This week, our In Focus section looks at a new Medicare model, Direct Contracting, introduced by the Centers for Medicare & Medicaid Services (CMS) Innovation Center. The new model will build on and continue testing potential reforms to the Medicare program encompassed by accountable care organizations (ACOs), Medicare Advantage (MA), and private sector risk-sharing arrangements. The payment model options may appeal to a broad range of physician and provider groups and other organizations because they are expected to introduce flexibility in health care delivery, support a focus on beneficiaries with complex, chronic conditions, and encourage participation from organizations that have not typically participated in traditional fee-for-service (FFS) Medicare or CMS Innovation Center models. However, there will be substantial financial risk—and reward—for participants based on a new, complex methodology, so organizations interested in this new model should carefully consider the possible outcomes from participating in Direct Contracting versus other options. CMS has announced that 51 organizations will participate in the model’s trial Implementation Period, which runs from October 1, 2020, through March 31, 2021. The agency has stated that it expects to announce additional Direct Contracting pathways in the future and that the next round of applications for participation in the second performance year will open in early 2021.
CMS’s Direct Contracting model will test a set of three voluntary payment model options aimed at reducing expenditures and preserving or enhancing quality of care for beneficiaries in FFS Medicare (Figure 1). CMS has provided significant flexibility in terms of who can qualify as a Direct Contracting Entity (DCE); providers have the option to organize into participant groups as they see fit. The following are examples of organization types that may be eligible: ACOs or ACO-like organizations, networks of individual practices (e.g., IPA), hospital systems, integrated delivery systems, partnerships of hospital systems and medical practices, Medicaid managed care organizations (MCOs), other payers, and skilled nursing facilities (SNFs).[1] The specific requirements are that the DCE:
Is a legal entity identified by tax identification number (TIN) formed under applicable state federal, or tribal law, and authorized to conduct business in each state that contracts with CMS for the Direct Contracting Model
- Is responsible for receiving shared savings and paying shared losses to CMS
- Is capable of administering payments to DCE Participant Providers, and if applicable, Preferred Providers
- Establishes, reports, and ensures DC Participant provider compliance with health care quality criteria, including quality performance standards
- Fulfills other DCE functions identified in the Participation Agreement

DCEs must have arrangements with Medicare-enrolled providers or suppliers, who agree to participate in the model and contribute to the DCE’s goals pursuant to a written agreement. DCEs form relationships with two groups of providers or suppliers:
- DC Participant Providers
- Are used to align beneficiaries to the DCE
- Are required to accept payment from the DCE through their negotiated payment arrangement with the DCE
- Report quality
- Preferred Providers
- Are not used to align beneficiaries to the DCE
- Can elect to accept payment from the DCE through a negotiated payment arrangement with the DCE
- Both Participant Providers and Preferred providers
- Continue to submit claims to Medicare and accept claims reduction
- Are eligible to receive shared savings
- Have the option to participate in benefit enhancements or patient engagement incentives
Initial participants will gain experience with beneficiary attribution or “alignment” to participant organizations during the Implementation Period that started October 2020. The first PY is scheduled to begin in April 2021 and will be followed by five additional PYs. The Innovation Center will expect beneficiaries to be aligned with the DCE primarily voluntarily. Under voluntary alignment, beneficiaries choose to align to a DCE by designating a Participant Provider as their primary clinician. The other alignment option is similar to that of ACO claims-based alignment with CMS aligning beneficiaries based on where they receive the plurality of their primary care services, as evidenced in claims data.
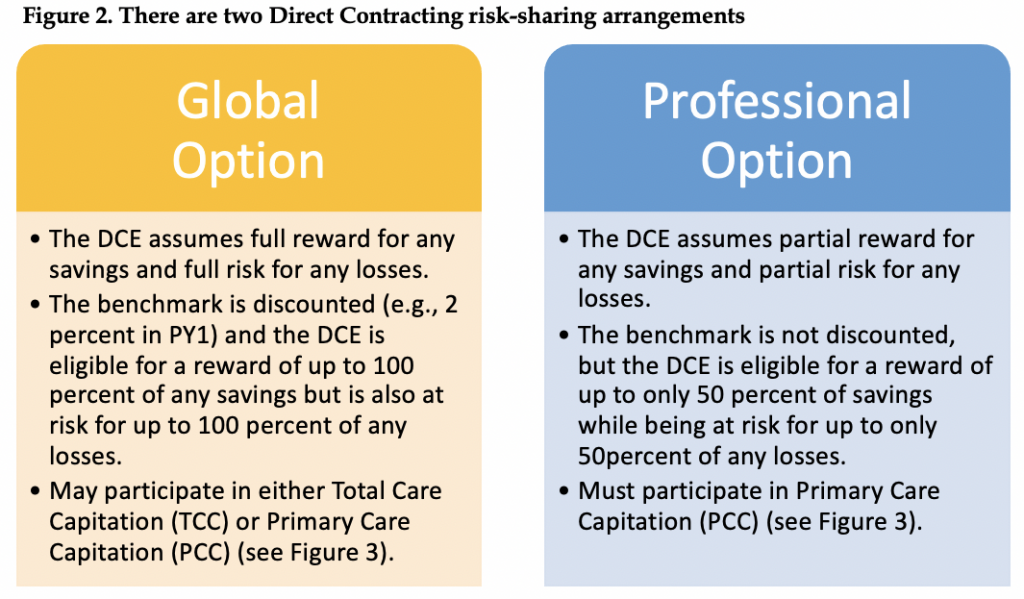
Direct Contracting offers options for both risk-sharing arrangements and risk mitigation strategies. The two risk-sharing arrangements are the Global Option and the Professional Option (Figure 2). Direct Contracting includes two risk mitigation strategies available for DCEs: risk corridors and stop-loss reinsurance. Risk corridors determine the percentage of the savings or losses that are retained by the DCE. Optional stop-loss protects DCEs from financial liability for individual beneficiary expenditures above the stop-loss “attachment points” (i.e., dollar thresholds at which stop-loss protection begins).
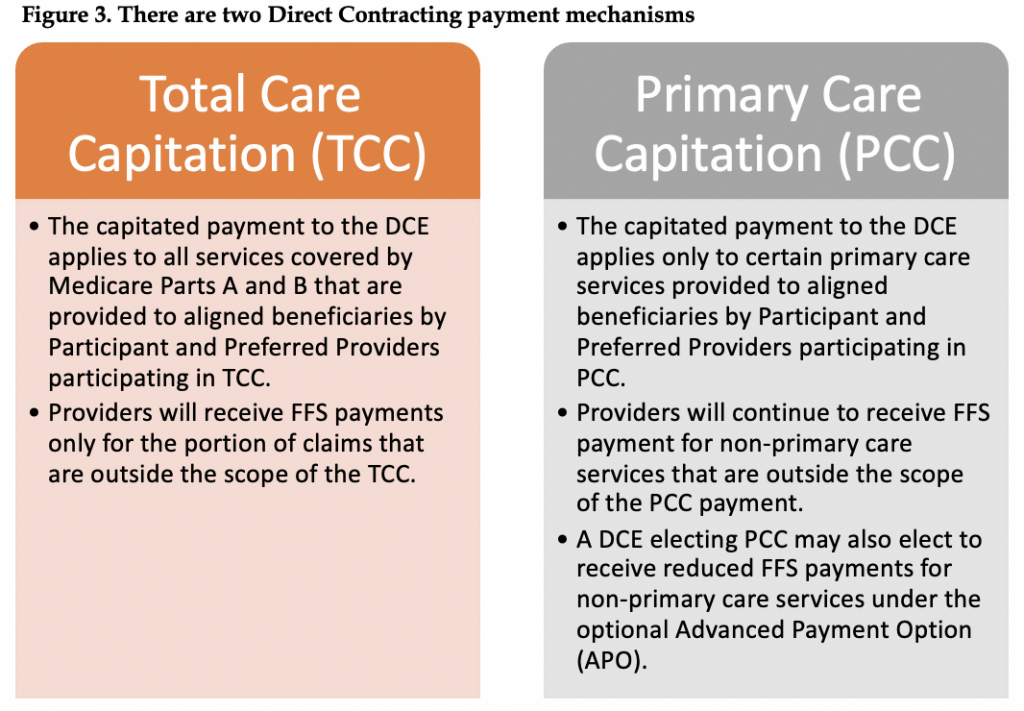
Direct Contracting offers two payment mechanisms in which DCEs are paid a monthly capitated amount based on claims reductions made for Participant Providers and Preferred Providers. All DCEs must participate in one of the capitation payment mechanisms (Figure 3). A DCE electing PCC may also elect to accept claims reduction through the optional Advanced Payment Option (APO). The APO is available only to Preferred and Participant Providers of a DCE electing PCC. It is up to each individual provider to decide whether they want to pursue claims reduction via the APO, and each provider may choose the desired percent reduction for relevant FFS claims (1 percent–100 percent). Because APO applies to non-primary care services (i.e., services for which PCC does not apply), APO is complementary to PCC in that APO and PCC will never apply to the same service.
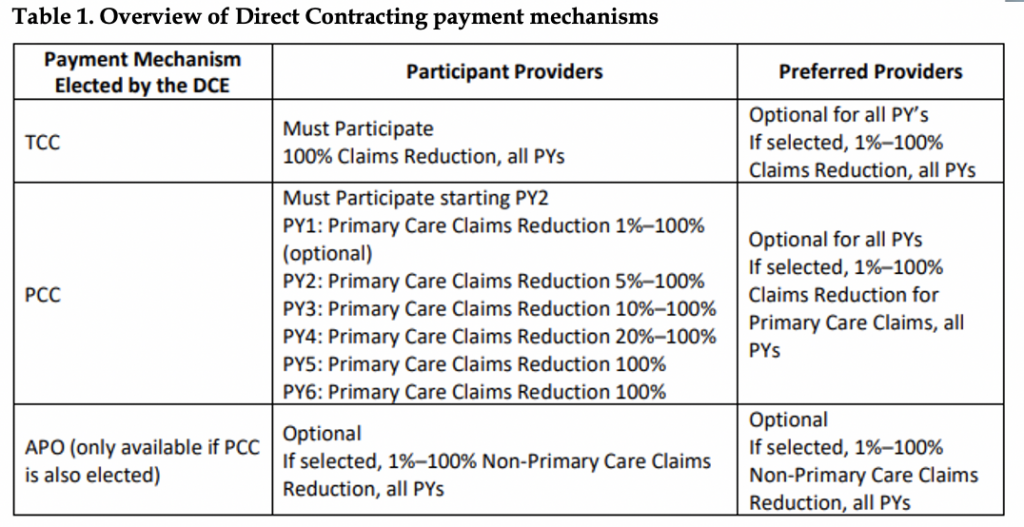
The impact of decisions made about TCC versus PCC vary depending on the PY and whether providers have opted to be Participant or Preferred Providers (Table 1).
The elections that organizations interested in participating as a DCE make for each of these model characteristics include: type of DCE, selection of Participant and Preferred providers, risk-sharing arrangements, payment mechanisms, and additional choices can have a substantial impact on potential shared savings and losses. HMA staff have extensive experience evaluating the most optimal pathway, understanding unique organizational risks, and assessing the implications of these decisions for the Direct Contracting model relative to other opportunities, including additional Innovation Center models. HMA also assists clients with the implementation process, including conducting assessments of organizational readiness.
[1] During the Implementation Period, DCEs and their DC Participant Providers and Preferred Providers can participate in both the Direct Contracting Model and the Medicare Shared Savings Program (MSSP). During each performance year starting with 2021, DCEs and their DC Participant Providers may not simultaneously participate in the MSSP. The determination of whether such an overlap exists will be made at the tax identification number (TIN) level prior to the start of each performance year. This requirement does not apply to Preferred Providers.