HMA will be offering analyses on various investor related topics in the healthcare sector. Our first report examines the growth of Artificial intelligence (AI) in the US healthcare market. AI is expected to reach projected revenues of $102 billion by 2030. Learn more in this analysis.
1307 Results found.

Navigating Uncertainty in Medicare and other Federal Health Programs
As we approach Medicare’s 60th Anniversary this July, the program again finds itself at a critical crossroads, facing demands for higher quality care, expanded access to transformative treatments, and streamlined patient access to their medical information. Decision makers also must integrate digital tools into clinical models, address mounting scrutiny of costs, and ensure accountability for outcomes influenced by social determinants of health.
This period of transition at the Federal level is bringing new scrutiny and pressure for efficiency. With more than 68 million beneficiaries, nearly half of whom are enrolled in Medicare Advantage, the Medicare program is continually evolving to respond to shifting policies and priorities. Organizations that stay ahead of policy changes will be best positioned for success and drive meaningful improvements for Medicare beneficiaries.
When you work with HMA’s federal policy experts, you get access to former CMS officials and plan executives, payment system and coding experts, and policy analysts to support your efforts. HMA’s Medicare team includes experts specializing in Medicare Advantage, dual eligibles, Medicare stars, value-based care, rural health, PACE, actuarial support, and data and quality. We draw on the resources of experts from our HMA companies to provide comprehensive and end-to-end solutions. Read some of our insights in the links below.
Here’s how HMA is helping clients navigate this dynamic landscape:
- Our policy team is working with clients to understand what is happening right now in Congress and in the US Department of Health and Human Services that will usher in significant policy and funding changes. Our teams are advising stakeholders on the short- and long-term implications, strategies to advance their objectives in this new environment, and working with states to understand immediate impacts on local financing.
- Our clinicians are working closely with insurers, providers, and health systems to strengthen models of care that address complex conditions, behavioral health issues, long-term services and supports and unique needs of special Medicare populations.
- Our actuaries are conducting financial modeling and analysis to forecast costs, revenues, and potential outcomes to help navigate financial uncertainties in Medicare Advantage bids, Medicare payment models, and emerging environmental and regulatory issues, including digital quality measure collection, increased focused on dual integration, supplemental benefits, and drug price negotiations.
- Our digital quality experts are working with healthcare organizations to prepare for rapid changes that digital health quality measurement will bring to reimbursement models. Our teams are advising on the influx of newly accessible clinical data to ensure it is properly validated and interpreted and working with insurers and providers to develop strategies allowing them to be more agile in contract negotiations.
To talk to an expert to help support and improve your Medicare programs, contact Greg Gierer with the HMA DC office ( [email protected]) or Josh Trent with the Leavitt Partners DC office ([email protected]).
For more cutting-edge information check out some of our recent insights:
Policy & Regulatory Strategies: Legislative, regulatory, reimbursement, and budget analysis from experienced former staffers from CMS and various legislative committees. The HMA policy team includes past HHS officials like Amy Bassano and Monica Johnson, as well as the team at Leavitt Partners.
- Webinar Replay — Legislative Reconciliation in a New Era: Understanding Its Role and Impact in the 119th Congress
- Podcast — Has Medicare’s Drug Policy Struck the Right Balance Between Access and Cost?
- Webinar Replay — 2024 Political Checkpoint
- Webinar Replay — The 2024 Election: What It Could Mean for Health Policy
- Report — On Rare Disease Day, HMA releases new report analyzing federal spending on Orphan Drugs
Actuarial & Financial Analytics: Leading actuaries with deep MA experience and robust tools to support innovative benefit and pricing strategies. Encounter data audits to improve risk scores. The HMA Actuarial team includes Wakely Consulting Group and Cirdan Health Systems and Consulting.
- PACE Plans and The Changing Risk Environment
- Webinar Replay — 2025 Medicare Advantage Bids Are Over. Now What?
- Project Spotlight — CMS Encounter Data Quality Review for an I-SNP Plan
Communications & Engagement: Creative campaigns to inform, persuade, and engage providers and payers. The HMA team includes 720 Strategies and Lovell Communications.
- Web campaign — American Association of Nurse Practitioners
- Website — Five Paid Digital Tactics You Need for Advocacy
Strategy & Transformation: Strategy & analytic fundamentals informed by variety of experts in Medicare, health insurance, care delivery for older and vulnerable populations, and value-based payment and delivery innovations.
- Podcast — Can data shape the future of Medicare’s value proposition?[TM6]
- Using Virtual Research Data Center (VRDC) Data to Answer Big Questions
- Report — Analyzing the Expanded Landscape of Value-Based Entities: Implications and Opportunities of Enablers for the CMS Innovation Center and the Broader Value Movement
Operations & Implementation: Clinical and administrative operations building care models, implementing value-based payment incentives, technology, and compliance. The HMA Managed Care team is led by Holly Michaels Fisher.
Quality Outcomes & Research: Integrated approach to STARS ratings, building digital quality management tools and strategies for compliance and accreditation. The HMA team includes Caprice Knapp and Sarah Scholle.

Digital Quality Measurement: A Key Driver to Value
HMA Spotlight
Digital Quality Measurement: A Key Driver to Value
The healthcare industry is on the cusp of a seismic shift in how quality data are collected, analyzed and reported. Beginning in January 2027, new federal interoperability and prior authorization rules will require widespread data exchange, paving the way for full digital quality measurement (dQM) by 2030. This move toward dQM presents enormous opportunity to enhance quality outcomes, strengthen value-based arrangements, and streamline operations. However, it also requires substantial strategic, operational, and technological changes that most organizations simply cannot manage alone.
Regulatory Mandates
Organizations that delay preparing for the 2027 rule risk costly setbacks and non-compliance.
Opportunity for Transformation
dQM drives efficiency and quality improvement, supporting population health initiatives, care coordination, and value-based contracting.
Complexity and Risk
dQM implementation spans multiple departments—IT, quality improvement, analytics, legal, and more—creating a host of challenges requiring specialized expertise.
Competitive Advantage
Early adopters will have a first mover advantage. This advantage could result in revenue associated with auto-assignment, STARS bonus, value-based purchasing, reduced sanctions and fine, etc.
Why Partner with HMA?
HMA’s dQM consulting team understands the operational, clinical, and technical dimensions of transitioning to digital quality measurement. Leveraging deep expertise across health plans, provider organizations, and state and federal agencies, we help you plan, implement, and evaluate your dQM strategies at every stage.
1. Speed to Solution
- Front-Seat Knowledge: HMA, together with Leavitt Partners, an HMA Company, is actively influencing and shaping national conversations on interoperability and digital measures. Our front-line insights mean you gain rapid access to the latest best practices, regulatory updates, and strategic guidance.
- Streamlined Roadmap & Implementation: We help you develop a clear, achievable plan of action—saving you from the pitfalls of trial-and-error by fast-tracking your implementation and monitoring the results.
2. Cross-Department Coordination
- Complexity of Transformation: dQM requires alignment across IT, quality, clinical operations, and finance—often a monumental undertaking for organizations already at capacity. Robust change management & strategic planning and communications is crucial for success.
- Meet Mandated Timelines: Waiting to act can result in financial risk, stressed operations, and missed opportunities to optimize reimbursement.
- Manage Risk: Because digital quality measurement is in an emerging phase, organizations face higher levels of uncertainty. HMA mitigates risk by leveraging our extensive experience and industry partnerships.
3. Proven Expertise and Ongoing Support
- Full Project Lifecycle: From early planning and strategy development through implementation and evaluation, we stand by you every step of the way.
- Value Beyond Compliance: Our team identifies how dQM can drive broader business goals—improving population health, care coordination, and value-based contracting performance..
Ready to Transform Your Quality Measurement?
HMA’s expert consultants provide the advanced technical, business, and operational skills you need to succeed in today’s rapidly evolving regulatory landscape. Don’t let the complexity of dQM derail your strategic plans or burden your teams. With HMA as your partner, you can confidently navigate and optimize your transition to digital quality measurement.
Take the first step toward harnessing the power of digital quality measurement. Partner with HMA to position your organization for success today—and well into the future.
Contact our HMA dQM experts to discuss your organization’s goals and challenges:









CMS Shakes Up the Innovation Center Model Landscape: What Comes Next?
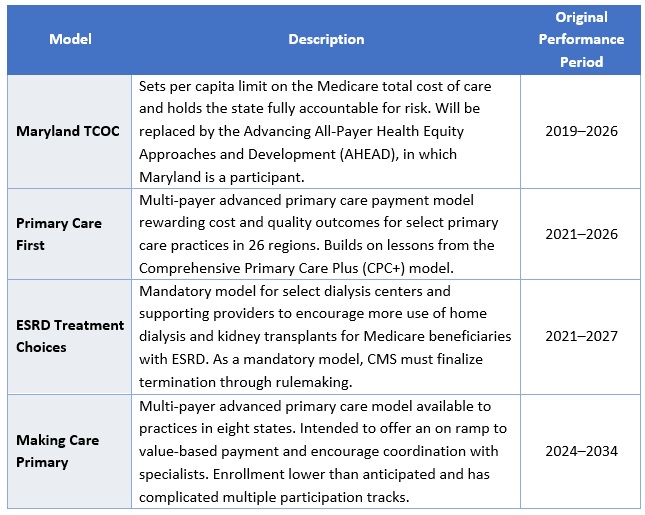
This week, our In Focus section focuses on a March 12, 2025, announcement from the Centers for Medicare & Medicaid Services (CMS) regarding CMS Innovation Center programs under the new Administration. After reviewing the Innovation Center’s model portfolio, CMS has elected to discontinue four models ahead of their original end dates: Maryland Total Cost of Care (TCOC), Primary Care First (PCF), End-Stage Renal Disease (ESRD) Treatment Choices (ETC), and Making Care Primary (MCP). The agency also intends to downsize the Integrated Care for Kids Model (InCK) and forgo the launch of two drug pricing initiatives. According to the announcement, CMS appears to be moving forward with other Innovation Center models, but signaled upcoming modifications to models to align with Administration priorities as well as new model announcements.
The following is a discussion of CMS’s announcement and what it may signal about the agency’s commitment to value-based care, key takeaways regarding the four terminated models, and how stakeholders should be preparing to engage with the Innovation Center on current or future models while we await additional details.
CMS’s Strategic Decision
As part of CMS’s recent announcement about the model terminations, the agency reaffirmed its support for testing models that reduce program spending while maintaining or improving quality of care. Furthermore, the Innovation Center “plans to announce a new strategy based on guiding principles to make Americans healthier by preventing disease through evidence-based practices, empowering people with information to make better decisions, and driving choice and competition.” These statements should be seen as a commitment to using the Innovation Center to test new approaches to delivering care but with an expectation that the models will need to demonstrate significant cost and quality improvements as outlined in its statutory authority. According to CMS, the cancellation of these models is projected to save an estimated $750 million.
Because CMS said it may modify additional models in the future, it is reasonable to expect those changes will focus on achieving a higher level of savings or to see savings earlier in the demonstration, as well as aligning model design with the priorities of this Administration. The potential modifications could have an impact on the number of model participants, length of model testing, and financial arrangements, especially with regard to risk and quality improvement approaches.
Models Ending
CMS Innovation Center models are time-limited pilots meant to help the agency test which types of interventions lead to cost savings and improved quality and, if successful, can be scaled on a nationwide basis. These models are evaluated regularly, and CMS has the authority to modify or terminate models if they fall short of the statutory criteria.
The four models the agency plans to terminate are ending for various reasons (e.g., underwhelming performance, forthcoming replacement by successor model, etc.) and, as stated above, the decision should not be seen as a retreat from value-based care, but rather as a signal regarding Administration priorities for Innovation Center models. For example, despite terminating PCF and MCP prior to their original end dates, CMS reaffirmed its support for primary care as a “foundational component of the Center’s strategy” and that future primary care payment reforms will focus on approaches that produce savings. CMS also noted that ending these models early offers an opportunity to move beneficiaries into more permanent programs, such as the Medicare Shared Savings Program (MSSP)—CMS’ flagship accountable care initiative—even going so far as to direct readers to the MSSP’s calendar year 2026 application.
CMS plans to advise current model participants of other options for advanced primary care payment before the models conclude by December 31, 2025. Table 1 presents information on the models scheduled for early termination.
Table 1: Models Ending by December 31, 2025
In addition, the agency is considering options to reduce the size of the InCK model and will no longer pursue the Medicare Two Dollar Drug List and Accelerating Clinical Evidence models. The latter two initiatives were included in a Biden Executive Order on drug pricing and were not implemented. Notably, CMS did not end another drug pricing Innovation Center model, Cell and Gene Therapy Access (CGT) Model.
Innovation Center’s New Strategic Plan
CMS also announced that it will soon release its new vision for the Innovation Center, based on principles designed to improve Americans’ health through evidence-based practices, empower individuals with decision-making information, and drive competition.
This vision will set the direction for future value-based care initiatives and reflect the leadership changes within CMS, including the anticipated confirmation of Mehmet Oz, MD, as CMS Administrator and the appointment of Abe Sutton, as the new Director of the Innovation Center. Mr. Sutton’s experience with value-based care—especially during his time as an advisor to then Department of Health and Services Secretary Alex Azar under the first Trump Administration and his subsequent private sector leadership of value-based companies—positions him to play a key role in shaping CMS’s future efforts.
Stakeholder Considerations
Stakeholders have several critical operational decisions and strategic considerations to address, including:
- Transition Support. Participants in the models scheduled to end must assess their options for sustaining certain components of the payment models without Innovation Center support. This effort will require strategic, operational, and financial analyses to make informed decisions.
- Evaluation of Other Programs. While the Innovation Center has signaled its intentions of announcing new models, participants should not wait to evaluate options. The Administration plans to prioritize permanent payment programs and will continue to support the MSSP as CMS’s permanent model for accountable care organizations (ACOs). Stakeholders interested in participating in the MSSP in 2026 must act quickly to assess their organizational readiness, conduct financial modeling of their potential benchmark and performance, evaluate potential partners, and prepare for the application process. Both existing and new ACOs should be exploring their strategies and infrastructures to optimize performance.
- Adapting to Changes in Existing Models. While CMS discontinued select models, it is likely the agency will make additional changes to the Center’s continuing models. These revisions likely will reflect President Trump’s executive actions and policy priorities. With the increased focus on cost savings, CMS may choose to spend fewer resources on model implementation, including participant support and model engagement.
- Policy and Market Intelligence. Monitoring the dynamic federal policy landscape and seeking strategic advisory support can help stakeholders navigate and inform potential future federal and state alternative payment model opportunities. Stakeholders should expect that existing and potential new models may have stricter requirements and higher expectations for financial risk. Providers, states, insurers, and other interested stakeholders should monitor public and private sector developments to understand the landscape and evolving opportunities.
Connect with Us
Health Management Associates, Inc. (HMA), is home to alternative payment model experts that can assist stakeholders in responding to changes in Innovation Center models and the agency’s approaches and to help prepare for participation in future model opportunities. Additionally, HMA produces a weekly briefing focused on public and private sector VBP-related news. To learn more about how HMA can support your organization’s federal engagement and innovation strategy, contact our experts below.

What Strategies Help Local Governments Stay Resilient Amid Health Policy Changes?
John Eller, managing principal at Health Management Associates, joins Vital Viewpoints on Healthcare to discuss the critical role of resilience in local health services. As communities navigate shifting federal policies, economic uncertainty, and natural disasters, John shares insights on how agencies can remain nimble, collaborative, and innovative. Drawing from his extensive experience in Medicaid transformation, behavioral health, and social services leadership, he highlights the power of community trust and cross-sector partnerships in maintaining stability during turbulent times.

New Insights on Medicaid Spending: An Analysis of Disaggregated Managed Care Spending
Medicaid is a federal/state health insurance program that served more than 86 million lower-income people in fiscal year (FY) 2021. The combined federal and state spending for Medicaid totaled $717 billion that year, $420 billion of which was spent on providing care to Medicaid managed care organization (MCO) members, and $297 billion on services provided to fee-for-service enrollees.
- While the role of managed care in Medicaid has grown tremendously over the past decade, with MCOs covering nearly three-quarters of Medicaid enrollees, detailed cost information has not been estimated for the people with MCO coverage. These data historically have been available only for fee-for-service (FFS) Medicaid because of limitations on federal data sources.
- This lack of data blocks our understanding of the relative magnitude of the cost drivers in the program and contributes to an uninformed debate about policy reforms to control the growth of spending and improve quality of care.
- Obtaining and using cost data by provider type for MCOs can help answer questions such as how much funding do MCO enrollees with diabetes, asthma, and/or hypertension consume? Of these patients, how many also have behavioral health conditions? How many MCO enrollees have six or more emergency department (ED) visits during a year and/or multiple inpatient hospital stays, and what does their resource consumption look like?
Health Management Associates (HMA) has developed a reliable methodology that can be applied to all 50 states, which approximates spending for the major categories of health services that MCOs cover, including: inpatient and outpatient hospital care, physician and other professional services, skilled nursing facilities, clinics, pharmaceuticals, and other services. HMA can determine prices for these services, which, combined with data on the number of encounters, yields reliable cost figures. These cost estimates will be useful in identifying unmet medical needs, gaps in our delivery systems, and areas of high spending where efficiencies and timely care management can be added to slow the growth in total health spending.
Navigating CMS’s 2025 Marketplace Rule: What It Means for ACA Marketplaces, Insurers, and Consumers
This week, our In Focus section also reviews the 2025 Marketplace Integrity and Affordability Proposed Rule, released by the Centers for Medicare & Medicaid Services (CMS) on March 10, 2025. The proposed rule calls for enhancing program integrity protections in the Affordable Care Act (ACA) marketplaces through targeted changes to eligibility and enrollment policies and procedures.
This proposed rule aligns with the overarching policy priorities President Trump has identified, including reducing federal costs and reforming policies related to immigrants. It also takes aim at fraud, waste, and abuse practices in the ACA Marketplaces, which is the cornerstone from which the US Department of Health and Human Services explains and justifies its proposed initiatives.
Notably, the proposed changes will occur alongside other potential federal policy revisions, including the December 31, 2025, expiration of the ACA enhanced subsides for consumers, which led to historically high coverage levels—nearly 24 million people were enrolled in the Marketplace as of January 2025. The combined changes will have a varied but significant effect on all state health insurance markets, creating a need for scenario planning and preparation to start immediately.
CMS is providing the public 30 days to submit comments on the proposed rule. An overview of the proposed changes and key considerations follow.
Rule Components
Enrollment Timeline: CMS proposes shortening the open enrollment period for all individual market coverage, including for state-based marketplaces (SBMs), which traditionally have had flexibility to set later enrollment deadlines. If finalized, open enrollment will begin November 1 and end December 15, a month earlier than the current deadline of the following January 15.
Income Verification: The rule would require marketplaces to bolster their income verification processes to protect against manipulation of the authorization and calculation of advance premium tax credit (APTC) values. CMS policymakers believe these changes will be useful in addressing broker and consumer fraud and abuse of the APTC eligibility process. Proposed income verification changes include requirements that people provide the documentation of their income if they meet the following criteria:
- The income on their application is between 100 percent and 400 percent of the federal poverty level (FPL), but the income returned from external data sources show they make less than 100 percent of the FPL
- No tax data are available from external data sources to confirm the applicant’s self-attested income
Applicants who do not verify their income will have it adjusted to align with the income returned from external data sources, and their APTC eligibility will be updated accordingly. In some cases, such as when no returned income data are available, these individuals will become ineligible for the APTC.
CMS also plans to reinstate a 2015 policy that requires marketplaces to designate applicants or enrollees as ineligible for APTCs if they fail to file and reconcile their APTC on their federal income taxes. This requirement is known as the failure to file and reconcile (FTR). The Biden Administration changed the FTR requirements to find enrollees ineligible for APTCs if they fail to file and reconcile for two consecutive tax years.
Lastly, CMS proposes eliminating the additional 60 days consumers are granted to resolve income inconsistencies. Today, most marketplace consumers have up to 150 days to resolve income inconsistences. This proposal would return to the 90-day verification period that was in place prior to the Biden Administration.
CMS also requests input on alternative redetermination and re-enrollment policies for fully subsidized consumers, including whether $5 is the appropriate premium amount or should be higher or if fully subsidized consumers should be required to actively confirm their eligibility and reenroll every year.
Another proposal would remove the ability for marketplaces to automatically reenroll Bronze members who are eligible for a cost-sharing reduction (CSR) in a Silver plan if the Silver plan has the same provider network, is in the same product, and has a lower or equivalent net premium as the consumer’s Bronze plan.
Special Enrollment Period Changes: CMS is proposing multiple changes to special enrollment periods (SEPs), including the removal of monthly SEPs for individuals with household incomes that are projected to be at or below 150 percent of the FPL and a requirement that marketplaces verify eligibility for at least 75 percent of new enrollments during SEPs. CMS also proposes adopting a pre-enrollment income verification model for SEPs.
- Bar Deferred Action for Childhood Arrivals (DACA) recipients from QHPs in the Marketplace and basic health programs, making them ineligible for APTCs and CSRs and returning to pre-Biden era DACA eligibility rules
- Remove gender-affirming care as an essential health benefit
- Allow insurers to require payment of past due premiums before effectuating new coverage, if state law permits
- Increase cost sharing/lower premiums by increasing the maximum out-of-pocket limit and widening de minimis ranges
Implications
CMS is reverting to several policies that were put in place during President Trump’s first term, increasing the likelihood that CMS will finalize many of the changes as proposed or with minimal modification.
Insurers, SBMs, insurance departments and other stakeholders should engage in the federal policymaking process and begin planning immediately for the financial and operational changes that will be required to comply, as several of the requirements will take effect as soon as the rule is finalized. Stakeholders will also want to consider the direct impact on consumers.
Health Management Associates (HMA) Marketplace experts identified the six key considerations for stakeholders:
- Market share and risk. The proposed changes are projected to decrease Marketplace enrollment and Insurers and states need to plan for shifts in their market and consider approaches to manage these changes.
- Administrative operations. A shorter enrollment period and additional eligibility and enrollment requirements may increase administrative actions for enrollees, insurers, and marketplaces. Examples include:
- Marketplaces will need to make system and operational changes to comply with the new income verification, SEP, and open enrollment period requirements.
- Departments of Insurance may need to adjust their rate and form filing instructions and timelines to give insurers the clarity and time they need to comply with new requirements.
- Consumer education. Insurers and marketplaces will need to consider the effectiveness of their marketing and outreach and education strategies, given the shorter open enrollment period.
- Interactions with the expiration of the enhanced subsidies in 2026. The Congressional Budget Office estimates that the uninsured population will increase by 2.2 million in 2026 and up to 3.8 million by 2028 if the enhanced ACA subsidies expire. While it is too early to project or measure the impact of this proposed rule and the expiring subsidies, together they undoubtedly will have direct impacts on eligibility, enrollment levels, market dynamics including pricing and risk mix, and the overall stability of the Marketplaces in the long term. Congress may also take action on other policies related to Marketplace stability for which stakeholders should prepare.
- State-level mitigation. States interested in mitigating the impacts of this proposed rule, as well as the expiring subsidies, will need to consider legislation to address the resulting affordability gaps and coverage losses. For example, states may look to state-funded subsidy wraps or reinsurance programs to minimize the net premium rate increases that most Marketplace plan members will experience when the enhanced subsidies expire in 2026.
- Federal engagement. CMS is providing the public 30 days to comment on the proposed rule. This provides stakeholders the opportunity to voice their positions on the impact of this and future Marketplace policies. Comments on the proposed rule may also be shared with congressional policymakers and staff to help shape future legislative proposals.
HMA experts have considerable experience working with marketplaces, Departments of Insurance, insurers, and federal policymakers with jurisdiction over the Marketplace. They work with these entities to inform, analyze, and influence federal policies and conduct impact analyses on pricing, enrollment, administration, and operations. HMA also provides strategic and project management support for the implementation of finalized policies.
To learn more about how the proposed rule and the scheduled sunsetting of enhanced subsidies may affect your organization contact HMA Marketplace experts below.
New Insights on Medicaid Spending: HMA Analysis of Disaggregated Medicaid Managed Care Spending
This week, our In Focus section highlights insights from a new Health Management Associates (HMA), issue brief, “New Insights on Medicaid Spending: An Analysis of Disaggregated Managed Care Spending.” Until now, most Medicaid cost data have focused on enrollees in fee-for-service (FFS) programs. HMA used the Centers for Medicare & Medicaid Services (CMS) Transformed Medicaid Statistical Information System (T-MSIS) database to analyze Medicaid managed care organization (MCO) spending in major categories of healthcare, including inpatient and outpatient hospital care, physician and other professional services, skilled nursing facilities (SNFs) and home and community-based services (HCBS), clinics, pharmaceuticals, and other services. HMA’s methodology can be applied to all 50 states and allows us to determine prices for these services, which, combined with data on the number of encounters, yields reliable cost figures.
Findings
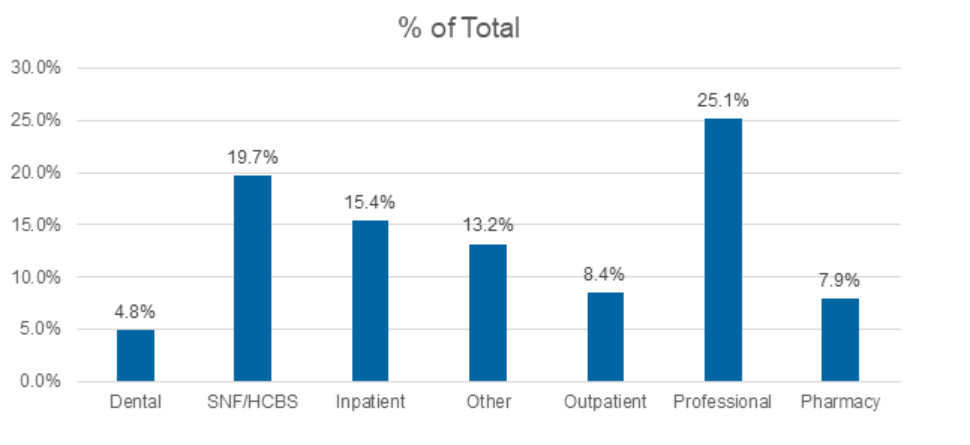
Medicaid managed care accounted for $420 billion of the total $717 billion in Medicaid spending for federal fiscal year 2021. Professional claims accounted for the largest portion of Medicaid spending, totaling 25.1 percent, followed by SNFs at 19.7 percent, and inpatient claims at 15.4 percent.
Figure 1. T-MSIS Medicaid Spending by Service Category 2021 (MCO Disaggregated plus FFS)
What’s Next
This analysis can be replicated for subsequent years and will provide important information on Medicaid spending trends. This work also sets the stage for analyses and comparisons of cost categories by variables such as eligibility category (e.g., dual eligibles, children, parents, adults without children, the Medicaid expansion population, and designated as aged/frail/disabled); race and ethnicity; frequent users of hospital services; and people with multiple chronic illnesses. This type of analysis allows us to answer fundamental questions about the Medicaid program and can pinpoint areas of high need within the Medicaid population, such as:
- How much do we spend on services for people with diabetes?
- How much do we spend during childbirth/first year of life and in the last year of life?
- How much do we spend for Medicare-Medicaid dual eligibles?
Data-informed discussions on these and other topics can help identify opportunities for efficiencies and timely care management to slow the growth in total healthcare spending. This information will provide important context for the policy debate, offering a full view of the relative magnitude of the major categories of Medicaid spending.
Connect with Us
Medicaid providers, MCOs, states, and policymakers all have an interest in identifying high-cost drivers of Medicaid managed care. The methodology applied in the analysis for the HMA issue brief can be applied and adapted for future analysis.
For details about this analysis, its implications for state and local policies, and additional research using T-MSIS, contact our experts below.

March 19, 2025
New Insights on Medicaid Spending: HMA Analysis of Disaggregated Medicaid Managed Care Spending
Join the Call to Action to Address the Behavioral Health Workforce Crisis
The behavioral health workforce crisis, a long-standing issue worsened by the COVID-19 pandemic, threatens the ability of provider organizations to meet growing demands for behavioral health treatment services. Despite decades of efforts, challenges such as inadequate compensation, workforce shortages, lack of diversity, and high burnout persist. In fact, a 2023 survey of state Medicaid officials on behavioral health revealed that nearly every state was engaged in at least one strategy to address the workforce shortage.[1]
Since 2021, The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked to create both short and long-term solutions. Efforts have included:
- Policy papers aimed at short term solutions
- Review and crosswalk of over 400 recommendations from organizations across the country
- Creation of the Workforce Solutions JAM, begun in May 2024, a monthly webinar spreading innovation and discussing all elements of the behavioral health workforce
- Multiple convenings of technical experts and partners to discuss how to support action on the workforce
- And now a call to action.
The next step for the Workforce Solutions Partnership is to expand engagement with partners to address the workforce shortage. The Partnership believes that using the Collective Impact framework, will provide the structure to build a national strategy and cross-sector approach to shared implementation of workforce initiatives, resulting in effective and scalable solutions. We understand there are countless workforce initiatives underway across the country, many of which are demonstrating progress and innovations that can be scaled. Rather than duplicate or distract from existing efforts, the Partnership will build connections between these efforts, elevate their impact and empower emerging innovative ideas.
Initial areas of focus will include:
Community alignment: Enhancing recruitment and retention of a workforce that reflects the communities accessing behavioral health services.
Creation of efficiencies: Building a new operational and administrative model that improves access.
Technology integration: Exploring tech-enabled supports to enhance skill development and service delivery.
Career pathways and compensation: Improving access to career opportunities and using evolving payment models to increase salaries for behavioral health professionals.
The Call to Action outlines the Partnership common agenda, levers of change, and the process for developing a national platform for change. It outlines how partners can engage and is the launch of what we hope will be national action to build a sustainable workforce.
[1] Saunders, H., Guth, M., & Eckart, G. (2023). A look at strategies to address behavioral health workforce shortages: Findings from a survey of state Medicaid programs. Kaiser Family Foundation. https://www.kff.org/mental-health/issue-brief/a-look-at-strategies-to-address-behavioral-health-workforce-shortages-findings-from-a-survey-of-state-medicaid-programs/
Workforce Solutions Partnerships: Call to Action to Build a Sustainable Behavioral Health Workforce
The Workforce Solutions Partnership, a collaboration of The National Council for Mental Wellbeing, The College for Behavioral Health Leadership, and Health Management Associates has worked since 2021 to create both short and long-term solutions addressing the behavioral health workforce crisis. In this whitepaper, we issue a Call to Action to partners across all sectors to join us in this effort to drive pervasive change and ensure the future of behavioral health care. We need you to help us create and define the future of the workforce and envision a new system of care. This paper outlines the problem and highlights the efforts developed by our partnership, and mechanisms that can help to address the problem.