patients. CMS also proposes shortening the performance period for certain measures from three years to two—a change designed to accelerate feedback and better align measures across programs.
These changes continue CMS’s broader effort to harmonize quality measurement across Medicare payment and value-based programs, reduce reporting lag, and incorporate a more comprehensive view of patient populations.
Updates to Mandatory TEAM Model
CMS also proposes several updates to the Transforming Episode Accountability Model (TEAM), the mandatory episode-based payment model finalized last year. Key proposals include:
- Expanding the list of MS-DRGs included in the spinal fusion episode
- Aligning TEAM quality measurement performance periods with the IQR Program
- Making targeted technical refinements to payment methodology
In addition, CMS is seeking stakeholder feedback on whether ambulatory surgery centers (ASCs) should participate in TEAM and whether participation should be voluntary for physician-owned hospitals, signaling potential future expansion or recalibration of the model.
Proposed Expansion of Joint Replacement Bundles
CMS proposes to expand the existing Comprehensive Care for Joint Replacement Expanded (CJR-X) Model nationwide beginning October 1, 2027. The agency also plans to make participation mandatory for most IPPS hospitals.
CMS tested the original CJR model in 34 metropolitan areas between 2016 and 2024, generating improved patient outcomes and net Medicare savings, according to agency evaluations. CJR-X would become the fifth Center for Medicare and Medicaid Innovation model to meet the statutory criteria for nationwide expansion.
Under CJR-X, hospitals performing lower extremity joint replacements would be accountable for the cost and quality of care for the initial procedure and most related spending during the subsequent 90 days. Although the overall structure mirrors the original CJR model, CMS proposes several important updates:
- Expansion of episodes to include ankle replacements, in addition to hip and knee procedures
- Adoption of a more robust risk adjustment methodology with significantly more variables, aligning closely with the TEAM model
- Introduction of a 5 percent stop-loss policy for hospitals that serve higher proportions of dually eligible beneficiaries and certain smaller hospitals
Participation would be mandatory for most IPPS hospitals, with exceptions for hospitals already participating in TEAM, which includes a lower extremity joint replacement episode; Maryland hospitals operating under global budgets; and hospitals not paid under both IPPS and the Outpatient Prospective Payment System, such as Critical Access Hospitals.
Why It Matters
The 2027 IPPS and LTCH PPS proposed rule reinforces several clear policy signals:
- Pressure on hospital margins is likely to persist, as payment updates continue to trail hospital-reported cost growth.
- Mandatory episode-based models remain central to CMS’s value-based strategy, with CJR-X representing a significant escalation in scope and scale.
- Program alignment and MA inclusion are accelerating, with implications for hospital data systems, care coordination strategies, and reporting infrastructure.
Hospitals and health systems will need to assess not only the near-term financial impact of the proposed payment updates, but also their readiness to accept expanded episode accountability and meet evolving quality measurement requirements.
Comments on the proposed rule will shape final decisions regarding payment levels, quality program changes, and the scope of mandatory participation in CJR-X. Stakeholders will be watching closely to see whether CMS moderates its approach to mandatory models or doubles down on episode-based accountability as a cornerstone of Medicare payment reform.
In parallel, CMS has released several other proposed payment rules this month, including those that would affect skilled nursing facilities, hospice providers, inpatient rehabilitation facilities, and inpatient psychiatric facilities. For these entities, CMS generally proposes payment updates of approximately 2.4 percent and 2.3 percent for inpatient psychiatric facilities. As part of its broader program integrity focus, CMS also has proposed new transparency measures for hospice providers; this follows recent enforcement actions related to fraudulent enrollment.
Connect with Us
Health Management Associates, Inc. (HMA), monitors federal regulatory and legislative developments in the inpatient setting and assesses the impact on hospitals, life science companies, and other stakeholders. Our experts interpret and model hospital payment policies and assist clients in developing CMS comment letters and long-term strategic plans. Our team replicates CMS payment methodologies and model alternative policies using the most recent Medicare fee-for-service and Medicare Advantage (100%) claims data. We also support clients with DRG reassignment requests, New Technology Add-on Payment (NTAP) applications, and analyses of Innovation Center alternative payment models.
For more information about the proposed policies, contact one of our Medicare experts.
Medicaid Managed Care Enrollment: Q4 2025 Trends and Early Signals Ahead of New Eligibility Policies
This week Health Management Associates (HMA), draws on its database of monthly Medicaid managed care enrollment to present its latest quarterly analysis, offering a snapshot of enrollment trends across 37 states.
The analysis comes at a critical time. As states prepare for Medicaid eligibility policy changes that take effect in 2027—including more frequent eligibility determinations and expanded work and community engagement requirements—current enrollment trends provide an early signal of how policy decisions and administrative practices are already influencing coverage levels.
The HMA Information Services (HMAIS) analysis shows that Medicaid managed care accounted for 85.6 percent of total Medicaid enrollment in December 2025. This analysis, available to HMAIS subscribers, uses data from nearly 300 health plans in 41 states. The report provides by-plan enrollment plus corporate ownership, program inclusion, and for-profit versus not-for-profit status, with breakout tabs for publicly traded plans.
Key Insights from Q4 2025 Data
The 37 states included in this review have released monthly Medicaid managed care enrollment data through public websites or in response to a public records request from HMA. The report includes the most recent data obtained and illustrates the effect of state-level choices around eligibility and administration. Key findings include:
- As of December 2025, Medicaid managed care enrollment across the 37 states declined by 2.2 million members year over year, falling to 62.5 million—a 3.4 percent decrease.
- Of the 37 states, eight—Colorado, Delaware, Mississippi, Missouri, New Jersey, North Carolina, North Dakota, and Oregon—did not experience year-over-year managed care enrollment declines, and instead showed flat enrollment or modest gains. With the exception of Mississippi, these are all Medicaid expansion states.
- Arizona and Indiana experienced double-digit percentage declines. Notably, Indiana began requiring enrollees to actively respond to renewal mailers, which aligns with enrollment declines that began in March 2025.
- Among the expansion states in the analysis, enrollment declined by 1.7 million (-3.3%) to 50.8 million. The seven non-expansion states experienced a similar decline (-3.6%), bringing enrollment to 11.7 million enrollees.
Data Considerations. The data have some important limitations. States report enrollment figures at different points during the month, with some data reflecting beginning of the month totals and others capturing end of the month enrollment. In addition, some state datasets encompass all Medicaid programs offering managed care plans, whereas others reflect only a subset of the managed Medicaid population. As a result, the findings should be viewed as indicative of broader trends rather than a comprehensive state-by-state comparison.
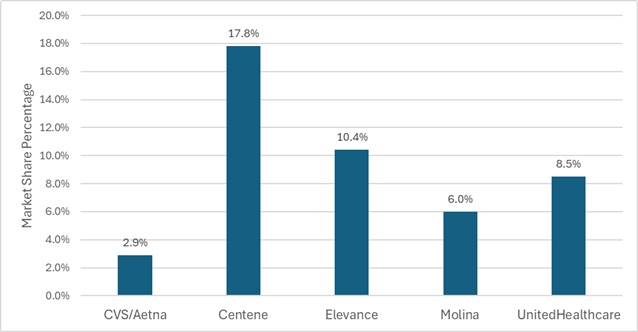
Market Share and Plan Dynamics
Using our data repository for 300 health plans across 41 states, HMAIS analyzes corporate ownership, program participation, and tax status among Medicaid managed care plans. As of December 2025, Centene maintained the largest share of the national Medicaid managed care market at 17.8 percent, followed by Elevance (10.4%), United (8.5%), and Molina (6.0%) (see Figure 1). These figures highlight continued concentration among large national plans, even as overall enrollment declines.
Figure 1. National Medicaid Managed Care Market Share by Number of Beneficiaries for a Sample of Publicly Traded Plans, December 2025
What to Watch
Enrollment trends observed in the fourth quarter (Q4) of 2025 and continuing into 2026 indicate increasing state attention to eligibility policy and program integrity. State legislative activity, budget pressures, and federal regulatory developments are prompting many states to assess and strengthen certain aspects of their programs related to eligibility, particularly as they prepare to implement redetermination and work and community engagement requirements.
Several states are already moving toward implementation. Nebraska is scheduled to launch Medicaid work requirements on May 1, 2026, while Montana plans to begin implementation on July 1, 2026. With additional federal guidance still emerging, most other states are working toward compliance ahead of January 2027 deadlines. In expansion states, policymakers retain authority to tighten administrative processes, alter optional benefits, or adjust provider payment levels—actions that may materially affect enrollment.
These developments underscore why Medicaid managed care enrollment trends deserve close attention. Declines in enrollment are often an early indicator of broader system impacts, including rising uncompensated care for providers, shifts in payer mix, and increased financial pressure on safety‑net systems. For managed care organizations, even modest enrollment changes can mask more significant shifts in risk profiles, geographic concentration, or service needs.
Connect with Us
HMA is home to experts who know the Medicaid managed care landscape and how it is evolving. HMAIS’s Medicaid enrollment data, financials, procurement tracking, and a robust library of public documents equips stakeholders with timely, actionable intelligence.
For more information about the HMAIS subscription, contact Andrea Maresca and Alona Nenko.
HMA Resource Provides Key Insights about the Evolving Medicare-Medicaid Integration Landscape
People who are dually eligible for Medicare and Medicaid remain a central focus for policymakers and healthcare organizations, given their complex care needs, disproportionate share of spending, and the long-standing challenge of coordinating coverage across two programs. One of the primary vehicles for advancing integration has been Dual Eligible Special Needs Plans (D-SNPs), which continue to play an increasingly prominent role as federal and state policymakers encourage tighter Medicare-Medicaid alignment.
As states play a more active role in shaping enrollment rules, Medicaid contracting, and procurement strategies, the duals market is becoming more structured and more explicitly guided by state policy decisions. Health Management Associates (HMA’s) 2026 Duals Integration Environmental Inventory, examines how this shift shapes the integration landscape in 2026. This comprehensive inventory is based on a review of the 2026 market, insights from states, and other publicly available resources.
This article examines key trends from HMA’s 2026 inventory and addresses federal policy changes scheduled to take effect for 2027, which contribute to this dynamic environment.
What to Expect in 2026
As the landscape for duals integration evolves, the central question has shifted from whether D-SNPs operate in a state to the more consequential question of how states are using Medicaid policy levers (i.e., enrollment rules, procurement, contracting, and managed care structures) to drive tighter alignment between Medicare and Medicaid.
At the federal level, recent Medicare Advantage and Part D rulemaking is reinforcing that movement. The Contract Year 2025 Medicare Advantage and Part D Final Rule finalized the second phase-down of the D-SNP look-alike threshold to 60 percent for 2026 and established 2027 rules that limit enrollment in certain D-SNPs to members of an affiliated Medicaid managed care organization. The rule also limits the number of D-SNP benefit packages that can be offered alongside an affiliated Medicaid managed care organization. More recently, the Contract Year 2026 Medicare Advantage and Part D Final Rule requires certain D-SNPs to use integrated member ID cards and integrated health risk assessments beginning in 2027.
Together these rules signal a continued federal emphasis on linking D-SNP enrollment and operations more closely to Medicaid coverage and delivery systems, with states playing a greater role in determining how alignment is achieved.
What the 2026 Inventory Shows
HMA’s 2026 Duals Integration Environmental Inventory shows how these policy signals are translating into state action. More specifically:
- Statewide exclusively aligned enrollment appears in 16 states in the 2026 inventory, up from nine in 2025.
- Applicable Integrated Plans (AIPs) are present in 22 states, up from 14, and default enrollment is in place in 21 states, up from 16.
- The inventory also captures 6,084,997 total D-SNP enrollees, including 1,975,250 in Highly Integrated SNPs (HIDE) and 743,683 in Fully Integrated SNPs (FIDE-SNPs).
Those changes are already visible in state markets:
- Illinois, Massachusetts, Ohio, and Rhode Island entered 2026 with a greater FIDE-SNP presence tied to legacy Medicare-Medicaid Plan transitions.
- Michigan launched MI Coordinated Health as a HIDE-SNP in selected regions in 2026, with statewide expansion planned for 2027.
- Delaware also stands out: Although it already had AIPs in the 2025 inventory, it adds statewide exclusively aligned enrollment in 2026 and shows both HIDE-SNPs and coordination-only D-SNPs.
A Resource to Track State Market Direction
HMA’s 2026 Duals Integration Environmental Inventory, available to HMA Information Services (HMAIS) subscribers, includes a state-by-state view of the Medicaid policy, contracting, and program structures shaping duals integration and D-SNP markets. In addition to enrollment trends, the inventory documents the integration model each state is pursuing, whether long-term services and supports or behavioral health are included in managed care, and how procurement and contract decisions may inform future market activity.
HMA experts work with clients to apply this information and deepen their understanding of state integration approaches, inform assessments of their market readiness and alignment opportunities, and develop strategies that support more effective Medicare-Medicaid integration.
Looking Ahead
Notably, HMA’s inventory reflects a point in time understanding of where an individual state is today and what is known at this time about their next steps and plans. However, we expect changes in many states as they seek guidance from the Centers for Medicare & Medicaid Services and the D-SNP community to implement required changes and adopt new regulatory provisions that support state goals and priorities.
The 2026 inventory suggests that more states are using formal alignment tools, that more enrollment is concentrated in integrated products, and that more markets are being shaped by the interaction between Medicaid structure, procurement, and D-SNP strategy.
Connect with Us
For organizations seeking to understand where the market is headed, the Duals Integration Inventory offers a clear view of how state policy and market structure are evolving and where tighter Medicare-Medicaid alignment is taking hold.
Contact Holly Michaels Fisher and Julie Faulhaber to discuss your organization’s questions and needs regarding an integration strategy and market analysis. For information about the HMAIS subscription, access to the Duals Environmental Inventory contact Andrea Maresca and Gabby Palmieri.

Connected Crisis Care: Generating Collaborative Solutions for 988 and Beyond
HMA Solutions
Connected Crisis Care: Generating Collaborative Solutions for 988 and Beyond
Health Management Associates, Inc. (HMA), is a national leader in crisis system design, known for developing innovative, collaborative, data-driven solutions that help states and communities build effective, person-centered crisis response systems. We help strengthen crisis response systems through skill-building and collaboration strategies. Our model creates lasting crisis response system connections, fosters trust, and enhances the overall quality of care across the crisis response continuum.
Is your state, region, or county ready to enhance and sustain its crisis response?
Has your state recently launched 988, mobile crisis teams, or crisis stabilization units and is now exploring next steps to strengthen the system?
Are you seeking practical, engaging training, and convening strategies to deepen collaboration and elevate your crisis response across all partners?
Our Approach:
Coordinated Crisis Response Through Skill-Building and System Integration
Our team uses a two-prong approach to bring together a diverse group of providers, partners, and stakeholders to expand system capacity and build trust and collaboration across the crisis response continuum. Through a series of cross-system trainings and convenings, we lay the foundation for better communication, coordination, and collaboration. This approach ensures that individuals in crisis experience more seamless, coordinated, and compassionate care across every point of the response continuum.
Skill-Building:
Monthly Training Programs Tailored to Every Role in Crisis Response
"This training helped cross-train coping strategies for working with clients, reminded us that there is always a path through stress, and helped us focus on meeting individuals where they are in their journey." -Crisis care provider
We collaborate with our clients to determine the best approach for training that meets the needs of your organization. Our monthly virtual training courses are designed to meet crisis response providers where they are—across all levels of readiness and roles. Using diverse learning methods, such as didactic instruction, interactive problem-solving, and peer-to-peer collaboration, we ensure content is practical, engaging, accessible and grounded in best practice frameworks and protocols. Topics include culturally responsive mobile crisis response, trauma-informed care, suicide risk assessments, and working with diverse populations including youth, older adults, and individuals with intellectual/developmental disabilities. Each session builds real-world skills that can be applied immediately in the field. In addition, these courses can be set up to be taken on demand.
System Integration:
Systemwide Convenings to Build Trust and Drive Collaboration
"I appreciate having a variety of divisions and departments (i.e., HR) participating in these monthly convenings. Thank you for this opportunity and collaboration." - Crisis convening attendee
Through structured, facilitated convenings, led by HMA’s crisis response experts, we bring together a diverse network of crisis providers, partners, and stakeholders to strengthen coordination across the full crisis continuum. We use Liberating Structures and other learning techniques to enhance engagement, foster relational trust, share knowledge, and sustain collaboration. Convening topics can be aligned with the monthly training topics to reinforce learning and provide opportunities to operationalize new skills and understanding across the crisis continuum. Convenings often highlight local exemplars as a way to share local best practices and encourage locality-specific collaboration and problem-solving.
Ready to Build Trust and Capacity in Your Crisis System?
We are excited to partner with your crisis care system to help you create a transformative response model based on collaboration, trust, and ongoing professional development. In addition to this suite of offerings, the HMA team has expertise in helping communities develop and implement strategic roadmaps for next-phase crisis system improvement.
Who We Help
911/call centers/emergency management services (EMS)
Associations and foundations
Behavioral health care providers
Coalitions and advocates
Criminal justice stakeholders and facilities
Crisis care systems and providers
Educational settings and academic institutions
Federal, state, and local government agencies
Health plans
Hospitals and health systems
Investors
Law enforcement
Public health departments
Project Spotlight:
HMA has significant experience in supporting states and other clients with behavioral health crisis care design, training, implementation of 988, policy and evaluation strategies. HMA assists 12 states (California, Colorado, Iowa, Louisiana, Massachusetts, Mississippi, New York, Ohio, Oklahoma, Rhode Island, Vermont, and Washington) and jurisdictions (e.g., New Haven, CT), philanthropic organizations, healthcare systems, and other organizations to develop and implement 988 crisis lines and/or crisis system assessment and design. We leverage our experience across states, counties, and jurisdictions to share emerging best practices in crisis and 988 care.
What Makes HMA Different?
Many of our team members are former executives and clinical leaders from the behavioral health sector. They bring decades of experience in leading behavioral health care in inpatient, outpatient and emergency department settings, and have been instrumental in establishing the 988 program. HMA provides the depth, agility, and collaborative approach to address today’s most urgent behavioral health challenges. We know the challenges faced by states and organizations, and support strategic planning and implementation, large scale crisis system redesigns, crisis needs assessments, and relationship building with stakeholders.
Contact our experts:

Angela Bergefurd
Senior Principal

Allie Franklin
Managing Director

Jennifer Hodgson
Principal

Monica Johnson
Managing Director

Kim Williams
Principal

April 22, 2026
HMA Resource Provides Key Insights about the Evolving Medicare-Medicaid Integration Landscape

Medicare’s “Inpatient Only” Rule Is Going Away. Now What?
This episode of Vital Viewpoints on Healthcare explores how evolving Medicare payment policy is reshaping where and how care is delivered. The discussion covers the phase-out of the inpatient only list and the operational and financial challenges tied to shifting procedures into outpatient settings. Zach Gaumer, regional director at Health Management Associates, shares his perspective on the policy mechanics, provider behavior, and market signals emerging from CMS rulemaking; while Rachel Stewart, senior consulting actuary at Wakely (an HMA Company), explains how plans are modeling uncertainty, navigating contract dynamics, and assessing the downstream impact on costs and quality across the healthcare system.