Our March 19, 2026, Connecting the Dots analysis described the federal requirements and the operational questions states and partners will need to answer to effectively implement Medicaid work and community engagement requirements. Since then, federal officials have advanced their forthcoming regulation to the final stage of review and intend to meet the statutory requirement to release interim final guidance by June 2026. In addition, many states have taken early steps to communicate upcoming changes and begin planning for system, policy, and partner readiness.
While state sessions are clearly grabbing a lot of energy, timing of pulling together many of the moving parts is becoming a concern as states undergo one of the most fundamental operational challenges to the Medicaid program since its inception. This article synthesizes emerging approaches and identifies practical opportunities to refine strategies and strengthen readiness while minimizing burden for enrollees and state Medicaid agencies.
Early Actions in States Preparing to Implement Work and Community Engagement Requirements
1. States Are Launching Websites that Highlight Coming Changes
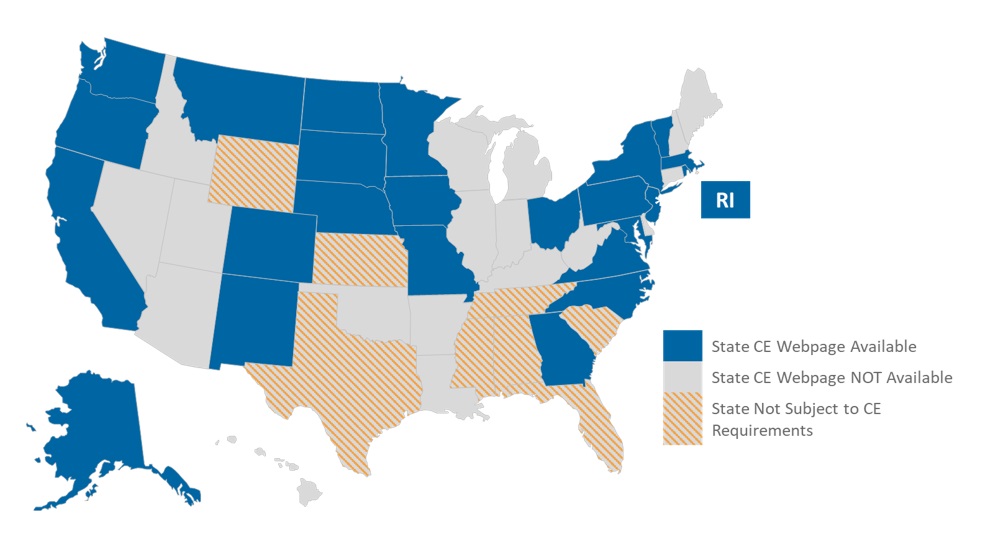
As of April 2026, more than half of US states that are subject to the Medicaid work and community engagement requirement had posted web page content describing forthcoming changes associated with the 2025 budget reconciliation act (P.L. 119-12, OBBBA). Some websites provide high-level descriptions of key provisions (e.g., qualifying beneficiary ages, qualifying activities, and exemptions), while others include more detailed information reflecting state-specific policy decisions, educational messages, and suggested steps that beneficiaries, providers, managed care plans (MCPs), and community-based stakeholders can take now (see Figure 1).
Figure 1. States with a Community Engagement Web Page
For example, Ohio’s website describes the requirements for, and provides examples of, acceptable documentation Medicaid members may use to demonstrate compliance or eligibility for an exemption. Ohio also offers a “Communications Partner Packet” that contains frequently asked questions (FAQs) and draft outreach materials to support stakeholder communications and increase awareness. The communications tools include a one-page flyer, a rack card, and potential social media posts to raise awareness of the changes, with some use of QR codes to enhance quick access to key websites like the beneficiary self-service portal.
2. States are Beginning to Make and Communicate Preliminary Policy Decisions
States must make a range of policy decisions, including the penalty start date, the number of required months of compliance for both the initial application and subsequent renewals, the potential adoption of short-term hardship exceptions, and how exceptions are defined and operationalized. While most states anticipate compliance beginning January 1, 2027, in alignment with OBBBA, Nebraska and Montana have announced plans to begin implementation in 2026, and their websites reflect additional policy details to support accelerated timelines.
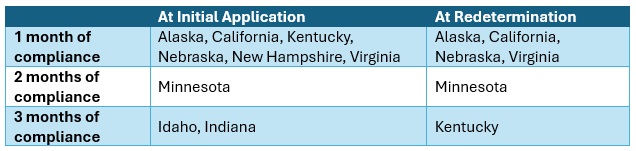
A handful of states, including Arkansas and Ohio, also are communicating ahead of OBBBA’s timeline to promote awareness and engagement before the work and community engagement requirement becomes effective. Table 1 summarizes examples of the current state planning[1] around the number of required months of compliance for the initial application and renewals.
Table 1. Sample Number of Months in Compliance
States also are taking different approaches to exemptions and short-term exceptions. Although many exemptions and exceptions are defined in statute, the interpretation of “medically frail” remains an area in which states have significant flexibility, with implications for how many individuals are exempt. Many states have experiences with establishing definitions of medically frail. For example, states that offer an adult benefit package that differs from the state plan benefit package must allow medically frail adults to opt in to the state plan. At least 12 states already make medically frail determinations, and these existing policies and processes may inform approaches for work and community engagement requirements.
One of those states—Nevada—has posted a proposed definition of medically frail with a request for public comment, including a sample list of qualifying medical conditions. Although such lists can provide clarity, they also underscore the importance of a clear and straightforward exemption request process to support appropriate determinations, including for individuals with conditions that are omitted from a specified list.
3. States Are Securing Additional Support to Address Administrative Challenges
The new eligibility criteria, coupled with more frequent eligibility checks, are placing substantial new demands on Medicaid agencies, eligibility systems, and personnel. In response, states are considering or actively pursuing a range of approaches to strengthen administrative capacity. Examples include:
- Hiring new state eligibility and enrollment workers: Indiana and Montana
- Funding system enhancements and improvements: Alaska and New Jersey
- Hiring outreach and engagement contractors: Arizona and Arkansas
States are also proposing to take a more coordinated, cross-agency approach that uses other state agencies and programs as data sources and referral pathways to help beneficiaries meet their work and community engagement requirements. A variety of states are looking to leverage data from their Supplemental Nutrition Assistance Program (SNAP) program to facilitate compliance checks, and Kentucky has proposed receiving data from a variety of sources (e.g., Department of Revenue, Department of Corrections, Unemployment Insurance, Vital Statistics, and others) to more automatically identify eligibility and exemption changes.
States like Hawaii, Montana, and Nebraska have highlighted their labor departments to connect people to job and community service resources. Virginia’s work and community engagement website directs the public to a series of different programs based on whether they are interested in employment, volunteer, or education resources. Minnesota also has introduced legislation proposing collaboration between the commissioner and county agencies to link beneficiaries to other critical services like job training, childcare, and transportation.
Shrinking federal contributions and constraints on Medicaid revenue strategies—such as limits on provider taxes—are prompting states to rethink how Medicaid agencies operate within existing budgets. Limited federal funding to support administrative needs elevates the importance of efficiency, coordination, and automation.
What States Might Do to Chart a Better Path Forward
A robust pre-implementation plan is critical to successful work and community engagement implementation. A well-documented plan helps states fully document the variety of moving parts across policy, systems, and partners, clarify milestones and decision points, and define what readiness looks like in practice.
Key components of a pre-implementation plan may include:
- Signing agreements and contracts to support infrastructure. Pre-implementation planning should ensure that appropriate support from third-party vendors and sister agencies is secured to optimize flexibilities and manage the requirements. Examples may include maintenance of effort (MOE) agreements, memoranda of understanding (MOU), contract updates, and requests for proposals (RFP) as appropriate. States may need to use expedited contracting vehicles when available and maximize existing vendor arrangements. Agreements should address data governance, privacy, and cost allocation issues to support smooth operational integration and reduce downstream friction.
- Quantifying and automating exemptions. Systems and reporting should be updated to identify, notify, and manage cases for expansion adults who are likely exempt. Leveraging additional resources and data matching may help states identify common exempt populations, such as caretakers with dependents under age 14, disabled veterans, and pregnant women without requiring additional verification. Understanding the demographics of the remaining nonexempt population may also be useful in outreach, education, and links to supports.
- Preparing for readiness review, including system readiness, coverage transition, and churn management. Pre-implementation plans should prioritize robust system testing, staff training, and timely updates to required documentation (e.g., state plan amendments, policy and member manuals, notices, and reviewing and approving MCP communications). Building in clear transition supports for individuals who may lose coverage or transition to other coverage options can improve continuity of coverage, reduce uninsurance and uncompensated care, and limit administrative burden following implementation.
- MCP contracts. Most enrollees subject to work and community engagement requirements are enrolled in Medicaid MCPs. States will need to describe enhanced roles and responsibilities in both the MCP contracts as well as the rates. Clear contract expectations can support transparency and mutual accountability across partners.
- Test communications with the target audiences to ensure understanding and appropriate action. Awareness of the new work and community engagement requirement was one of the biggest challenges Arkansas faced when it launched its program in 2018. Beneficiaries also struggled to understand whether the requirement applied to them and what they needed to do to comply. States must build communications plans and messaging to clearly address these issues to reduce the number of beneficiaries losing coverage simply because they did not understand the new requirements.
Connect with Us
Health Management Associates (HMA) Medicaid experts assist Medicaid and state policymakers with the following:
- Strategic positioning
- Policy-to-operations design
- Cross-agency governance and partner alignment
- Information systems impact assessment, change planning, testing strategies and readiness metrics
- Scenario planning and beneficiary impact analysis
- Communications and operational playbooks
- Program integrity, reporting, and audit support
HMA Medicaid experts can also assist MCPs, providers, and community-based organizations with:
- Risk assessments (e.g., enrollment, utilization, and spending impacts)
- State-specific policy and operational insights and trends
- Communications, outreach, and engagement strategies and content
- Member retention strategies
- Grassroots workforce development and community engagement strategies
For questions, contact HMA contributors to this article Lora Saunders, Matt Powers, Andrea Maresca, and Amber Swartzell.
[1] Some of these policies are in pending legislation and, therefore, are subject to change.