
On May 13, 2025, the Centers for Medicare & Medicaid Services (CMS) published its new strategic direction for the CMS Innovation Center. The strategy builds on the lessons of the first 15 years of the Innovation Center, while presenting a significant pivot in policy direction, which emphasizes evidence-based prevention, consumer engagement, and tech-enabled care, while prioritizing financial performance over broad participation.
The new strategy provides high-level direction on the Trump Administration’s vision for the next phase of value-based payment reform under the leadership of CMS Administrator Dr. Mehmet Oz and Innovation Center Director Abe Sutton. They intend to “double down on our commitment to value-based care and take the learnings from the[se] previous investments to build a health system that empowers people to drive and achieve their health goals and Make America Healthy Again.” Notably, the strategy also aligns with goals central to the Trump Administration’s Make America Healthy Again initiative.
This new direction affirms the administration’s commitment to continue advancing value-based care and opens additional opportunities for organizations seeking to enhance the delivery of services that drive positive outcomes. Health Management Associates (HMA), experts will be tracking the implementation of the Innovation Center’s new strategy, including expected forthcoming models, movement toward greater levels of downside risk, and changes to existing models to align with the administration’s priorities. In this article, our experts review the strategy and provide insights on key takeaways for stakeholders.
New Strategy Overview
CMS leaders view the Innovation Center agenda as a framework for accelerating healthy behaviors, leveraging the agency’s authority to test new approaches designed to incentivize and engage stakeholders. According to CMS officials, the Innovation Center “will work expeditiously toward the future of health—building a system in which people are empowered to achieve their health goals and providers are incentivized to compete to deliver high-quality, efficient care and improve the health outcomes of their patients.”
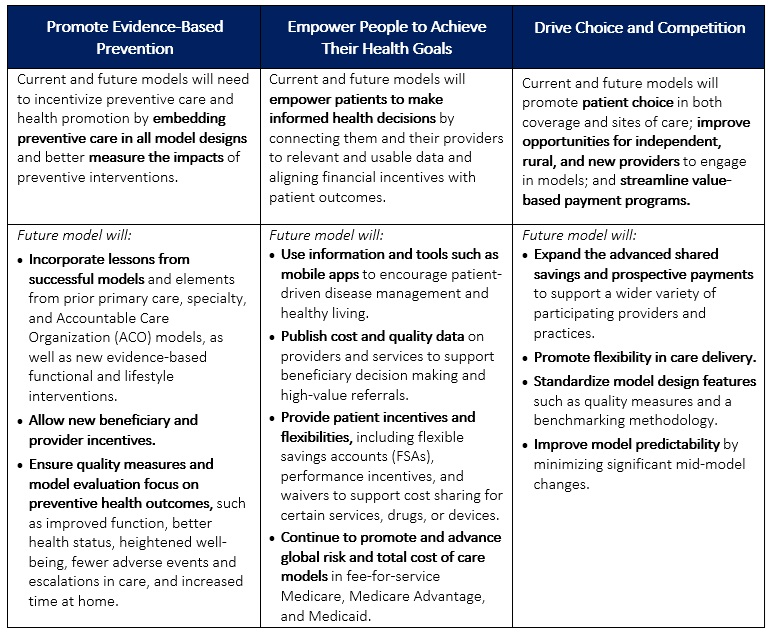
The strategy has three interrelated, foundational pillars:
- Promoting evidence-based prevention
- Empowering people to achieve their health goals
- Driving choice and competition.
Table 1 provides more detail on each pillar.
In addition to the new agenda, CMS released a request for information (RFI) seeking industry input on strategies that can better leverage data and technology to empower consumers. The focus of the RFI aligns with the Innovation Center’s strategic pillars to use tools, information, and processes that better connect people to their health data and allow them to make informed health decisions alongside their providers.
Table 1. CMMI’s Interrelated Strategic Pillars
Takeaways and Considerations
Critical to CMS’s approach is the belief that empowering individuals to make their health decisions—through incentives, better data access, and more flexible options—can lead to better health outcomes and lower overall costs. This shift reflects an evolution in healthcare policy that places greater emphasis on personal accountability and private sector collaboration—a key theme that is emerging across the administration’s policy initiatives.
Consumer Engagement. One of the most notable aspects of the new Innovation Center strategy is the promotion of consumer engagement; it places more focus on direct consumer engagement through education and incentives compared with earlier initiatives. This is one area in which the Innovation Center plans to collaborate with the private sector to develop consumer-facing tools (e.g., mobile apps, nudges toward healthy behaviors, etc.).
The focus on consumer engagement also presents opportunities for organizations to enhance their customer experience. By understanding the needs and preferences of their patients, organizations can tailor their services and care models to better meet those demands. This personalized approach not only improves patient satisfaction, but also drives continuity of care, ultimately contributing to long-term improvements in health.
Data and Technology. The new strategy also emphasizes the importance of data, indicating intentions to better equip organizations that participate in the model with data that can inform decisions and optimize their processes. CMS officials are examining policies and collaborations that will empower private sector organizations, including model participants, researchers, and technology vendors, to develop innovative data-driven solutions to drive efficiencies and improved health.
To that end, the May 16, 2025, Request for Information (RFI) from CMS and the Assistant Secretary for Technology Policy/Office of the National Coordinator for Health (ASTP/ONC), Health Technology Ecosystem (CMS-0042-NC), focuses on Medicare beneficiaries’ use of technology to improve health outcomes. The RFI, which HMA experts analyze here [insert bookmark or link to the other In Focus article] underscores the administration’s intentions of taking “bold steps to modernize the nation’s digital health ecosystem.”
Medicare Advantage. The Innovation Center’s new strategy indicates that stakeholders should expect more models that address Medicare Advantage (MA). The agency stated that “features of a model could include testing changes to payment for MA plans, such as testing the impact of inferred risk scores, regional benchmarks, or changes to quality measures that better align with promoting health.” Additionally, the strategy references a forthcoming specialty-focused longitudinal care model within MA and Medicaid, signaling intentions to drive multi-payer alignment.
Saving Federal Tax Dollars. Another major aspect of the strategy is “protecting federal taxpayers.” This goal reflects a continued emphasis on total cost of care accountability and indicates a more aggressive shift to downside risk. The Innovation Center says it will “require all models to have downside financial risk and require providers to assume some of the financial risk..” Additional provisions of protecting tax dollars include reducing role of state governments in rate setting, simplifying model benchmark methodology, and ensuring “proper and nondiscriminatory provision of funds for health care services.”
What to Watch
For healthcare organizations, the Innovation Center’s agenda signals a need to prioritize consumer-centric models. Hospitals, providers, and insurers should anticipate the following:
- Increased focus on preventive care initiatives to align with new model designs
- More robust data-sharing and technology requirements, meaning investments in patient-focused digital tools will become essential
- New opportunities in MA, given potential payment model innovations affecting plan structures and risk-adjusted reimbursement
Healthcare stakeholders should monitor possible developments related to the strategy.
- While details on specific strategies have yet to emerge, the Innovation Center indicated it plans to provide more information on new models, as well as changes to existing models, in the coming months.
- The Innovation Center has not provided a goal akin to the previous administration’s effort to have 100 percent of Medicare beneficiaries in accountable care relationships by 2030. It is still unknown whether these goals are forthcoming or if this will remain vague.
- Stakeholders are still awaiting clarity on changes to existing models, including key models set to conclude at the end of 2026 (i.e., ACO REACH and Kidney Care Choices).
- Strategy language indicates that the agency may develop payment innovation in prescription drugs, medical devices, and technology.
Connect With Us
The Health Management Associates Annual Conference, Adapting for Success in a Changing Healthcare Landscape, October 14-16, 2025, in New Orleans, LA, will feature discussions on how the new strategy is reshaping the healthcare system and care delivery for patients, particularly the opportunities to revisit provider contracts with MA plans and to integrate technology to advance the prevention of chronic conditions and achieve population health goals.
For more information about the opportunities and considerations the Innovation Center agenda presents for your organization, contact HMA’s featured experts below.
