This week, our In Focus section highlights key insights from a new Health Management Associates (HMA), white paper, Concentration of Specialty Services in Medicaid. Experts from HMA and Wakely, an HMA company, used the national Transformed Medicaid Statistical Information System (T-MSIS) database to learn more about specialty provider networks and examine the provision of specialty services across various states.
The analysis, released in January 2025 with support from the Robert Wood Johnson Foundation, focuses on three representative services that are relatively common, potentially difficult for Medicaid beneficiaries to access, significantly affect quality of life, typically accessed as elective procedures, and unlikely to be provided by other clinicians, such as primary care or mid-level practitioners.
T-MSIS Analysis Overview
T-MSIS analytic files are a comprehensive resource for Medicaid encounter, beneficiary demographics, program enrollment, service utilization, and payment data. Individual states compile their Medicaid claims data and submit monthly files to the Centers for Medicare & Medicaid Services (CMS). As each state submits data individually, numerous state-specific variations occur in data availability and quality. Currently, T-MSIS data are available for 2016−2023. HMA data scientists have permission to use the T-MSIS files for healthcare services research.
This paper examines services in 10 states that met a threshold of data integrity in the T-MSIS dataset for 2022. Other important design aspects of the analysis are as follows:
- The three service procedures included in the analysis are total knee replacement (TKA), cataract removal, and impacted tooth extraction.
- Selected states represented a diverse sample of geographic, socioeconomic, and other demographic factors.
- The analysis includes non-dually eligible adult populations, ages 22−64 years.
- The data cover all services provided in 2022 for each procedure and the providers who rendered the service; facilities are excluded.
Concentration of Specialty Providers
Table 1 summarizes findings about the concentration of specialty services.
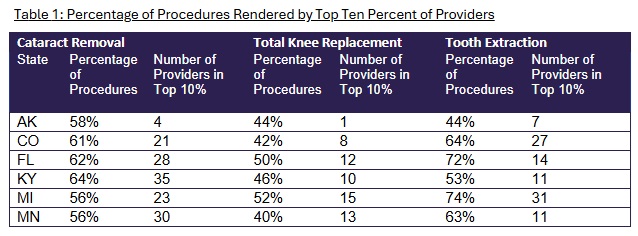
The authors further analyzed the provision of services and, building on a previous study, examined network concentration. Findings were as follows:
- When looking at the same procedure across states, no consistent pattern emerged regarding which states had the highest and lowest concentration of services in the top 10/25 percentile of providers.
- However, when looking at the same procedure across multiple states, TKA tended to have the lowest concentration of services among those studied.
- Regardless of procedure and state, the 50 percent of providers with the lowest number of procedures tended to provide fewer than 10 percent of the total services combined.
These findings suggest that the specialty networks within each state are highly nuanced, and state policymakers need to look at individual specialty networks when considering health policy. State policymakers and managed care organizations (MCOs) need to examine each specialty individually to assess the distribution of services and access to care.
Looking Ahead
Timely access to healthcare services is critical for ensuring optimal health outcomes. The report authors’ analysis of T-MSIS data showed significant concentration of selected specialty services among providers, which may affect appropriate access to these services.
The analysis of concentration of specialty services among Medicaid specialty providers can guide MCOs and state policymakers in developing strategies to improve network adequacy, including clarifying the level of network adequacy and developing policies to assess and regulate access to specialty care. Addressing gaps in access to specialty care can contribute to better health outcomes for Medicaid beneficiaries and may be aligned with provisions in value-based contracts.
Connect with Us
Medicaid consumers, providers, MCOs, and states all have an interest in ensuring access to specialty care for Medicaid beneficiaries. The methodology applied in the analysis for the HMA white paper can be applied and adapted for future analysis to monitor network stability and to compare access among various payers.
For details about this analysis, its implications for state and local policies, and additional research using T-MSIS, contact our experts below.