If you search the term “value-based care” on the internet you will find over 2.5 million hits on that term alone. No one would disagree with the need to provide value to patients and purchasers, but how we define value differs based on where we sit. Value is paying for outcomes, not volume of services. Value is ensuring that patients get the right care at the right time. Value is ensuring that purchasers pay a reasonable cost for the highest possible quality. Value is ensuring that healthcare is provided equitably and sustainably. Implementing value is even trickier than defining it, given the complexity of who pays for care and the challenges of measuring the outcomes we seek to reward.
From the top office of HHS to the back office of a health center and everywhere in between, HMA leaders have been part of our collective journey to value: advancing policy and regulatory change, calculating risk and setting prices, crafting alternative payment models, integrating social services and behavioral health, and coaching industry leaders to make important changes to their business models to adapt to a more sustainable approach to American healthcare. These experiences – both successes and challenges – provide a unique perspective from which to advise clients on transformation of healthcare.
The HMA 2023 fall conference, scheduled for October 30-31, 2023, has thoughtfully curated several discussions to educate, enlighten and motivate attendees on industry standards and navigating the practicality of providing value in care, coverage, and patient experience in publicly funded healthcare:
Leading the Charge on Value, Equity and Growth: The Future of Publicly Sponsored Healthcare: Discuss how these public programs came to be the industry standard bearers and what this shift means for outcomes, affordability, policy, and the overall direction of U.S. healthcare.
Positive Change and the Growing Importance of Managed Care in Publicly Sponsored Healthcare: Discuss the future of publicly sponsored healthcare, outline promising initiatives aimed at improving coverage and care, and address key concerns over funding, policy, equity, and coordination between government, plans, providers, and members.
The Future of Delivery Systems: Achieving Operational and Financial Sustainability: Discuss a wide range of practical approaches to prepare for the future, including managing cash flow, optimizing the workforce, developing long-term reimbursement plans, improving operational efficiency, and addressing changes in government policy.
Real Talk from the Trenches of Value-based Payments: Learn about the advantages and pitfalls of value-based payments, with important insights from organizations that have made it work.
Navigating Change in Medicare Advantage: A Roadmap for Success: Discuss what Medicare Advantage plans must do to meet the demanding, new requirements – all against a backdrop of continued efforts to improve equity, access, outcomes, and cost.
In addition, a pre-conference workshop on behavioral health will be held the afternoon of October 29th, prior to the official start of the conference. This workshop will highlight the integral role of behavioral healthcare in improving patient outcomes across the continuum of publicly sponsored healthcare programs.
We are excited to engage with industry experts throughout these discussions about value-based care and forge a better path forward toward a more sustainable and equitable system of care.
This week, our In Focus section reviews the projected healthcare expenditure and enrollment data from the Centers for Medicare & Medicaid Services (CMS) Office of the Actuary, published June 14, 2023. The Office of the Actuary provides annual updates to historical and projected National Health Expenditure data on Medicare, Medicaid, CHIP, and other public insurance programs, as well as commercial healthcare insurance.
CMS projects that the average annual growth for national healthcare spending from now through 2031 will be 5.4 percent. CMS estimated that the number of insured individuals in the United States was projected to reach a high of 92.3 percent in 2022 and would decrease to 90.5 percent by 2031. CMS projects 93.6 million Medicaid and CHIP members will account for more than $1.2 trillion in annual spending in 2031 and that 76.4 million Medicare beneficiaries will account for more than $1.8 trillion in expenditures that year. A summary of other key takeaways from the actuarial report follows.
Enrollment Projections
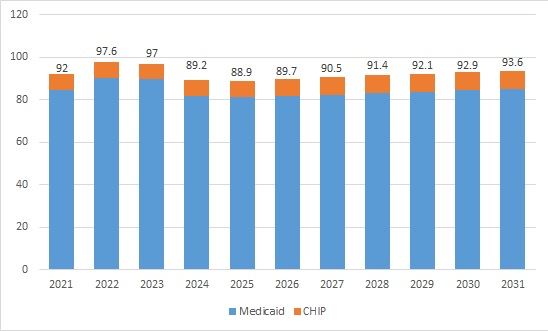
Approximately 92 million people were enrolled in Medicaid and CHIP programs in 2021. Enrollment is projected to have reached a high of 97.6 million in 2022 and is expected to fall between 2023 and 2026 because of Medicaid redeterminations. CMS projects the largest loss in 2024, with 8 million people leaving Medicaid and CHIP that year alone. By 2026, enrollment is projected to hit a low of 89.7 million and start to rise back up in the subsequent years until reaching 93.6 million enrollees in 2031.
Table 1. Historical and Projected Medicaid/CHIP Enrollment (in Millions)
Figure 1. Historical and Projected Medicaid/CHIP Enrollment (in Millions)
Medicare enrollment is projected to continue growing steadily. CMS estimates that Medicare beneficiaries totaled 63.6 million in 2022. By 2031, Medicare enrollment is expected to climb to 76.4 million.
Expenditure Projections
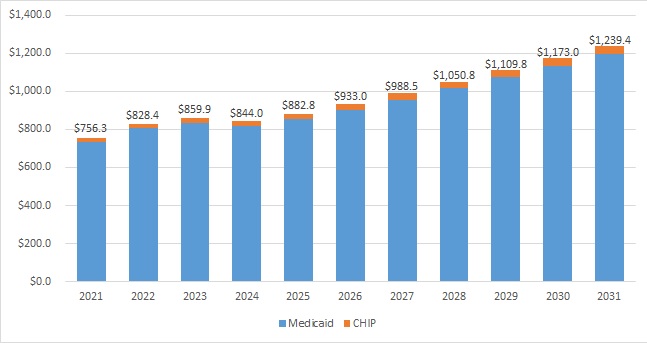
Medicaid expenditures are expected to grow by 5 percent on average in 2022−2031. In 2022, the Medicaid annual growth rate was projected to be −2.1 percent. Following the public health emergency unwinding, average expenditure growth would pick up to 5.6 percent in 2025−2031.
CMS estimated that total Medicaid and CHIP annual spending in 2022 was $828.4 million; by 2031, it is projected to hit $1.2 trillion. For context, private health insurance is projected to reach nearly $2.1 trillion in 2031.
Table 2. Historical and Projected Medicaid/CHIP Expenditures (in Billions)
Figure 2. Historical and Projected Medicaid/CHIP Expenditures (in Billions)
Medicare spending is projected to grow to more than $1.8 trillion in 2031 from $944.2 million in 2022. During this time, average annual expenditure growth is projected to be 7.5 percent. In 2022, spending growth dropped to 4.8 percent compared with 8.4 percent in 2021 because fee-for-service beneficiaries were using fewer emergency department services and as a result of reinstated payment rate cuts associated with the Medicare Sequester Relief Act of 2022.
Medicaid Expenditure Projections by Category
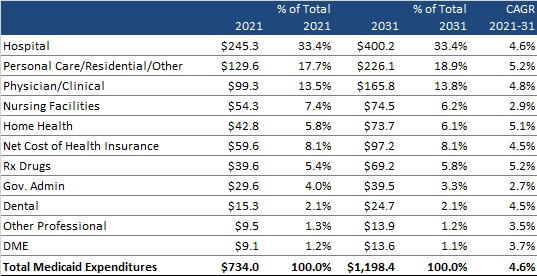
CMS provides a historical and projected breakdown of expenditures by category for Medicaid only (CHIP is bundled with Department of Defense and other public spending). Table 3 summarizes the projected change in annual expenditures for several categories of services and other expenditures. It also shows each category’s percentage contribution to total Medicaid expenditures and the compounded annual growth rate (CAGR) in 2021−2031 for each category of spending. Hospital spending, personal care/residential/other, and physician/clinical expenditures are projected to continue to be the largest contributors to overall Medicaid expenditures, together equaling approximately 65 percent of total expenditures in 2021 and a projected 66 percent in 2031.
Table 3. Historical and Projected Medicaid-Only Expenditures by Category, 2021-2031 (in Billions)
Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth
Pre-Conference Workshop: October 29, 2023 Conference: October 30−31, 2023 Location: Fairmont Chicago, Millennium Park
Health Management Associates has announced the preliminary lineup of speakers for its sixth annual conference, Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth.
Hundreds of executives from health plans, providers, state and federal government, investment firms, and community-based organizations will convene to enjoy top-notch content, make new connections, and garner fresh ideas and best practices.
A pre-conference workshop, Behavioral Health at the Intersection of General Health and Human Services, will take place Sunday, October 29.
Confirmed speakers to date include (in alphabetical order):
Jacey Cooper, State Medicaid Director, Chief Deputy Director, California Department of Health Care Services
Kelly Cunningham, Administrator, Division of Medical Programs, Illinois Department of Healthcare and Family Services
Karen Dale, Chief Diversity, Equity, and Inclusion Officer, AmeriHealth Caritas
Peter Lee, Health Care Policy Catalyst and former Executive Director, Covered California
John Lovelace, President, Government Programs, Individual Advantage, UPMC Health Plan
Julie Morita, MD, Executive Vice President, Robert Wood Johnson Foundation
Anne Rote, President, Medicaid, Health Care Service Corp.
Drew Snyder, Executive Director, Mississippi Division of Medicaid
Tim Spilker, CEO, UnitedHealthcare Community & State
Stacie Weeks, Administrator/Medicaid Director, Division of Health Care Financing and Policy, Nevada Department of Health and Human Services
Lisa Wright, President and CEO, Community Health Choice
Publicly sponsored programs like Medicare, Medicaid, and the Marketplaces are leading the charge in driving value, equity, and growth in the U.S. healthcare system. This year’s event will highlight the innovations, initiatives, emerging models, and growth strategies designed to drive improved patient outcomes, increased affordability, and expanded access.
Early bird registration ends July 31. Group rates, government discounts, and sponsorships are available.
HMA is pleased to welcome new experts to our family of companies in April 2023. This diverse team brings significant expertise in Medicare, Medicaid, regulatory strategies, and managed care, strengthening HMA’s capabilities in healthcare consulting across areas like actuarial support, regulatory compliance, and strategic leadership in Medicare Advantage and Medicaid programs.
This is part of an ongoing series highlighting efforts in Human Services and Family Wellbeing.
During the month of May, National Foster Care Month provides an opportunity to raise awareness on issues related to foster care and to celebrate those who are dedicated to serving our children, youth, and families. Yet it is important to note that unfortunately issues surrounding children and youth experiencing foster care are not limited to one month a year. As noted in our recent child well-being blog, Child welfare services face challenges every day to prevent, treat, and reduce risk of maltreatment, neglect, trauma, housing instability, and violence in communities. All these issues contribute to the significant number of children and youth who enter or remain in the foster care system. These issues are year-round and decades in the making. They need to be seen as a priority for public health and community wellbeing and not just the jurisdiction and responsibility of child welfare agencies.
To positively impact the number of children and youth experiencing foster care, there are some strategies that can be implemented now to promote change:
We must meaningfully elevate the voices of those with lived experience to help us design systems that meet their needs. For foster care, working to hear and understand the voices of youth based on how they have experienced foster care will help create opportunities to improve the system from those most impacted. Further, the meaningful elevation of these voices helps to ensure their input is not contributing towards tokenism and re-traumatization.
Multi-system involvement is important. We can work together to enhance access, increase prevention-oriented services, improve community health, and well-being, and achieve better outcomes using an equity lens, but proposed system reforms cannot be successful without shared ownership within the community and across government agencies. This requires building a responsive and integrated system of care approach to allow communities to seek solutions with the necessary support of the highest leadership within their organizations.
Continue to find ways to assure that mandated reporters and staff who work within child welfare understand that poverty is not neglect, and poverty alone should not be a reason children and youth are removed from their home(s).
System redesign is needed. From front end reporting and assessment, to working with court systems, to building up networks of caring service providers, each component of the current child welfare system and human services partners can strive to find areas needing improvement and collectively change the experiences for children and youth engaged in the child welfare system.
Focus on mental health. This year’s theme from the Children’s Bureau for national foster care month is “Strengthening Minds, Uplifting Families” and is dedicated to supporting children and youth mental and behavioral health as the largest unmet need related to foster care. According to the Children’s Bureau, Up to 80 percent of children experiencing foster care have significant mental health issues, compared with approximately 18 to 22 percent of the general population.[1]
HMA can help public sector and community partners align themselves to improve and develop new delivery systems that will work to address inequalities and disparities as communities strive to meet the needs of children, youth and families impacted by issues like mental health and substance use disorder, domestic violence, child abuse and neglect, food insecurity, housing instability, incarceration and other traumas that impact them greatly.
HMA can help support foster care prevention or reunification program efforts in the following ways:
Creating additional human service system integration of prevention services to help support families and youth experiencing child welfare interventions or foster care.
Increasing Medicaid providers who offer more Evidenced Based and Informed Practices (EBP) among Community Based Organizations (CBO), Providers, and Local Government.
Supporting Managed Care Organizations to develop programs specifically designed to support the wellbeing of children and youth in the foster care system and their families.
Connecting the Family First Prevention Services Act (FFPSA) & Medicaid funding together to ensure that funding supports the need and enhance service implementation.
Working to implement School Based Mental Health programs in communities. We can help convene stakeholders, create process flows, and support the development of sustainable funding for such programs.
Increasing the meaningful use of youth voice for true collaboration in system redesign.
Enhancing judicial engagement with the child welfare system in a way that supports meaningful youth and family voice and representation in court while maintaining the child welfare system’s responsibilities around assuring child safety. Making the court process less traumatic for children and youth and more part of a solution for them will support better outcomes.
Recognizing longstanding racial inequities in foster care experiences that can and should be addressed holistically in communities and supporting efforts to understand the root causes for the disparities in foster care placement.
The public health workforce is in the midst of a crisis, dealing with staff shortages, accelerated retirements and unfilled positions.
The current climate was exacerbated by Covid-19, but many challenges began long before 2020’s pandemic. The public health system underwent a significant contraction following the Great Recession in 2008-2009, losing more than 40,000 positions in state and local governments across the country. While some of those positions were regained with Covid-19 funds during the pandemic, recruitment, diversity and retention remain as challenges, especially for hard to fill positions in nursing and epidemiology. Public health staff report high rates of burnout due to the Covid-19 response and the political climate that resulted, including suffering symptoms of post-traumatic stress disorder. It is likely that there will be staff shortages for the foreseeable future, increased retirements, and departures to other parts of the healthcare industry competing for skills with higher compensation.
New Funding Streams Available
State and local health departments have been receiving significant amounts of one-time money, including the Centers for Disease Control and Prevention (CDC) recent allocation of $3.5 billion specifically for governmental public health efforts.
Health Resources and Services Administration (HRSA) has created a new workforce research center for public health. The AmeriCorps program has developed a specific public health component. These new initiatives were designed to build and support the workforce in governmental public health. As state and local health departments receive or apply for these various sources of workforce development funding, HMA can provide existing technical assistance and training to minimize inefficiencies and duplication of efforts that might be created by a fragmented approach across state and local units of government developing independent approaches to the utilization of WFD funds.
HMA Workforce Expertise
The public health group at Health Management Associates (HMA) is made up of more than 100 colleagues with expertise in public or population health improvement, experienced working with national, state or local organizations seeking to improve public health outcomes. If your organization is looking to improve your public health workforce efforts, it is important to utilize expertise and consolidate efforts across the country so each unit of government is not “reinventing the wheel.” HMA can help multiple organizations in developing plans and coordinating processes for recruiting, training and development of the public health workforce.
HMA understands the skills that are needed to achieve high-performing public health and accountable care. Our expertise developing workforce within safety net delivery systems and accountable care organizations involve transferrable skills for the current challenges in building and developing the public health workforce. We have expertise in recruiting and are creating new training and retraining methods to meet the needs of public health teams, accountable care organizations, graduate medical education, nursing education, learning collaboratives, online training and team simulation training. We understand the care coordination, care management and IT support systems needed to backstop the workforce and meet quality and equity goals.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
The Biden administration has announced that the COVID-19 pandemic Public Health Emergency (PHE) declaration will expire on May 11, 2023. The end of the declaration and other changes in federal policy have significant implications for state Medicaid programs, including the end of a 6.2% increase in the regular federal medical assistance program (FMAP) matching rate for states and continuous enrollment requirements put into place early in the pandemic. This means that an estimated 4-14 million Americans, especially including women and children, will need to engage in state processes for re-certification to continue their Medicaid benefits and states will lose their enhanced matching.
While state have been planning for these changes, collectively referred to as “PHE Unwinding,” the public health implications of these shifts have received little attention. As millions of Americans lose Medicaid benefits, as a result of “PHE Unwinding,” public health departments nationwide are likely to face additional demands and pressures that are also critically important for states to consider. State public health agencies that have spent the last several years responding to the COVID-19 pandemic are now entering a new phase. During the CMS-recommended 12-month period that states have to complete their redeterminations, public health agencies may see increasing numbers of individuals who were previously eligible for Medicaid and other safety net services seeking access to public health programs. Public health officials also may be called on to address the community health impacts of the newly uninsured or those who have lost other benefits, such as enhanced Supplemental Nutrition Assistance Program (SNAP) dollars for food. Addressing challenges may require significant attention of Community Health Workers or other workforces engaged across public health and healthcare and take precedence over other public health priorities. All of this will be happening at a time when public health officials are being called on to re-imagine their infrastructure needs, including reconfiguring and modernizing their data systems.
Public health agencies planning for this immediate future may benefit by taking a systems approach to PHE unwinding and considering a few key variables in their planning—
1.The end of the PHE may rapidly increase demand for public health safety net programs.
Medicaid provides coverage for the sickest and most vulnerable. As redetermination processes leave some without insurance and other benefit programs like SNAP return to pre-pandemic coverage, historically marginalized and medically at-risk populations will be disproportionately impacted. This may result in increased demand for safety net programs usually found in public health departments that serve the under and uninsured, such as the Breast and Cervical Cancer Prevention Program (BCCP) that provides cancer screening for women, and Vaccines for Children (VFC) which provides required immunizations to school-age children who otherwise lack access. Programs such as the Women, Infants and Children (WIC) and perinatal home visiting programs that serve families with limited economic resources may also see increased numbers of eligible families. Health departments can quantify these increases by assessing their populations, estimating increases, and using their existing data to determine which communities and geographic areas are likely to exhibit the greatest needs, and then share this information with policymakers.
2.Unwinding may represent an opportunity to educate legislators and policymakers on the connection between Medicaid utilization and public health programs.
As states see decreases in federal matching for their Medicaid programs, policymakers will look for opportunities to fill gaps in the state share of operating these programs. Public health programs, which are usually run with a combination of state dollars and federal grants, are often looked at as potential sources to fill gaps in Medicaid program costs. Moreover, public health officials may be able to move upstream of these discussions by ensuring that states are maximizing the federal Medicaid match (FMAP) on any public health services that can be billed to Medicaid, including using waivers and state plan amendments to cover services such as maternal home visiting or tobacco cessation under Medicaid, thus stretching grant and state dollars further while covering more individuals. While public health has long discussed the benefits of calculating and sharing the long-term return on investment of public health services, officials may also wish to consider utilizing risk stratification strategies to identify short-term cost savings and cost avoidance to other state programs of the services offered by public health departments. At the local level, health departments are often closely involved in the delivery of services that keep children in school, adults at work, and protect people in hospitals and nursing homes from health care acquired infections. All of these services have immediate benefits to state and local economies.
3. New funding for public health infrastructure, data modernization, and workforce development represents an opportunity to drive collaboration between public health, Medicaid, and other sectors.
As a part of the American Rescue Plan, state public health agencies have received funding from CDC to strengthen their infrastructure to ensure that communities have the people, services, and systems to promote and protect public health. The grants are intended to allow states to focus on increasing the size and diversity of the public health workforce; modernize data systems; and ensure states can demonstrate the foundational capabilities of public health. CDC has affirmed its expectation that states will prioritize collaboration and organizational partnerships as part of these efforts. As state public health agencies use these federal investments to impact programs that reach priority populations and improve health outcomes, several opportunities to reach disadvantaged populations and improve their health outcomes become apparent. For example, public health agencies working collaboratively with state departments of education could lead to partnerships around school-based clinics or workforce training programs, while engaging with the private healthcare and laboratory sectors on data and disease surveillance seems promising. Health departments should start now to in preparation for the flurry of activity that will be sparked in the wake of the PHE. This might involve reaching out to potential partners or organizing town-hall-style” active listening sessions with citizens to meet people where they are and better understand the needs of the community they serve.
HMA and HMA companies will continue to analyze the public health implications of the Medicaid Unwinding and the end of the PHE. We have the depth and breadth of expertise to assist with capacity building, data collection and management, and population health analysis.
HMA can support your agency before or after the end of the PHE.
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
What does your organization need to know?
March 31st marked the end of the COVID-19 Medicaid continuous coverage condition. Most forecasts project between 10-15 million enrollees will lose Medicaid coverage. State Medicaid programs will lose supplemental funding provided for the continuous coverage requirement and begin to transition to normal eligibility operations. Health Management Associates (HMA) and HMA companies can help the full spectrum of stakeholders plan for, adjust to, and administer the changes up to and beyond the 12-month continuous coverage “unwinding” period. The immediate work can serve as a springboard for future improvement initiatives and to respond to federal guidance that is under development to strengthen and streamline eligibility and enrollment processes and improve the experience for consumers.
Who is affected by this change?
Payers including Medicaid managed care organizations and Qualified Health Plans
Provider organizations
Trade associations of Medicaid managed care or provider organizations
State and local community-based organizations
State and local governments responsible for administering and overseeing the eligibility processes for Medicaid and other public programs
Advocacy groups
Foundations
Vendors supporting state agencies, health plans and providers
Watch a video presentation about the HMA Coverage Model
What is in the HMA model?
HMA has developed an insurance mix model that projects how the resumption of Medicaid eligibility redeterminations beginning in April 2023 will affect Medicaid enrollment, employer sponsored insurance (ESI), Marketplace coverage, and the uninsured. The model includes enrollment projections for all 50 states and considers the enhanced Marketplace subsidies included in the Inflation Reduction Act (IRA). Approximately 20 million individuals gained coverage during the redetermination freeze and well over 10 million of the approximately 90 million current Medicaid enrollees are at risk for disenrollment. HMA’s model contemplates the variety in state approaches to managing the resumption of eligibility redeterminations as well as key insights related to the differential impact by Medicaid eligibility categories.
HMA can help with immediate needs to help you plan:
HMA has detailed state-specific unwinding policy insights for each state including observations regarding which states are taking more aggressive and less aggressive approaches.
We can provide technical assistance and strategic planning services to help states and organizations manage the necessary changes.
Actuarial experts can assist with acuity changes caused by the change in enrollment.
Our colleagues are available for a discussion of the product and the key policies influencing the projections.
HMA can also help with post PHE support.
For more information, please contact our experts below.
This week, our In Focus reviews a new Health Management Associates (HMA) report, highlighting hybrid (in-person & virtual visits) as the future of child welfare service delivery. During the COVID-19 public health emergency (PHE), the federal government waived the requirement for “once every 30 days” in-person visits by caseworkers for children in foster care, allowing these visits to occur virtually. In 2021, Casey Family Programs (CFP) commissioned HMA to evaluate the delivery of virtual child welfare services and outline the implications of the COVID-19 PHE on the child welfare system.
The report “Evaluating the Delivery of Virtual Child Welfare Services” is now available. It summarizes HMA’s findings and elevates the voices of staff in public and private child welfare agencies, and of youth and families with lived experiences, and examines their perspectives on how well virtual services have worked. It also details the implications of the COVID-19 PHE, the response from public child welfare agencies, and offers guidance on a hybrid (part in-person, part virtual) service model, which we believe will continue to be a factor in the future delivery of child welfare services.
As the COVID-19 PHE accelerated the spread and scale of telehealth adoption in health care, we surmised that the experience offered valuable opportunities to learn more about how the health care sector’s adoption of telehealth services could be applied in the child welfare community. While cognizant of the unique considerations for child welfare, this disruption also represents a substantial opportunity to rethink the child welfare system and advance both the use of technology as well as a more prevention- and strengths-based approach to child welfare.
The report highlights innovative approaches in the field, offers questions to frame a jurisdiction’s decision-making process, and provides a tool to facilitate an informed decision on the hybrid model. The report also offers a broader value proposition that outlines policy, practice, workforce, and technology imperatives to develop a hybrid approach to the delivery of child welfare services.
This week our In Focus section reviews President Joseph R. Biden’s 2023 State of the Union Address (SOTU) to Congress. The President highlighted specific actions that Congress, and the Administration have taken over the last two years to advance his health care priorities.
During his first SOTU address in 2022, President Biden announced the creation of a “Unity Agenda”, which included priority policy areas with potential for bi-partisan support. The President highlighted several steps the Administration has taken to advance the “Unity Agenda” including:
The bipartisan effort to enact the Mainstreaming Addiction Treatment (MAT) Act, which removed the federal requirement for practitioners to have a waiver (known as the X-waiver) to prescribe medications, like buprenorphine, for the treatment of opioid use disorder
The Cancer Moonshot announcements for almost 30 new programs, policies, and resources to close the screening gap, tackle environmental exposure, decrease preventable cancers, advance cutting-edge research, support patients and caregivers, and more.
Addressing mental health needs through the expansion of Certified Community Behavioral Health Clinics and launch of the 988-suicide prevention hotline.
In his SOTU and accompanying White House materials, the President also proposed new policies and initiatives to further advance his health care agenda. These actions include a combination of issues that would require Congressional approval as well as actions regulatory agencies can already advance. Congress and the Administration are expected to build on previous bipartisan achievements to tackle the nation’s dual crises with addiction and mental health.
Notably, the policies outlined in the SOTU foreshadow an active regulatory agenda over the next 18 months as the Administration seeks to solidify key aspects of the President’s health care agenda ahead of the next Presidential election.
The Administration’s planned actions include the following:
Opioids
Calling on Congress to pass legislation to permanently schedule all illicitly produced fentanyl-related substances into Schedule I.
SAMHSA will provide enhanced technical assistance to states who have existing State Opioid Response funds, and will host peer learning forums, national policy academies, and convenings with organizations distributing naloxone beginning this spring.
By this summer, the Federal Bureau of Prisons will ensure that each of their 122 facilities are equipped and trained to provide in-house medication-assisted treatment (MAT).
This spring CMS will provide guidance to states on the use of federal Medicaid funding to provide health care services—including treatment for people with substance use disorder—to individuals in state and local jails and prisons prior to their release. California is the first state to receive approval for a similar initiative.
Mental Health
CDC plans to launch a new campaign to provide a hub of mental health and resiliency resources to health care organizations in better supporting their workforce.
The Department of Education (ED) will announce more than $280 million in grants to increase the number of mental health care professionals in high-need districts and strengthen the school-based mental health profession pipeline.
HHS and ED will issue guidance and propose a rule to make it easier for schools to provide health care to students and more easily bill Medicaid for these services.
The Administration is scheduled to propose new mental health parity rules this spring.
HHS will improve the capacity of the 988 Lifeline by investing in an expansion of the crisis care workforce; scaling mobile crisis intervention services; and developing additional guidance on best practices in crisis response.
HHS also plans to promote interstate license reciprocity for delivery of mental health services across state lines.
HHS intends to increase funding to recruit future mental health professionals from Historically Black Colleges and Universities and to expand the Minority Fellowship Program.
The Department of Veterans Affairs (VA), working with HHS and Defense, will launch a program for states, territories, Tribes and Tribal organizations to develop and implement proposals to reduce suicides in the military and among veterans.
VA will also increase the number of peer specialists working across VA medical centers to meet mental health needs
Cancer Moonshot
The President called on Congress to reauthorize the National Cancer Act to overhaul cancer research and to extend the funding for biomedical research established in the 21st Century Cures Act.
The Administration will take steps to ensure that patient navigation services are covered by insurance. This could require legislation depending on which type on insurance an individual has.
Health care costs
Urging Congress to pass legislation to cap insulin prices in all health care markets. Expanding the $35 insulin cap to commercial markets will require the 60 votes in the Senate.
Home and community services
Working with Congress to approve legislation to ensure seniors and people with disabilities can access home care services and to provide support to caregivers.
HMA and HMA companies are closely monitoring these federal policy developments. We can assist healthcare stakeholders in responding to the immediate opportunities and challenges that arise and contextualize these actions for longer-term strategic business and operational decisions.
If you have questions about these or other federal policy issues and how they will impact your organization, please contact our experts below.