Join us on Monday, March 6, 2023, at the Fairmont Chicago, Millennium Park, for “Healthcare Quality Conference: A Deep Dive on What’s Next for Providers, Payers, and Policymakers,” where Lee Fleisher, MD, chief medical officer and director of CMS’ Center for Clinical Standards and Quality, will deliver the keynote titled A Vision for Healthcare Quality: How Policy Can Drive Improved Outcomes.
HMA’s first annual quality conference will provide organizations the opportunity to “Focus on Quality to Improve Patients’ Lives.” Attendees will hear from industry leaders and policy makers about evolving health care quality initiatives and participate in substantive workshops where they will learn about and discuss solutions that are using quality frameworks to create a more equitable health system.
In addition to Fleisher, featured speakers will executives from ANCOR, CareOregon, Commonwealth Care Alliance, Council on Quality and Leadership, Intermountain Healthcare, NCQA, Reema Health, Kaiser Permanente, United Hospital Fund, and others.
Working sessions will provide expert-led discussions about how quality is driving federal and state policy, behavioral health integration, approaches to improving equity and measuring the social determinants of health, integration of disability support services, stronger Medicaid core measures, strategies for Medicare Star Ratings, value-based payments, and digital measures and measurement tools. Speakers will provide case studies and innovative approaches to ensuring quality efforts result in lasting improvements in health outcomes.
“What’s different about this conference is that participants will engage in working sessions that provide healthcare executives tools and models for directly impacting quality at their organizations,” said Carl Mercurio, Principal and Publisher, HMA Information Services.
View the Full Agenda
Early Bird registration ends January 30. Visit the conference website for complete details. Group rates and sponsorships are available.
As respiratory syncytial virus (RSV), a seasonal pathogen in young children is challenging the national health care system as part of an unprecedented “tripledemic” with COVID-19 and flu this winter, HMA authors weigh in on potential coverage pathways for new monoclonal antibody (mAb) preventive therapies for RSV and their implications for access.
The Vaccines for Children (VFC) program is a proven vehicle for ensuring comprehensive coverage of immunizations based on recommendations from the Advisory Committee on Immunization Practices (ACIP). An ACIP workgroup is actively discussing potential recommendations for immunization with RSV mAbs.
In the recent Health Affairs Forefront article, “Coverage By Vaccines For Children Program Is Critical For RSV Therapy Access,” HMA authors Helen DuPlessis, MD, FAAP, Diana Rodin, and Matt Wimmer explore the implications of ACIP recommendations, Medicaid coverage pathways, and children’s access to the new therapies.
This week, our In Focus section reviews changes to Medicaid’s COVID-19 Public Health Emergency (PHE) unwinding. People enrolled in the Medicaid program have been continuously enrolled for almost three years, but that situation is about to change. In December 2022, Congress passed, and the President signed into law a massive compromise bill to fund the government. It includes an important change to Medicaid’s continuous enrollment policy, which has been in effect since the early days of the COVID-19 PHE in March 2020.
Congress passed the Families First Coronavirus Relief Act (FFCRA) in March 2020. This legislation has allowed states to receive a 6.2 percentage point increase in their federal matching rate for Medicaid. As a condition for receiving the enhanced funding, states have been prohibited from disenrolling individuals who were otherwise determined ineligible for Medicaid. As a result, nearly 20 million more people are now enrolled in the Medicaid program.
The 2023 spending bill severs the link between the COVID-19 PHE declaration, the continuous enrollment requirement, and the higher federal match rate. The new law:
Ends the Medicaid continuous coverage policy on March 31, 2023, even if the PHE declaration remains in effect. States may begin issuing terminations of ineligible individuals as early as February 1, with an effective date of April 1.
Phases down the 6.2 percentage point increase in the federal matching rate rather than ending it abruptly at the end of the PHE as required under the FFCRA. Specifically, the increase will drop to 5 percentage points in April−June 2023, 2.5 percentage points in July−September 2023, and 1.5 percentage points in October−December 2023.
Does not end the PHE or other flexibilities linked to the PHE.
Congress also added new parameters and reporting requirements for states as they resume annual eligibility renewals with coverage cancellation for individuals who no longer qualify. These requirements are in addition to data the Centers for Medicare & Medicaid Services (CMS) previously directed states to report. For example:
States must maintain up-to-date enrollee contact information for individuals who will undergo an eligibility redetermination.
States cannot disenroll individuals based only on returned mail.
Prior to disenrolling an individual, the state must make a “good faith effort” to contact the person using more than one communication mode.
States must submit to CMS “on a timely basis” a report explaining their eligibility redetermination activities.
States must submit data related to individuals whose eligibility information was transferred between Medicaid and the Marketplace, with some exceptions for states that have integrated Medicaid and Marketplace eligibility systems and those that use the Federally Facilitated Marketplace.
Beyond the “Delinking”
The new law includes other important eligibility-related policies that may affect state and stakeholder planning for what is often referred to as the “unwinding” of continuous enrollment. Notably, the state Medicaid and CHIP programs will now be required to provide 12 months of continuous coverage for children. A total of 24 states already have adopted the 12-month continuous eligibility option for all children enrolled in Medicaid. While the new requirement will not take effect until January 1, 2024, additional states could adopt this option as they resume normal eligibility operations.
In addition, the new law makes permanent the option for states to extend Medicaid postpartum coverage to 12 months, up from 60 days. The one-year postpartum coverage option initially was approved in the American Rescue Plan but for a limited period of five years. Making the option permanent provides more certainty for states. Nearly two-thirds of states have already implemented or are planning to implement the 12-month postpartum coverage extension.
What Happens Next?
The definitive end date for the continuous enrollment policy sets in motion certain federal and state actions and the process for unwinding. On January 5, 2023, CMS published its first guidance to states on processes related to the new unwinding date. The agency is developing additional guidance and will use other communication tools to provide states with greater clarity on the new statutory reporting, matching rate, and federal agency expectations and oversight.
State plans: All states must submit unwinding plans to CMS by February 15; however, February 1 is the deadline for states that intend to begin renewals in February. These proposals must provide details regarding unwinding strategies, the timeline for starting enrollee renewals, and the pace of ongoing renewal processes. The specific end date for the continuous enrollment policy is driving more states to review and finalize their initiatives and engage with stakeholders.
Impact on health plans and providers: The unwinding process will create important decision points and considerations for Medicaid health plans and providers that have members and patients whom the unwinding process may affect in the next 12-18 months. The law’s requirements reinforce the imperative for states, Medicaid health plans, providers, and other partners to renew efforts to confirm enrollee contact information. The unwinding all will create new considerations for Medicaid health plans with respect to enrollee support, case mix, and rate setting issues.
State budgets and legislation: Many states will kick off their legislative sessions this month. The unwinding process—especially the phase-out of higher federal funding—has important implications for state budgets. State legislatures also may address the new continuous eligibility requirements for children and the permanent option for 12 months of postpartum coverage. As a result, Medicaid will likely remain a top priority during upcoming legislative sessions.
Federal oversight and enforcement: The law’s enhanced reporting provision is intended to provide safeguards to ensure eligible individuals remain enrolled in Medicaid. The reporting also focuses on data related to identifying and directing individuals likely to be eligible for the Marketplace program. Although CMS must publicly report these data, the agency has offered no specific timeline for posting the information. Notably CMS has oversight tools and may impose financial penalties on states that are noncompliant with the unwinding requirements.
Forthcoming federal guidance will confirm the parameters for state unwinding actions, CMS’s plans for oversight of state work, and how these efforts affect current Medicaid enrollees. Medicaid partners should closely monitor state level actions, including announcement of state unwinding plans and opportunities for collaboration. Earlier blogs describe the strategies and actions HMA is working with states and partners to undertake as they prepare for this significant change in Medicaid eligibility policies.
Please contact HMA experts below for more information.
The holiday season is grounded in gratitude. At HMA, we are grateful for successful partnerships that have fueled change to improve lives.
We are proud to be trusted advisors to our clients and partners. Their success is our success. In 2022 our clients and partners made significant strides tackling the biggest healthcare challenges, seizing opportunities for growth and innovation, and shaping the healthcare landscape in a way that improves the health and wellness of individuals and communities.
HMA partnered with the Colorado Department of Human Services to support the planning and implementation of a new Behavioral Health Administration (BHA). HMA provided technical research and extensive stakeholder engagement, drafted models for forming and implementing the BHA, employed an extensive change management approach, and created a detailed implementation plan with ongoing support. Today the BHA is a cabinet member-led agency that collaborates across agencies and sectors to drive a comprehensive and coordinated strategic approach to behavioral health.
Wakely Consulting Group, an HMA Company, was engaged to support the launch of a Medicare Advantage (MA) joint venture partnership between a health plan and a provider system. Wakely was responsible for preparing and certifying MA and Medicare Part D (PD) bids, a highly complex, exacting, and iterative effort. The Wakely team quickly became a trusted advisor and go-to resource for the joint venture decision makers. The joint venture has driven significant market growth over its initial years, fueled by a competitive benefit package determined by the client product team.
In 2021 Indiana Governor Eric Holcomb appointed a 15-member commission to assess Indiana’s public health system and make recommendations for improvements. The Indiana Department of Health (IDOH) engaged HMA to provide extensive project management and support for six workstreams. HMA prepared a draft report summarizing public input as well as research findings and recommendations. The commission’s final report will form the basis of proposed 2023 legislation, including proposals to substantially increase public health service and funding across the state.
In early 2022 HMA and Wakely Consulting Group, an HMA Company, assisted multiple clients with their applications to participate in the new CMS ACO REACH model. The purpose of this model is to improve quality of care for Medicare beneficiaries through better care coordination and increased engagement between providers and patients including those who are underserved. The team tailored their support depending on each client’s needs. The application selection process was highly competitive. Of the 271 applications received, CMS accepted just under 50 percent. Notably, nine out of the 10 organizations HMA and Wakely supported were accepted into the model.
HMA, and subsidiaries The Moran Company and Leavitt Partners, were selected by a large pharmaceutical manufacturer to analyze the current pipeline of innovative therapies, examine reimbursement policies to assess long-term compatibility with the adoption of innovative therapies and novel delivery mechanisms, and make policy recommendations to address any challenges identified through the process. The project equipped the client with a holistic understanding of future potential impacts and actions to address challenges in a detailed pipeline analysis of innovative therapies.
While the current federal COVID-19 Public Health Emergency (PHE) declaration could be in place through the winter months, HMA’s team of experts see many reasons to put the PHE’s Medicaid unwinding planning at the top of your list now.
Without an extension, the PHE declaration will expire on January 11, 2023. U.S. Department of Health and Human Services (HHS) officials pledged to provide 60-days’ notice before ending the PHE. As a result, since HHS did not announce an extension by November 12, we can assume that HHS Secretary Xavier Becerra will extend the PHE beyond January.
However, congressional leaders are again considering proposals that would impact the PHE’s Medicaid policies. Such a change could advance during the lame duck session of Congress. For a variety of reasons, lawmakers could seek a statutory change that would de-link Medicaid’s continuous enrollment requirement, the 6.2 percentage point increase in the federal Medicaid match, and other Medicaid maintenance of effort policies from the PHE declaration. Congress could set a specific date for ending these Medicaid policies. Doing so would provide more certainty for planning for the end of the continuous Medicaid enrollment policy and its downstream implications for health insurance programs.
What can Medicaid agencies, health plans, providers and other stakeholders do now?
The transition from Medicaid’s continuous enrollment requirement to normal eligibility operations involves a myriad of policy decisions and operational changes that will impact enrollees. In turn, the end of Medicaid’s continuous coverage policy will also have great bearing on the business and operational strategies of managed care plans, providers and other stakeholders participating in the Medicaid and Marketplace programs.
HMA’s experts are working with state agencies, health plans, hospitals and health systems, and other stakeholders to identify options and workable solutions to prepare for these major changes. This work touches policy, organizational workstreams, systems, and payment. There are issues specific to Medicaid as well as the intersection with Marketplace, the Supplemental Nutrition Program (SNAP), and other public programs.
Combining our collective on-the-ground experience in states with our federal policy insights, experts from across the HMA family of companies list below themes and immediate actions stakeholders can consider. These action steps are focused on ensuring states, managed care plans, providers and other stakeholders are prepared to immediately respond to the end of the Medicaid continuous enrollment policy and work with individuals to provide information and other support they may need to stay enrolled in a coverage program.
Monitor and prepare for federal activities, particularly during the lame duck session of Congress and into 2023. Healthcare policies are likely to feature prominently in Congress’ lame duck session in November and December. Decoupling the Medicaid continuous enrollment and enhanced Federal Medical Assistance Percentage (FMAP) policies from the PHE is one issue under consideration. Any statutory changes to these policies may also include new requirements for the unwinding process. Stakeholders will want to closely monitor these discussions. If Congress sets a statutory end date for the PHE’s Medicaid eligibility policies, this will provide the certainty needed for states to finalize PHE unwinding action plans with target dates for resuming normal eligibility operations. Notably, this may also drive conversations during states’ 2023 legislative sessions.
Stay informed about state-specific landscapes. With statewide elections largely decided and expectations for a PHE end date sometime in the first part of 2023, now is the time for stakeholders to revisit when and how to engage with state Medicaid and other state agencies to support Medicaid eligibility unwinding plans. Stakeholders will want to solidify strategies and timing for engaging with states as unwinding plans are further solidified and eventually implemented. Stakeholders can also monitor changes to states’ eligibility and enrollment rules – including initiatives designed to simplify eligibility rules, enhance eligibility and enrollment systems, and adjust managed care rate setting policies, among others. Many states are utilizing the temporary federal Medicaid flexibilities to alleviate the significant eligibility unwinding workload. Federal agencies also continue to regularly publish new information for states and stakeholders to consider. Some states are implementing policies designed to improve the transition from Medicaid to Marketplace. Understanding the implications of such policies will help stakeholders anticipate how ending Medicaid’s continuous coverage requirement will directly affect them.
Refresh strategies and messaging for outreach and assistance. While the PHE end date remains in flux, state plans for ending the Medicaid continuous coverage policy are still evolving. States are refining their beneficiary communication plans and may be developing updated guidance for stakeholders. Health plans, providers, and other stakeholders should align their messaging and outreach work accordingly and continue to build partnerships in communities across the state. However, outreach alone will not be enough to reach all Medicaid enrollees. Many will need assistance in understanding and complying with changes that come with the end of the continuous enrollment policy. For example, stakeholder-provided redetermination assistance will be key to minimizing the number of enrollees who lose coverage for failure to complete the redetermination process and state requirements for stakeholder assistance will vary state by state.
Update projected impact of enrollee transitions between Medicaid and Marketplace programs. For states and stakeholders, especially health plans, it is time to update projections about 2023 Medicaid and Marketplace enrollment. This may also require new analysis and strategies to address the changing population acuity and resulting impact on capitation revenue. For healthcare providers, health systems, and other healthcare facilities, the end of the Medicaid continuous enrollment policy is expected to drive significant changes in payer mix, and it could reduce revenue as well as impact qualifications for special payment programs, the 340B program, among others. Understanding these dynamics can help with budgeting and implementation of specific patient outreach and support strategies.
5. Develop strategies to translate experiences from Medicaid to Marketplace. Medicaid agencies, managed care plans, and providers have gained valuable insights about the needs of individuals who have remained continuously enrolled in Medicaid during the COVID-19 PHE. This is particularly true for Medicaid enrollees diagnosed with a mental illness, substance use disorder, or both. Medicaid providers and health plans have gained valuable insight on effective clinical care models, whole person care, partnerships with community-based organizations and reimbursement strategies that can better meet the needs of complex populations. Providers and plans can utilize these experiences to better support the millions of individuals who are expected to become eligible for Marketplace coverage after Medicaid’s continuous enrollment policy ends.
The HMA team continues to monitor the dynamic state and federal policy landscapes, including state planning documents and new federal guidance and informational tools. We have the ability to support stakeholders to prepare for the end of PHE and to support state and communities by modeling projected enrollment and payer mix changes across health coverage categories. Stakeholders should be using this time to address gaps in their plans for PHE unwinding and continue to identify and evaluate new options that may emerge to support beneficiaries in retaining health coverage.
This week, our In Focus section reviews highlights and shares key takeaways from the 22nd annual Medicaid Budget Survey conducted by The Kaiser Family Foundation (KFF) and Health Management Associates (HMA). Survey results were released on October 25, 2022, in two new reports: How the Pandemic Continues to Shape Medicaid Priorities: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2022 and 2023 and Medicaid Enrollment & Spending Growth: FY 2022 & 2023. The report was prepared by Elizabeth Hinton, Madeline Guth, Jada Raphael, Sweta Haldar, and Robin Rudowitz from the Kaiser Family Foundation and by Kathleen Gifford, Aimee Lashbrook, and Matt Wimmer from HMA; and Mike Nardone. The survey was conducted in collaboration with the National Association of Medicaid Directors (NAMD).
This survey reports on policies in place or planned for FY 2022 and FY 2023, including state experiences with policies adopted in response to the COVID-19 pandemic. The conclusions are based on information provided by the nation’s state Medicaid Directors.
Key Report Highlights
In the following sections, we highlight a few of the major findings from the reports. This is a fraction of what is covered in the 50-state survey reports, which include significant detail and findings on policy changes and initiatives related to delivery systems, health equity, benefits, telehealth, provider rates and taxes, and pharmacy. The reports also look at the opportunities, challenges, and priorities facing Medicaid programs.
Medicaid Enrollment and Spending Growth
The COVID-19 pandemic created significant implications for Medicaid. During this time, Medicaid enrollment has reached record highs due to the Families First Coronavirus Response Act (FFCRA), enacted in March 2020, which authorized a 6.2 percentage point increase in the federal match rate, or Federal Medical Assistance Percentage (FMAP), retroactive to January 1, 2020, and until the Public Health Emergency (PHE) ends. The increase was available to states that meet certain “maintenance of eligibility” (MOE) requirements. Since the survey, the PHE was extended to mid-January 2023, somewhat delaying the anticipated effects described in survey.
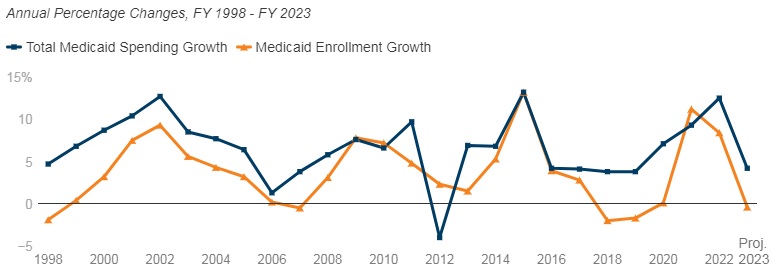
Medicaid enrollment growth slowed to 8.4 percent in FY 2022, after a sharp increase in FY 2021 (11.2 percent). Almost all responding states reported that the MOE continuous enrollment requirement was the most significant factor driving FY 2022 enrollment growth. Responding states expect Medicaid enrollment growth to decline (-0.4 percent) in FY 2023, based largely on the assumption that the PHE and the related MOE requirements would end by mid-FY 2023. States anticipate larger declines as Medicaid redeterminations and renewals resume.
In FY 2022, total Medicaid spending is expected to reach a peak growth of 12.5 percent, with enrollment growth as the primary driver. For FY 2023, total spending growth is expected to slow to 4.2 percent, assuming slower enrollment growth after the unwinding of the PHE. State Medicaid spending grew by 9.9 percent in FY 2022 and is projected to increase by 16.3 percent in FY 2023 once enhanced federal fiscal relief expires. If the PHE is extended, state spending increases and enrollment decreases that states anticipated for FY 2023 could occur later.
Figure 1 – Percent Change in Medicaid Spending and Enrollment, FY 1998-23
SOURCE: FY 2022-2023 spending data and FY 2023 enrollment data are derived from the KFF survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, October 2022. 49 states submitted survey responses by Oct. 2022; state response rates varied across questions. Historic data reflects growth across all 50 states and DC and comes from various sources.
Delivery Systems
Capitated managed care remains the predominant delivery system for Medicaid in most states. Forty-six states operated some form of Medicaid managed care (managed care organizations (MCOs) and/or primary care case management (PCCM)). Forty-one states contracted with risk-based MCOs. Of these, only Colorado and Nevada did not offer MCOs statewide. Only five states – Alaska, Connecticut, Maine, Vermont, and Wyoming – lacked a comprehensive Medicaid managed care model.
Thirty-four states, including Distrct of Columbia, operate MCOs only, five states operate PCCM programs only, and seven states operate both MCOs and a PCCM program.
Twenty-seven states contracted with one or more PHPs to provide Medicaid benefits, including behavioral health care, dental care, vision care, non-emergency medical transportation (NEMT), and long-term services and supports (LTSS).
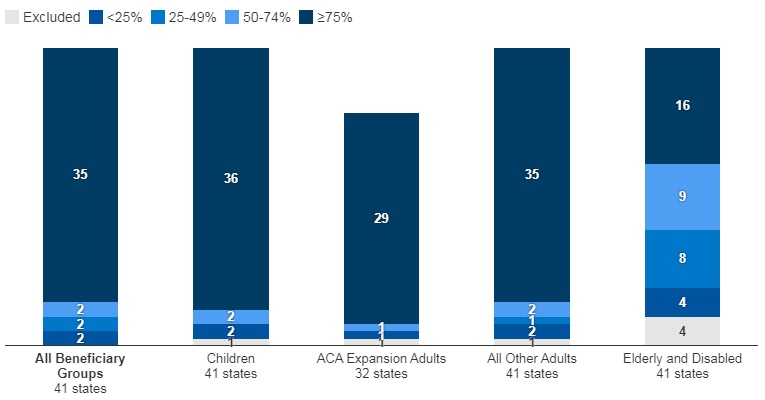
Of the forty-one states that contracted with MCOs, 35 reported that 75 percent or more of their Medicaid beneficiaries were enrolled in MCOs as of July 1, 2022.
Figure 2 – MCO Managed Care Penetration Rates for Select Groups of Medicaid Beneficiaries as of July 1, 2022
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2022.
Medicaid Managed Care and Delivery System Changes
California, Missouri, Nevada, New Jersey, and New York reported expanding mandatory MCO enrollment for targeted populations.
Missouri and Ohio reported introducing specialized managed care programs for children with complex needs.
California, Nevada, and Tennessee indicated that they were carving in certain long-term services and supports (LTSS) into their managed care programs.
California and Ohio reported carving out pharmacy services in FY 2022 or FY 2023, respectively. The District of Columbia carved out emergency medical transportation from its MCO contracts in FY 2022.
Maine, North Carolina, Oregon, and Washington reported changes to their PCCM programs.
Virginia plans to implement Cardinal Care in FY 2023, merging the state’s two existing managed care programs: Medallion 4.0 (serving children, pregnant individuals, and adults) and Commonwealth Coordinated Care Plus (CCC Plus) (serving seniors, children and adults with disabilities, and individuals who require LTSS).
Forty-one states reported at least one specified delivery system and payment reform initiative (e.g. Patient-Centered Medical Home (PCMH), ACA Health Homes, Accountable Care Organization (ACO), Episode of Care Initiatives, All-Payer Claims Database (APCD)).
Health Equity
Twenty-five states reported using at least one specified strategy to improve race, ethnicity, and language (REL) data completeness. Of the 45 responding states, 16 states reported requiring MCOs and other applicable contractors to collect REL data, 12 states reported that eligibility, renewal materials, and/or applications explain how REL data will be used and/or why reporting these data are important, nine states reported linking Medicaid enrollment data with public health department vital records data, and eight states reported partnering with one or more health information exchanges (HIEs) to obtain additional REL data for Medicaid enrollees.
Twelve of 44 responding states reported at least one financial incentive tied to health equity in place in FY 2022. The vast majority of these incentives were in place in managed care arrangements (11 of 13). Within managed care arrangements, states most commonly reported linking or planning to link capitation withholds, pay for performance incentives, and/or state-directed provider payments to health equity-related quality measures. Only two states (Connecticut and Minnesota), reported a FFS financial incentive in FY 2022. Five additional states report plans to implement financial incentives linked to health equity in FY 2023.
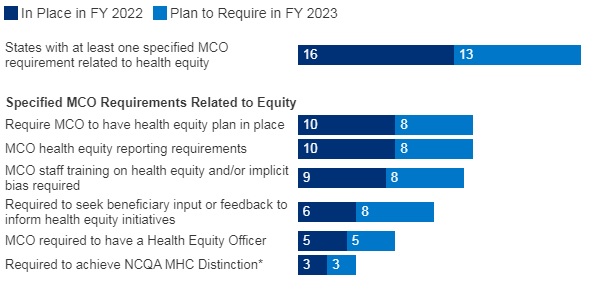
Sixteen of 37 responding MCO states reported at least one specified health equity MCO requirement in place in FY 2022. The number of MCO states with at least one specified health equity MCO requirement in place is expected to grow significantly in FY 2023, from 16 to 25 states. Examples of MCO requirements to address health equity include having a health equity plan, designating a Health Equity Officer, and staff training on health equity and/or implicit bias.
Figure 3 – MCO Requirements to Address Health Equity, FYs 2022-23
SOURCE: KFF survey of Medicaid officials conducted by HMA, October 2022; n=37 states.
Benefits
Thirty-three states reported new or enhanced benefits in FY 2022 and 34 states are adding or enhancing benefits in FY 2023. Two states reported benefit cuts or limitations in FY 2022 and no states reported cuts or limitations in FY 2023.
Figure 4 – Select Categories of Benefit Enhancements or Additions, FYs 2022-23
SOURCE: KFF survey of Medicaid officials conducted by HMA, October 2022; Arkansas and Georgia did not respond.
Behavioral Health Services. States reported service expansions across the behavioral health care continuum, including institutional, intensive, outpatient, home and community-based, and crisis services. States reported addressing SUD outcomes, including coverage of opioid treatment programs, peer supports, and enhanced care management. At least ten states are expanding coverage of crisis services, which aim to connect Medicaid enrollees experiencing behavioral health crises to appropriate community-based care, including mobile crisis response services and crisis stabilization centers.
Pregnancy and Postpartum Services. In April 2022, a temporary option under ARPA to extend Medicaid postpartum coverage from 60 days to 12 months took effect. In addition to the states that took advantage of this eligibility change, some states are enhancing coverage of pregnancy and post-partum services. Nine states (California, District of Columbia, Illinois, Maryland, Michigan, New Mexico, Nevada, Rhode Island, and Virginia) are adding coverage of services provided by doulas and seven states (Alabama, Delaware, Illinois, Maryland, Ohio, Oregon, and Vermont) are investing in the implementation or expansion of home visiting programs.
Preventive Services. Sixteen states reported expansions of preventive care in FY 2022 or FY 2023. For example, seven states are expanding services to prevent and/or manage diabetes, such as continuous glucose monitoring. Other reported preventive benefit enhancements relate to asthma services, vaccinations, and genetic testing and/or counseling.
Services Targeting Social Determinants of Health. Many states reported new and expanded benefits targeting social determinants of health. Twelve states reported new or expanded housing-related supports, as well as other services and programs tailored for individuals experiencing homelessness or at risk of being homeless.
Dental Services. Nine states are adding comprehensive adult dental coverage, while additional states report expanding specific dental services for adults.
Telehealth
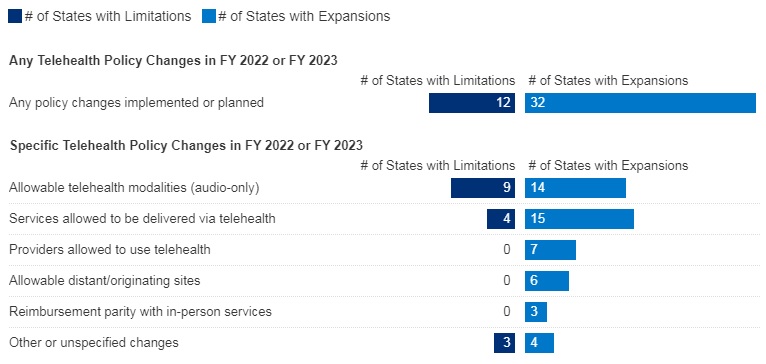
Most states have or plan to adopt permanent Medicaid FFS telehealth expansions that will remain in place even after the pandemic, though some are considering guardrails on such policies. Nearly all responding states that contract MCOs reported that changes to FFS telehealth policies would also apply to MCOs.
Figure 5 – Changes to FFS Medicaid Telehealth Policy, FY 2022 or FY 2023
SOURCE: KFF survey of Medicaid officials conducted by HMA, October 2022; n=48 states.
Nearly all responding states added or expanded audio-only telehealth coverage in Medicaid in response to the COVID-19 pandemic. Twenty-eight states reported that they newly added audio-only coverage while 19 states expanded existing coverage. Nearly all states reported audio-only coverage of mental health and substance use disorder (SUD) services. States least frequently reported audio-only coverage of home and community-based services (HCBS) and dental services. Two states (Mississippi and Wyoming) reported no coverage of audio-only telehealth for the services in question.
Telehealth utilization by Medicaid enrollees has been high during the pandemic but has decreased and/or leveled off more recently. States noted that telehealth utilization trends over time correspond to COVID-19 outbreaks, with higher utilization during COVID-19 surges and lower utilization when case counts are lower. In general, states reported that telehealth utilization was projected to continue at higher levels than before the pandemic, at least for some service categories.
Thirty-seven states (out of 47 responding) reported that behavioral health services were among those with the highest utilization. Additionally, a majority of states reported high utilization of evaluation and management (E/M) services and/or other physician/qualified health care professional office/outpatient services, including primary care.
States reported ACA expansion adults as one of the groups most likely to use telehealth (about one-third of responding states), followed by children and individuals with disabilities (each identified by about one-sixth of responding states).
Concerns regarding services delivered via telehealth included the quality of diagnoses, whether audio-only telehealth may be less effective, and inadequate access.
Key issues that may influence future Medicaid telehealth policy decisions include analysis of data, state legislation and federal guidance, and cost concerns.
Provider Rates and Taxes
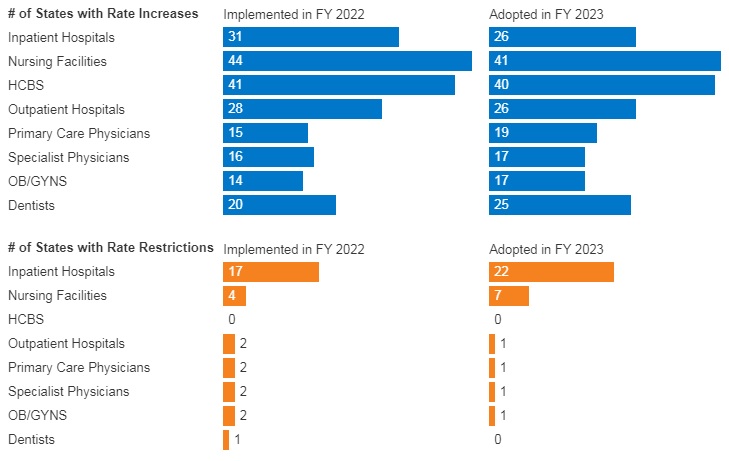
In FY 2022, all 49 responding states reported implementing rate increases for at least one category of provider and 19 states reported implementing rate restrictions. In FY 2023, 48 states reported at least one planned rate increase and the number of states planning to restrict rates increased to 25 states.
States reported rate increases for nursing facilities and home and community-based services (HCBS) providers more often than other provider categories. The survey also found an increased focus on dental rates with about half of reporting states (20 in FY 2022 and 25 in FY 2023) reporting implementing or plans to implement a dental rate increase
Figure 6 – FFS Provider Rate Changes Implemented in FY 2022 and Adopted for FY 2023
SOURCE: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, October 2022.
States continue to rely on provider taxes and fees to fund a portion of the non-federal share of Medicaid costs. All states but Alaska have at least one provider tax or fee in place. Thirty-eight states had three or more provider taxes in place in FY 2022 and eight other states had two provider taxes in place.
The most common Medicaid provider taxes in place in FY 2022 were taxes on nursing facilities (46 states), followed by taxes on hospitals (44 states), intermediate care facilities for individuals with intellectual disabilities (33 states), and MCOs (18 states).
Three states (Alabama, Mississippi, and Wyoming) reported plans to add new ambulance taxes in FY 2023.
Pharmacy
Most states that contract with MCOs report that the pharmacy benefit is carved into managed care (34 out of 41 states that contract with MCOs). Six states (California, Missouri, North Dakota, Tennessee, Wisconsin, and West Virginia) report that pharmacy benefits are carved out of MCO contracts as of July 1, 2022. California was the latest to carve out pharmacy benefits as of January 1, 2022. Two states (New York and Ohio) report plans to carve out pharmacy from MCO contracts in state FY 2023 or later.
In FY 2022, Kentucky began contracting with a single PBM for the managed care population. Louisiana and Mississippi report that they will require MCOs to contract with a single PBM designated by the state in FY 2023 and FY 2024, respectively.
Seven states (Alabama, Arizona, Colorado, Massachusetts, Michigan, Oklahoma, and Washington) have value-based arrangements (VBAs) in place with one or more drug manufacturers.
More than half of responding states reported newly implementing or expanding at least one initiative to contain prescription drug costs in FY 2022 or FY 2023.
Six states (Florida, Kentucky, Massachusetts, Maryland, Nebraska, Nevada) reported recently implemented or planned policies to prohibit spread pricing or require pass through pricing in MCO contracts with PBMs.
Key Opportunities, Challenges, and Priorities in FY 2023 and Beyond
When asked to identify the top challenges for FY 2023 and beyond, Medicaid directors listed the following:
The unwinding of PHE emergency measures and the resumption of redeterminations.
Expiration of emergency authorities.
Lasting focus on COVID-19, including vaccinations, long-COVID, decreased utilization of preventive care services, and future emergency preparedness.
Medicaid directors stated that future priorities shaped by COVID-19 include:
Health equity.
Specific populations and service categories, including behavioral health, long-term services and supports, and maternal and child health.
Health care workforce challenges.
Payment and delivery system initiatives and operations.
IT system modernization.
Social determinants of health.
Medicaid directors note that COVID-19 has presented both new opportunities and challenges and has also shifted and shaped ongoing Medicaid priorities.
This week, our In Focus highlights a Health Management Associates Institute on Addiction (HMA IOA) report, Delaware Substance Use Disorder Treatment System Needs Assessment, published in June 2022. HMA IOA conducted a statewide three-county substance use disorder (SUD) treatment system needs assessment in Delaware. This project began in November 2021 and was primarily funded by New Castle County with contributions from Kent and Sussex counties. The goal was to review the current state of the SUD treatment ecosystem, identify strengths and gaps collecting input from as many Delawareans across multiple sectors as possible, and make actionable recommendations to build a more robust and sustainable future state system.
The final analysis included interviews with key stakeholders, focus groups, a survey of all licensed SUD providers, claims data analysis, and a comparison of Delaware’s public (e.g., Medicaid) outpatient and residential SUD reimbursement rates with selected regional states. This approach provided a unique cross-sector view of where the most significant opportunities for improvement and investment may rest.
The areas of greatest experienced need in the system were reported as: inadequate treatment beds, especially for some populations, like children and youth; lack of residential services for adults, especially those on Medicare and without insurance; needed supports for those experiencing negative impacts from social determinants of health (SDOH), like transportation and housing needs; lack of consistent access and care coordination; lack of adequate reimbursement to sustain the system or expand the treatment system; the need for trauma-informed care (TIC); and the need for more harm reduction and prevention strategies, including greater access specifically to Narcan 4mg Nasal Spray or its generic equivalent.
The study found that Delaware is meeting only 15 percent of SUD treatment needs and only meeting five percent of the need for the highest-intensity services, including inpatient treatment.
The results also showed an apparent discrepancy between what the state is working hard to implement to address the SUD and overdose crisis in Delaware and the community’s perception of, or lived experience with, those SUD treatment services and supports. Additionally, HMA IOA heard about many treatment system strengths from interviewees, town hall participants, and focus groups and included recommendations that are meant to leverage those existing strengths in the future treatment system.
On August 18, 2022, the Centers for Medicare and Medicaid Services (CMS) released a roadmap to support healthcare providers with preparing for the eventual end of the COVID-19 public health emergency (PHE) declaration. CMS also published a series of fact sheets summarizing the status of Medicare Blanket waivers and flexibilities by provider type as well as flexibilities applicable to the Medicaid providers and stakeholders.
In its announcement, CMS expressed concern that the continued PHE flexibilities could contribute to further decline in patient, resident, and client safety beyond what has already been observed. As a result, the agency is cautiously working to balance ongoing PHE needs while conveying more urgency for providers to prepare for the eventual end of the PHE flexibilities and waivers.
CMS has already ended certain flexibilities and waivers. The agency could phase out other flexibilities as it prepares to let the PHE declaration lapse. This means that providers and health plans should act now to assess flexibilities and waivers in use and develop a plan to transition to post-PHE environment.
Phase-out of COVID-19 Flexibilities
During the COVID-19 PHE, CMS has utilized Medicare and Medicaid waivers and flexibilities extensively. For example, Medicare has not enforced certain federal requirements during this time to allow hospitals to utilize off-site locations to screen and treat patients when needed as well as to minimize certain reporting requirements. The agency’s flexibilities also have accelerated adoption of telehealth and audio only services, particularly for behavioral health services.
Medicare and Medicaid providers across the states utilized PHE flexibilities to varying degrees, in part depending on experiences in individual communities, capacity, and other provider specific factors. Additionally, over the course of the PHE health plan and provider staffing and workflows have changed dramatically. This means health plans and providers will need a tailored plan to support the transition to the post PHE environment.
HMA’s experts are working with hospitals, health systems, clinics, and other providers as well as health plans on the steps they need to take now to prepare for multiple transitions. Our experts identified six immediate steps that Medicare and Medicaid plans and providers can be undertaking now to ensure they can effectively return to normal operations, including:
Review performance on the patient and clinician safety metrics cited in the new CMS resources. In instances where providers have gaps and suboptimal safety and quality outcomes they will need assistance developing and implementing mitigation and quality improvement plans.
Utilize CMS’ tailored fact sheets to identify specific flexibilities and waivers in use now and the “normal” federal regulations that will be in effect once the PHE lapses. This assessment should include the blanket waivers and provider specific flexibilities, including:
Flexibilities around the requirements and timing for practitioner training
Expansion of allowable sites of service that permitted more expansive use of telehealth and virtual services as well as screening and treatment provided at alternative sites
Relaxation of federal requirements pertaining to surge capacity protocols
Flexibilities for staffing requirements, including medical records departments, nursing facilities, among others
Waiver of requirement for hospitals to submit occupational mix surveys and to have a utilization review plan with a UR committee focused on services furnished to Medicare and Medicaid enrollees
Applicable of the Extreme and Uncontrollable Circumstances Policy in Medicare’s Shared Savings Program and use of other flexibilities for MSSP Accountable Care Organizations (ACOs)
Non enforcement of certain physician self-referral laws
Waiver of numerous reporting requirements including those pertaining to verbal orders, discharge planning, HEDIS and STARs measure reporting, among others
Project impact of ending Medicaid’s continuous coverage policy and support individuals with actions they may need to take at the end of the PHE. Once the PHE ends, Medicaid’s enhanced federal funding for states and continuous coverage policy will end. HMA is working with health plans, providers and other stakeholders to project how this change will impact the enrollment and payer mix on state and local levels. Additionally, patients and their caregivers will need support from plans, providers, and consumer groups to ensure they renew their coverage or transition to other coverage programs when needed. HMA’s experts have written extensively about our work to support the Medicaid unwinding activities in two blog posts – The PHE is continuing—what’s next for Medicaid? and How stakeholders can prepare now for unwinding of Medicaid public health emergency continuous eligibility.
Develop a plan to transition from “PHE” to “post-PHE” expectations that is informed by the assessment of flexibilities in use. Key components of the plan include:
Anticipated resource needs to reflect changes in staffing and workflows during the PHE
Articulation of specific compliance procedures and regular reporting requirements that will resume and the process for this transition
Develop training and education opportunities for staff that may be new or need refresher on normal policies and procedures as well as timeframes for making these changes
Update budgets projections to account for changes in reimbursement rates for certain services post-PHE. Certain reimbursement amounts and payment methodologies will change post-PHE, such as payment for administering the COVID-19 vaccine in a Medicare patient’s home among other changes. Providers will need to project the financial impact of these payment changes and update coding and billing manuals and procedures where applicable.
Build strategies to sustain changes to care models implemented during the COVID-19 PHE while also addressing health disparities. Some providers and facilities adopted care models and modified existing ones during the PHE that may have improved patient outcomes and experiences, maximized expertise of practitioners, and improved value-based care. For example, some providers have embraced the Medicare Hospital Without Walls Initiative and will need to assess their options as some of those flexibilities are phased out. Other federal opportunities have newly emerged during the pandemic, such as the Rural Emergency Hospital designation and pending changes to the Medicare Shared Savings Program (MSSP).
What’s Next
The COVID-19 PHE declaration next expires on October 12, 2022. While a renewal of the PHE declaration is possible into early 2023, providers should be using this time to prepare for resumption of normal policies and procedures.
The expiration of PHE flexibilities and waivers are not, however, happening in a vacuum. Providers need to make this transition amidst a dynamic healthcare sector with high expectations for continuous improvement in quality, patient experiences, and value. During this transitional period HMA’s experts are working with health plans and providers to develop or revisit strategic plans and investments to refocus attention on improving models of care and value-based payment approaches, including strategies that will help mitigate health disparities.
As the urgent needs of COVID-19 Public Health Emergency (PHE) continue to subside, state Medicaid agencies are exploring pathways and concepts to further address the historic inequities and health disparities laid bare by the pandemic. These efforts are closely aligned with the current Administration’s policy objectives for the Medicaid program, specifically:
Addressing health equity
Improving access and coverage
Promoting whole person care
For several decades, Medicaid Section 1115 demonstration programs have provided a powerful lever for federal and state policymakers to design, implement, and evaluate transformative initiatives. All states administer at least one Section 1115 demonstration program. Some demonstrations are narrowly tailored to address services or populations while others capture broader features pertaining to coverage, benefits, and payment and delivery system innovations.
Notably, a new wave of comprehensive and transformative Medicaid Section 1115 demonstration proposals is emerging.
Working closely with the Centers for Medicare and Medicaid Services (CMS), states are developing proposals that place individuals at the center of health care in an entirely new way – by recognizing their medical needs as well as the complexity of circumstances and environmental factors that shape the individual’s medical, physical, and behavioral care needs and outcomes.
Teams of experts from across the HMA family of companies are supporting state agencies, counties, health plans, providers, community and consumer organizations, and other stakeholders with translating federal goals and parameters into concrete proposals as these move through the stages of concept paper, application and negotiation, and implementation. Demonstrations will reflect each state’s unique political and policy landscapes, but the programs will be grounded in certain federal goals and expectations to enhance accountability and improve outcomes.
Our experts identified three trends in state 1115 demonstration programs. In this and subsequent In Focus posts we will share our team’s initial insights and considerations for stakeholders based on our collective “on the ground” expertise. We include illustrative examples from some states with approved and pending Section 1115 proposals.
Section 1115 Trend #1: States are advancing a new vision for Medicaid’s role in addressing health equity, influenced by social drivers and grounded in a community’s needs.
CMS is strongly encouraging states to consider initiatives that address health inequities and community specific social drivers of health. As evidenced by the current state initiatives, Section 1115 demonstration programs will be a primary — but not the only — pathway states utilize to design strategies to address health inequities driven by non-health systems and circumstances. Based on our work with states and stakeholders, it is critical that states ensure the services are directly linked to factors that impact health outcomes for Medicaid enrollees and that they have mechanisms to evaluate the impact of community and social care services.
Several state proposals already signal CMS’ current vision for using Section 1115 authority to test new types of assistance within service categories to include non-medical services, services tailored to populations, and assistance that is linked to desired outcomes. For example:
North Carolina’s Section 1115 pilot program will provide support to certain groups of consumers for an array of community supports ranging from housing related services and transportation access to interpersonal violence and access to food and nutrition services. The program includes help for consumers related to utility set up and moving costs, and support to connect with community services to address legal issues impacting housing and thereby impacting health.
In December 2021, CMS approved California’s Section 1115 demonstration program and linked this to a separate waiver approval allowing the state to further enhance services and accountability within its managed care program. As part of California’s implementation of its statewide whole person care initiative, the state will be able to pay for housing navigation and tenancy services and assistance with first month deposits for certain populations enrolled in its statewide managed care program. This proposal is grounded in the state’s commitment to ensure that the non-medical services were clearly defined and clinically oriented for the intended population.
CMS’ approval of the North Carolina and California programs is paving the way for conversations in other states, including New York, New Jersey, and Oregon among others. Negotiations on similar initiatives to address health equity in other states, include:
New York, like North Carolina, plans to seek CMS’ approval to offer a range of community services that would be provided through newly established networks of community-based organizations in all regions of the state. The state envisions that the CBO networks will include small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. In addition, New York is asking CMS to support a health equity focused proposal which would provide certain “in-reach” services for incarcerated individuals before they are released.
Oregon submitted a request to use federal Medicaid spending authority to address community-based health inequities and to establish statewide health equity investments (HEIs). The state is especially focused on supporting consumers during disruptions in coverage, life transitions, or disruptions caused by climate events. Community-based investments will reflect empirical evidence and community assessments and may include efforts to improve building environments and expand culturally and linguistically. Addressing climate events may be of particular interest as it addresses multiple priorities for Administration.
Conclusion
North Carolina and California offer important insights into what may be possible and as importantly, what may be beyond the bounds of CMS’ Medicaid authority. Chief among the outstanding issues for states and stakeholders is whether additional innovative programs for addressing health disparities among justice-involved populations is possible under Medicaid’s demonstration authority.
CMS may use the experience with initial states to provide more concrete information on these general parameters and expectations. Formal guidance would prove helpful to states and stakeholders seeking to apply new knowledge and experiences with health inequities into practice within the Medicaid programs.
HMA’s interdisciplinary teams of Medicaid, human services, and actuarial experts are assisting states as well as stakeholders as they conceptualize, develop, and implement Section 1115 programs. To learn more about our work and the breadth of our service, contact our expert below.
Be sure to register for HMA’s 2022 Conference by Monday, July 11, to get the special early bird rate of $1,695 per person. After July 11, the rate is $1,895.
Nearly 40 industry speakers, including health plan executives, state Medicaid directors, and providers, are confirmed for HMA’s The New Normal: How Medicaid, Medicare, and Other Publicly Sponsored Programs Are Shaping the Future of Healthcare in a Time of Crisis conference, October 10-11, at the Fairmont Chicago, Millennium Park.
In addition to keynote sessions featuring some of the nation’s top Medicaid and Medicaid executives, attendees can choose from multiple breakout and plenary sessions on behavioral health, dual eligibles, healthcare investing, technology-enabled integrated care, social determinants of health, eligibility redeterminations, staffing, senior care, and more.
There will also be a Pre-Conference Workshop on The Future of Payment Reform: Delivering Value, Managing Risk in Medicare and Medicaid, on Sunday, October 9.

 In December 2021, CMS approved
In December 2021, CMS approved  New York, like North Carolina, plans to seek CMS’ approval to offer a range of community services that would be provided through newly established networks of community-based organizations in all regions of the state. The state envisions that the CBO networks will include small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. In addition, New York is asking CMS to support a health equity focused proposal which would provide certain “in-reach” services for incarcerated individuals before they are released.
New York, like North Carolina, plans to seek CMS’ approval to offer a range of community services that would be provided through newly established networks of community-based organizations in all regions of the state. The state envisions that the CBO networks will include small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. In addition, New York is asking CMS to support a health equity focused proposal which would provide certain “in-reach” services for incarcerated individuals before they are released. Oregon submitted a request to use federal Medicaid spending authority to address community-based health inequities and to establish statewide health equity investments (HEIs). The state is especially focused on supporting consumers during disruptions in coverage, life transitions, or disruptions caused by climate events. Community-based investments will reflect empirical evidence and community assessments and may include efforts to improve building environments and expand culturally and linguistically. Addressing climate events may be of particular interest as it addresses multiple priorities for Administration.
Oregon submitted a request to use federal Medicaid spending authority to address community-based health inequities and to establish statewide health equity investments (HEIs). The state is especially focused on supporting consumers during disruptions in coverage, life transitions, or disruptions caused by climate events. Community-based investments will reflect empirical evidence and community assessments and may include efforts to improve building environments and expand culturally and linguistically. Addressing climate events may be of particular interest as it addresses multiple priorities for Administration.