
October 2, 2024
Shaping the Future: Join Us in Exploring Trends and Insights at the 2024 HMA Conference
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
Shaping the Future: Join Us in Exploring Trends and Insights at the 2024 HMA Conference

This week, our In Focus section from the HMA Weekly Roundup highlights the Illinois Department of Healthcare and Family Services request for proposals (RFP) for a dual-eligible special needs plan (D-SNP) to replace its current Medicare-Medicaid Alignment Initiative (MMAI) demonstration.
Illinois is one of the states affected by the Centers for Medicare & Medicaid Services (CMS) decision to end the capitated model in the federal Financial Alignment Initiative (FAI) demonstration. Illinois is among the last states to issue an RFP that will support the transition from the demonstration program. Two states, Texas and South Carolina, have yet to issue RFPs. On September 10, 2024, CMS issued a memo discussing end-of-demonstration enrollment and operational considerations and deadlines by which states should make operational decisions.
The Health Management Associates, Inc., (HMA) In Focus article June 26, 2024, discussed related changes that CMS finalized to the federal policy framework for D-SNPs to enhance care coordination, improve health outcomes, and ensure that dual-eligible beneficiaries receive accurate information about their healthcare while integrating successful features of the FAI demonstration and the Medicare-Medicaid Plan (MMP) program. These decisions are prompting more states to develop new models for integrating Medicare and Medicaid services.
This Illinois procurement will transition the state to a fully integrated dual-eligible special needs plan (FIDE-SNP) model, which will include a requirement that plans provide managed long-term services and supports (MLTSS) for both people who are dually eligible and Medicaid-only beneficiaries beginning in 2027.
The RFP is largely focused on quality care provisions and improved care coordination across all services lines, including overall expectations to achieve the following:
Overall, the Illinois D-SNP procurement reflects broader national trends toward more coordinated, equitable, and outcome-focused healthcare.
Focus on Health Equity. The procurement emphasizes health equity and reducing disparities, including information on innovations that are responsive to health-related social needs (HRSNs) and social determinants of health (SDOH). The state is weighing payers’ experience partnering with non-traditional providers to meet Medicaid customers’ needs, their innovative programs to address customers who are difficult to locate, and their strategies for improving care for adults with complex needs in facility or community-based settings.
In addition, the state will require plans to report outcomes by race, ethnicity, and geography. Given the demographic and health equity reporting requirements, payers should be prepared to speak to their data collection, member engagement strategies, and relationships with community-based organizations. This capability will be an essential component of addressing both population health and health equity activities.
Alternative Payment Models. The RFP also requests detailed information on the payer’s strategy for increasing the use of APMs in Illinois Medicaid managed care, including the models the payer intends to implement. Experience supported by data-driven outcomes and explanations of work with providers or clinics to adopt, manage, and support reporting and analytics for APMs is a key area of interest for the state. Notably, the state seeks information on plans to include behavioral health providers in APMs.
Long-Term Services Related Transitions. The RFP questions also reflect the long-term services and supports that dually eligible beneficiaries need, as well as those of Medicaid-only beneficiaries who are eligible for these services. More specifically, the RFP raises questions to determine how payers will effectively implement nursing home diversion plans, incentivize hospitals to discharge patients to community settings, and approaches to transition members from institutional settings to the home and community, including by connecting members with supports for HRSNs. Payers will be expected to provide specific examples of their experience and outcomes in other states.
The emphasis on health equity in the Illinois RFP reflects a broader national trend. States are increasingly interested in—and in some situations required—addressing SDOH and reduce disparities, especially for the Medicare and Medicaid dual-eligible population. As a result, payers and other healthcare organizations must develop capacity internally and through external collaborations to build their expertise and evidence base for advancing improvements.
The push for APMs in the Illinois procurement aligns with national efforts to move away from fee-for-service models. Illinois’s inclusion of behavioral health providers in APMs and requiring integrated care models highlights the growing recognition of the importance of mental health in overall health outcomes.
Illinois’s RFP also reflects heightened interest in improving care transitions and coordination. The potential for incentive programs related to community placement and increased focus on nursing home diversion will require innovative plans and a long-term commitment to working with all stakeholders to build on the federal FAI experiences.
Responses to the Illinois RFP are due October 18, 2024, and awards are expected to be announced in December. The state anticipates making awards to the top four bidders. Contract execution is estimated July 2025, with implementation January 1, 2026.
As the FAI demonstration ends and CMS’s integration requirements take effect over the next several years, there will be a steep learning curve for states, payers, and other key stakeholders adapting to this evolving environment. Compliance with new CMS rules will be crucial, and experiences in Illinois and other FAI demonstration states can provide valuable insights for other states and stakeholders.
Additional growth and program refinements in the federal Medicare Advantage (MA) landscape are expected in the coming years, especially among MA D-SNPs. Those MA D-SNPs that have yet to participate in Medicaid will need to continue make significant business decisions on participation and actively compete to secure state Medicaid contracts, which will have downstream implications for their state and local partners.
Health Management Associates (HMA) experts continue to review the evolving landscape and federal changes that will affect D-SNPs in 2025 and beyond. Contact our featured experts below for details about the nationwide D-SNP rules and landscape.
The upcoming HMA event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, offers extensive opportunities to engage with leaders from various sectors who are designing and implementing Medicare-Medicaid integration initiatives. Join us for main stage panel discussions with distinguished health plan executives from national and local plans and Medicaid directors from Iowa, New Mexico, New York, and Rhode Island.
HMA Principal Holly Michaels Fisher will lead a deeper dive into integration issues during the breakout session, Innovations to Improve Outcomes for Medicare-Medicaid Dually Eligible Individuals, with speakers Michael Carson, President and CEO of WellCare; Dr. Steven R. Counsell, Medical Director for the Division of Aging at Indiana Family and Social Services Administration; Dr. Linda Kurian, Executive Medical Director for the Center of Excellence of Medicare Duals/D-SNP at Aetna; and Juliet Marsala, Deputy Secretary for the Office of Long-term Living in the Pennsylvania Department of Human Services.
During the breakout, Meeting New Expectations for Health Equity and Improved Beneficiary Outcomes in Medicare Advantage, HMA Principal Greg Gierer will facilitate a conversation on the evolving landscape of MA rates and supplemental benefits, with experts Melinda Buntin, Health Economist and Bloomberg Distinguished Professor at the Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins Carey Business School; Mark Fendrick, Director of the University of Michigan’s Center for Value-Based Insurance Design, and Matt Kazan, Vice President of Policy and Government Affairs at the SCAN Group.
Online registration ends October 1st.
Countdown to HMA’s Fall 2024 Conference: Spotlight on Medicare-Medicaid Integration

Caprice Knapp, a seasoned health economist with over 20 years of experience in Medicaid and healthcare policy, shares her journey through various roles in government, academia, and private insurance. In this episode, Caprice offers a unique perspective on the challenges of measuring quality in healthcare, the importance of data-driven decision-making, and how global healthcare models can inspire innovation in Medicaid. From pediatric palliative care to cost-effective policy solutions, Caprice sheds light on how improving quality of care can transform healthcare outcomes for vulnerable populations.

Expanding access to medical respite care for individuals who are unhoused or have no stable housing and are too ill to be discharged to the streets but not sick enough to stay in the hospital and require some supports to recover from their illness or injury.
Medical respite, or recuperative care, according to the National Institute of Medical Respite Care (NIMRC) is “an intervention that provides post-acute medical care for individuals experiencing homelessness who are not sick enough to warrant hospitalization, but who are too frail or ill to recover safely in a shelter or on the streets.”
Respite care benefits both providers and patients and saves money. According to a study by NIMRC, respite care results in a 24% reduction in Medicaid cost per enrollee, 30% decrease in hospital admissions, 38% reduction in emergency department visits, and a 92% attendance rate at follow up appointments within 30 days of hospital discharge.
Medical respite is not a housing service. Housing support services like housing stability, shelter, and supportive housing are critical components of the housing support system. Medical respite is the bridge and a safe transition from the medical care system back to the community and other needed services and supports. By providing a safe bed, clean restrooms, nursing assistance, and healthy meals, medical respite services can improve health outcomes and begin a process of addressing other critical health-related social needs, such as stable housing.
HMA offers a full suite of professional health and human services consulting services to organizations across the country. In Minnesota, HMA helped write the legislation that helped Minnesota Medicaid give coverage for respite care and has expertise in creating this model that can be used in other states. Many states lack this benefit and even in Minnesota, where it is now covered, there is a shortage of providers.
Project Spotlight: Minnesota Recuperative Care Benefit
THE TASK:
Legislation was passed requiring Minnesota’s Department of Human Services (DHS) to create a recuperative care benefit through Medicaid. Stakeholder engagement to discuss Medicaid options and to define the benefit. Recuperative Care was not well developed in MN and there were few beds operating in the state.
HOW WE HELPED:
HMA engaged interested individuals as guided by DHS. This included interviewing individuals with lived experience. Our Medicaid and recuperative care SMEs walked everyone through understanding the service and defining the service. In addition, we educated interested parties about the pathways in Medicaid including a state plan amendment and the various waiver options. The group came to consensus with DHS on a state plan amendment. HMA wrote the legislative language and report to support this direction.
THE OUTCOME:
The legislative language was approved. The state plan amendment was submitted and approved by CMS. Recuperative care is now a Medicaid benefit in Minnesota.
HMA can help states, providers, and communities create this benefit, implement effective respite services, and adapt the set of national standards for Medical Respite given your state and community needs including:
Safe and quality accommodations
Environmental services
Care transitions into medical respite from other settings
Access to high quality post-acute clinical care
Care coordination and wrap-around services
Safe care transitions out of medical respite to the community
Quality improvement
HMA can also provide technical assistance, help with alternate payment models, workforce and strategic planning to support respite care.
Contact our experts:



In recognition of National Recovery Month this September, our In Focus section spotlights a new report from Health Management Associates, Inc. (HMA), Substance Use Disorder in California: A Focused Landscape Analysis. Published in August 2024 with support from the California Health Care Foundation, this analysis provides valuable insights into California’s substance use disorder (SUD) treatment system and offers actionable recommendations for improvement that can be applicable for other states.
The SUD Landscape in California
SUDs continue to be a significant issue both nationally and in California. In 2022, approximately 9 percent of Californians ages 12 and older met the criteria for SUD, compared with 16.5 percent nationally in 2021. The prevalence of SUD is also on the rise: in 2015, 8.1 percent of Californians ages 12 and older met SUD criteria, rising to 8.8 percent in 2022. Of the Californians struggling with SUD, only 10 percent received treatment for their condition, compared with 6 percent nationally in 2021. Overall, 81 percent of US adults who received care for SUD reported struggling to access necessary services.
California’s public behavioral health system siloes specialty mental health (MH) services, mild-to-moderate MH services, and SUD treatment services, resulting in a fragmented and inconsistent system that struggles to effectively support people with co-occurring conditions.
County plans administer specialty behavioral health (BH) services. They all have memorandums of understanding with the state’s Department of Health Care Services that are separate from the state arrangements to provide physical healthcare services. BH programs vary significantly across the state because counties operate them differently, with key variations in access policies, quality monitoring, services, and programming. Mild-to-moderate (non-specialty) MH benefits are administered by Medicaid managed care plans. Much of the state’s SUD treatment is operated by the Drug Medi-Cal Organized Delivery System (DMC-ODS).
Barriers to Care: Key Findings
System barriers prevent many Californians with SUD from accessing adequate care. Interviewees received a pre-interview questionnaire to determine the factors they believe have the greatest impact on access to SUD treatment. According to 11 out of 14 respondents, lack of access to housing and residential services is a “huge barrier” to SUD treatment.
Other barriers to care access, ranked in order, include limited access to food, transportation, and other social drivers of health (SDOH), SUD provider shortages, stigma against people with SUD, disparities in service availability across racial/ethnic groups and other populations, and complex referral and intake processes.
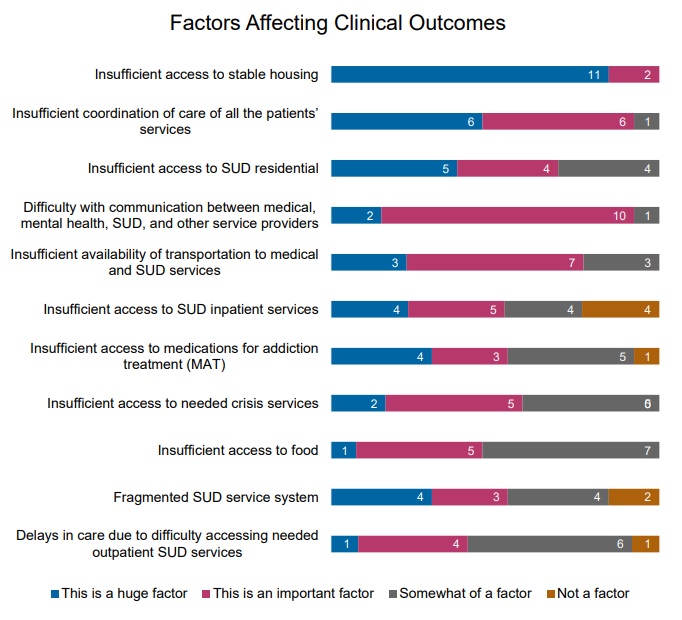
Respondents also identified factors that could negatively affect clinical outcomes for people with SUD. Insufficient access to stable housing ranked first, followed by inadequate care coordination, and limited access to residential SUD treatment. Respondents ranked 11 factors as follows:
Figure 1: Factors Leading to Reduced Outcomes, Ranked from a List of 11
Service gaps pose another significant barrier to people accessing SUD treatment, and some populations are more likely to encounter challenges than others. According to the respondents, by various population groups, Latine/Hispanic populations, African American/Black populations, and Native American/Alaska Native populations are most likely to experience SUD service gaps. By age, people who are 19−25 years old (transition-age youth) and adults ages 26−65 are most likely to face service gaps.

Opportunities to Support Improvements in SUD Care
Findings and recommendations to enhance support for individuals are informed by surveys and interviews conducted with SUD stakeholders from across the state. Recommendations highlighted in the report include:
What to Watch
The overarching challenges facing California’s recovery system are present in other states. These states can adapt the strategies discussed in this report to address their own SUD concerns. In California, as in other states, an important aspect of addressing SUD treatment involves strategic allocation of opioid settlement dollars. These funds, resulting from legal settlements with opioid manufacturers and distributors, are expected to play a significant role in improving the state’s SUD treatment infrastructure, especially when considered alongside available federal funding, demonstrations, and regulatory flexibilities.
Connect With Us
The upcoming HMA event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, will offer more opportunities to engage with leaders from various sectors who are advancing solutions to improve access to care and reducing access disparities. Throughout the conference, federal and state officials, community leaders, and national experts will shed light on the challenges and solutions to these issues.
New HMA Analysis: Options for Improving California’s Substance Use Disorder Treatment System
Community Health Centers (CHCs), also known as Federally Qualified Health Centers (FQHCs), are community-based health care providers that are vital lifelines in medically underserved areas.
Funded by the Health Resources and Services Administration (HRSA), they provide comprehensive primary and preventative care, dental services, mental health and substance use services, and supportive services like transportation and translation, for patients to access health care. In addition, we have supported more than 20 states to write their CCBHC planning grant applications to initiate a state-run CCBHC model. Most recently, we had 100% success rate for our FY23 planning grant applications, resulting in four states receiving one year planning grants to build a state-run CCBHC model.
FQHCs partner with HMA for expert guidance in strategic planning, board development, finance and operations, clinical improvement, understanding federal and state policy, advancing health equity, grant writing, community health needs assessment, expanding practice scopes, and executive coaching. HMA’s consultants bring extensive real-world and leadership experience and expertise working with FQHCs prior to joining HMA, offering FQHCs a range of services and support with:
In addition to working with FQHCs, HMA works collaboratively with multiple Primary Care Associations (PCAs) to leverage our expertise benefiting multiple FQHCs.
HMA’s FQHC value-based payment team has extensive experience working with PCAs, Health Center Controlled Networks, and FQHCs to form integrated delivery systems focused on the Medicaid and Medicare populations to help them progress along the CMS Framework for Value‐based Payments commensurate with their readiness. Current and recent projects have included PCAs and FQHCs in New York, Illinois, Rhode Island, Oklahoma, Wisconsin, Missouri, North Carolina, Montana, and Indiana.
HMA Principal Art Jones, MD, MPH, was the architect of the first FQHC APM in the country that transitioned payment from fee-for-service to capitation. It was adopted by the FQHC he led as CEO and four other Chicago-area FQHCs in 2001. In 2017, HMA helped the Washington Health Care Authority, the Washington Primacy Care Association, and its FQHC members develop a capitated FQHC APM. Since then, HMA has worked with PCAs and FQHCs in New York, Illinois, Rhode Island, Oklahoma, Wisconsin, Missouri, North Carolina, Montana, and Indiana to develop their own capitated FQHC APMs.
HMA Principal Art Jones, MD, MPH, partnered with five Chicago area FQHCs and five hospitals to establish Medical Home Network in 2011, the prototype clinically integrated network focused on underserved communities. Driven to solve social drivers of health and seeking to demonstrate that in the safety net, technology can be deployed to deliver superior outcomes, the network has grown to include 14 FQHCs and three health systems with more than 180,000 Medicaid beneficiaries with delegated responsibility for care management and global risk. It supports 80 FQHCs in eight states in Medicare ACOs. Another HMA principal was CEO of one of the founding FQHCs at the network’s inception. This model has been replicated in other states to benefit communities of need.
FQHCs in some states receive general revenue funding to support operations. HMA has extensive experience with federal-directed payment program rules that can secure matching federal funds that at least double and sometimes as much triple total funding depending on the state’s federal match rate for Medicaid. Directed payment programs require a value-based payment component. HMA has worked with three state PCAs to develop their programs.
HMA consultants assist FQHCs and their clinically integrated networks in assessing the value-based payment arrangements being offered by managed care plans and proactively designing proposals to take to payers. In many cases, HMA joins in active negotiations with the payer.
HMA has several clinically licensed consultants with experience working at and with FQHCs in their pursuit of value-based care. This includes assisting in NCQA Patient-Centered Medical Home certification, implementing care management programs, and designing and implementing new clinical models of care made uniquely financially feasible under APMs.
HMA has several experienced consultants helping individual FQHCs, State PCAs, and FQHC-led clinically integrated networks with their strategic planning process.
HMA has consultants focused on helping providers, including FQHCs, improve their billing and collections systems to improve cash flow and revenue.
HMA experts are uniquely positioned to help FQHCs and other organizations develop strategies and write for New Access Point and Service Area Competitions.
We believe in a data-driven approach to drive actionable insights. We start with an efficient assessment of your current state and prepare a roadmap for success. After our thorough and rapid assessment, our consultants work with your organization on any aspect of implementation to ensure a sustainable, high-performing empanelment environment that drives operational quality and optimizes
current and future revenue streams. A high-performing empanelment environment leads to optimized PCP continuity of care, accountable PCP and care teams driving clinical quality improvement, readily available appointment slots, and patient retention and productivity goals.
No matter the size, HMA empowers FQHCs to thrive in an ever-changing healthcare landscape. With deep expertise at every level, HMA teams partner with FQHCs nationally to address a wide range of operational challenges, including designing innovative school-based care, and expanding community health centers, optimizing scheduling and empanelment, integrating behavioral health care and strategically adopting telehealth solutions, we help FQHCs seize opportunities. Our experience extends to selecting and implementing cutting-edge IT systems for population health management, optimizing participation in the 340B program, and maximizing workforce capacity. HMA is dedicated to ensuring that FQHCs deliver exceptional care to those who need it most.
State PCAs frequently ask HMA to speak on various value-based payment-related topics at annual conferences.
Project Spotlight
Community Health Center, New York
HMA assisted the community health center in creating its strategic approach to value-based care. The project included analysis of current clinical and financial performance under managed care arrangements, workforce optimization, and opportunities to identify shared savings on total cost of care.
Health Center Strategic Planning, California
HMA worked with the board of directors, community stakeholders, clinicians, and staff to create a theory of change and then identify internal and external opportunities for expansion, quality improvement, and financial growth.
Community Health Center Service Area Competition (SAC) Grant, Ohio
HMA supported a CHC in completing its needs assessment and writing its SAC grant.
PACE readiness, Illinois
HMA consulted with an FQHC in Illinois to analyze, plan for, and apply to open a Program for All-Inclusive Care for the Elderly (PACE) focused on the Latinx population.
Learn more about our work
Contact our experts:





For many Americans, housing costs are out of reach, as 13 of the 20 largest occupations in the U.S. pay less than the housing wage. This housing crisis is impacting overall health and well-being and utilization of healthcare. Individuals and families struggling with homelessness often experience lower infant birthweights, mental health challenges, chronic disease, and higher mortality.
HMA works at the intersection of housing and healthcare in a variety of ways, including policy, programs, financing, and evaluation. A safe and secure place to live is fundamental to all of the healthcare and human services work we do at HMA. Our experts have developed and worked within programs in public housing authorities, hospital housing partnerships, shelters and transitional housing, post-incarceration transition and 1115 waiver supports, rural housing, and other housing supports.
HMA experts are former state and local public health leaders, directors of community-based organizations, and former senior officers from key federal agencies, setting us apart from other consulting companies.
We understand the complexity of designing and implementing change beyond the theoretical level – we have walked in the shoes of our clients and understand how to provide insight that is meaningful, actionable, and realistic.
Organizations we support
Federal, state and local government agencies
Managed Care Organizations
Public Housing Authorities
Community-based health/behavioral health and human service organizations
Provider organizations (FQHCs, CCBHCs)
Schools and universities
Departments of behavioral and public health
Healthcare systems and providers
Philanthropic organizations
Jails and correctional facilities
We Help Our Clients
Transform their community’s response to homelessness
Improve local housing delivery systems
Facilitate new or expanded community partnerships
Address systemic barriers
Build capacity of local partners and resources
Help with targeted impact improvements
Scale interventions to match resources and need
Increasing system capacity
Provide management tools for improved decision making
Planning and implementation support for continuum of homeless services
Affordable housing needs assessment
Consultation on shelter and outreach team best practices
Project Spotlight
The problem:
With new funding available and a homelessness crisis growing more acute, the JOHS requested an evaluation of the department’s effectiveness and barriers, as well as the governance model over all homelessness response functions.
How we helped:
HMA conducted a discovery process consisting of 40 stakeholder interviews with local elected officials, County and department staff, and contracted service providers. We also reviewed key contracts, policies and procedures, and other foundational documents; and completed a summary of national best practices to inform future program development. This resulted in a summary of gaps, opportunities and recommendations that HMA presented to a joint meeting of County and City Commissioners, and HMA continues to assist in implementation
The outcome:
HMA presented leaders with findings and recommendations, including reforms to provider payment, system governance, inter-agency partnerships and more). Subsequent contracted initiatives to support implementation include the renegotiation of an Inter-Governmental Agreement and action plans to improve to the shelter system and street outreach systems.
The problem:
Tens of thousands of residents of HUD assisted senior housing in California are dually eligible for Medicaid and Medicare and have complex medical, behavioral health, and health-related social needs. Affordable housing developers, owners and operators do not have financing to enhance resident supports to prevent homelessness, avoidable hospitalizations, or institutional care transitions. While evidence shows that Medicaid, Medicare and D-SNP plans and healthcare providers would reduce avoidable inpatient and urgent care costs from enhanced resident services, mechanisms to partner with housing organizations have been elusive due to different incentive structures, infrastructure, and cultures in each sector.
How we helped:
Through contracts with LeadingAge California, HMA supported California housing organizations to develop a compelling value proposition for strategic discussions with payers, providers, and foundations. HMA is developing a financing plan and gap analysis to braid and blend Medicaid, Medicare, D-SNP, workforce, behavioral health, and other funding streams to sustainably support enhanced services provided by trusted, culturally and linguistically responsive on-site service coordinators.
The outcome:
California DHHS and Department of Aging leadership endorsed the goals of the CICH model and are guiding next steps to develop the infrastructure and braided/blended financing plans. Two health plans in southern California are interested to partner in piloting the model.
The problem:
Housing and community development organizations are trusted resources in low-income rural and urban communities across the US; and they were instrumental during COVID in engaging high-risk communities in prevention activities. While housing and community development organizations are a natural place for successful CHW programs, most CHW models and training programs have been developed for healthcare organization environments.
How we helped:
HMA co-led a cohort of NeighborWorks network organizations to co-design three housing and community-development organization-centered CHW program models and a toolkit covering every element of standing up and sustaining a CHW program within housing and community development structures, values, and resources. We provided coaching and technical assistance to learning cohort participants to test toolkit components.
The outcome:
Web-based toolkit Community Health Workers: A Promising Program Model to Advance Health & Well-Being in Affordable Housing and Community Development – NeighborWorks America
The problem:
The organization has requested assistance with establishing healthcare partnerships, designing health care services to meet resident health needs in each affordable housing development, and identifying opportunities to expand health and wellness services.
How we are helping:
HMA is providing guidance in service planning, partnerships, resources, budgeting, and strategies. This may include identification of potential health care partners, design of the health care model, assistance with budgeting for health care service costs, and other consultation as requested.
The outcome:
HMA presented leadership with insight on how to expand embedded health services to optimize resident health across their housing portfolio, assisted with the design of health care services, and helped to build healthcare partnerships.
Our HMA experts are ready to help your organization support your communities.
Contact our experts:







This week’s second In Focus continues the conversation on drug policies and trends, providing updates and insights into the current landscape of Medicare’s drug price negotiations.
The Centers for Medicare & Medicaid Services (CMS) recently released the negotiated prices for the first 10 Medicare Part D drugs under the Inflation Reduction Act’s (IRA’s) negotiation authority. CMS plans to add more drugs to the negotiation list, including 15 additional Part D drugs in 2027 and 15 more products from both Part D (pharmacy benefit drugs) and Part B (mostly physician administered drugs). In 2029 and later years, another 20 drugs from either Part B or Part D will be chosen.
Negotiated Prices for First 10 Drugs Leave Unanswered Questions
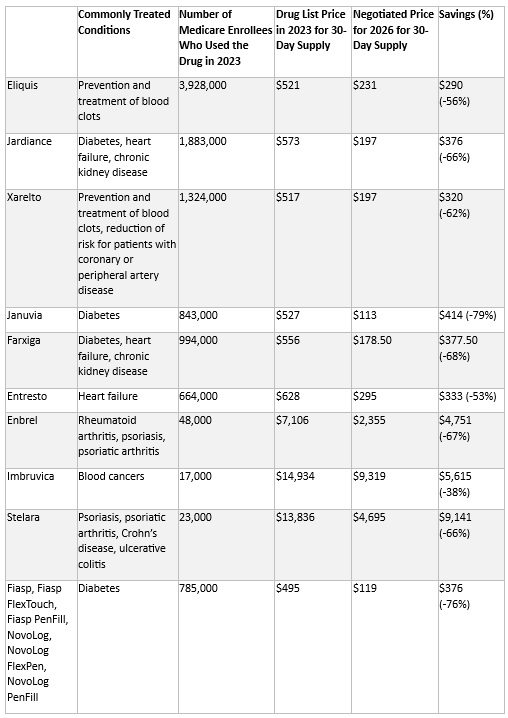
CMS estimates the negotiated prices for 30-day supplies of each medication will result in savings ranging from 38 percent to 79 percent compared with list prices when they take effect in 2026. This comparison, however, does not account for several factors that could affect the actual savings for the Medicare program and beneficiaries, including:
CMS is required to provide a detailed explanation of how negotiated prices were determined by March 1. The price comparisons with privately negotiated prices, however, will remain unclear and the effects on other payers and longer-term investments in new products may not be fully understood for some time. The table below lists the negotiated discounts for the first 10 drugs, which CMS selected from the top 50 Part D drugs by spending, which lacked generic or biosimilar alternatives and met other IRA criteria.
Negotiated Drug Prices Applicable in 2026
Looking Ahead
Age of Products and Role of Generic and Biosimilar Competition: Drugs eligible for negotiation are typically the highest expenditure drugs that have been on the market for at least seven years or 11 years in the case of biologics. Importantly, products with generic or biosimilar competition are exempt from negotiation. This exemption may increase the speed at which biosimilar or generic competition comes to market, as the IRA requires competitors to engage in bona fide marketing to exempt an innovator from negotiation. Despite approval, biosimilars for some of the drugs will remain subject to negotiated prices until their marketing efforts begin.1
Impact on Medicaid and Other Payers: The IRA’s negotiated discounts are not required to be available outside of the Medicare program. It remains uncertain whether other payers will use Medicare-negotiated prices as leverage in their own negotiations. For Medicaid, the direct impact of negotiations themselves is expected to be negligible; however, the IRA’s inflation penalties could encourage more manufacturers to moderate price increases over time, potentially leading to reduced inflation penalty rebates to state Medicaid programs.
Connect with Us
To explore these topics further, join Health Management Associates at the upcoming event, Unlocking Solutions in Medicaid, Medicare, and Marketplace. Engage with our Medicare experts below who will lead a small group discussion on trends in prescription drug policies during the pre-conference workshop.
For details on IRA pricing issues or other Medicare health policy developments, contact our featured experts below. HMA’s Wakely Actuaries also are available to discuss the IRA’s role in Medicare Part D.
This week’s In Focus covers key takeaways and insights from a recently released HMA report, State Approaches to Managing the Medicaid Pharmacy Benefit: Insights from a National Survey for State Fiscal Years 2023 and 2024.
The report, released in August 2024 with support from Arnold Ventures, includes survey responses from 47 states (including DC) for state fiscal years (SFYs) 2023 and 2024. The survey instrument builds on questions posed in the 2019 Medicaid Pharmacy Study of all 50 states and the District of Columbia, which HMA and the Kaiser Family Foundation conducted.
The report discusses state trends for how Medicaid pharmacy benefits are administered across the country, including planned priorities and anticipated challenges in SFY 2025 and beyond. The findings are based on information provided by the nation’s state Medicaid Directors, Medicaid Pharmacy Directors, and other Medicaid agency experts.
Pharmacy Benefit Administration
In many states, managed care delivery systems play a pivotal role in administering Medicaid benefits, including prescription drugs. As of July 1, 2023, survey results found that:
MCO states were surveyed about their use of carve outs for certain drug products/classes, inclusive of physician-administered drugs covered under the medical benefit.
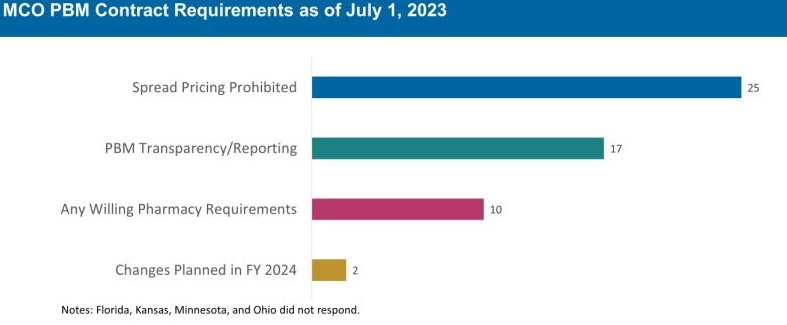
Pharmacy Benefit Managers
The significant role and market power of PBMs have prompted many state legislatures to enact greater transparency practices and require health plans to accept more responsibility for monitoring the PBMs they contract with, which reflect notable changes since the 2019 survey. More specifically:
The 30 MCO states that carve in pharmacy benefits responded to survey questions about PBM transparency and spread pricing requirements. Of these states:
The Role of PDLs, Prior Authorization, and Step Therapy in Controlling Drug Costs and Utilization
HMA’s experts also sought information on state payment strategies and utilization management protocols that are used to manage pharmacy expenditures. Nearly all responding states (44) have a preferred drug list (PDL) in place for fee-for-service prescriptions, which allow states to drive the use of lower cost drugs by encouraging providers to prescribe preferred drugs. Further, nearly two-thirds of responding MCO states (19 of 30 states) that do not carve out the pharmacy benefit reported having a uniform PDL for some or all drug classes, requiring all MCOs to cover the same drugs.
Many states have implemented step therapy and prior authorization (PA) guardrails in their Medicaid programs through legislation. However, 85.1 percent of responding states (40 of 47) report utilization controls like PA or step therapy applied to drugs that are reimbursed through the medical benefit to control utilization and costs. States also play an active role in managing MCO clinical protocols or medical necessity criteria, with 22 out of 30 MCO pharmacy carve-in states reporting that they require uniform clinical protocols for some or all drugs with clinical criteria. Approximately one-half of responding MCO carve-in states also require review and approval of MCOs’ PA criteria (15 of 30 states) and step therapy criteria (14 of 30 states).
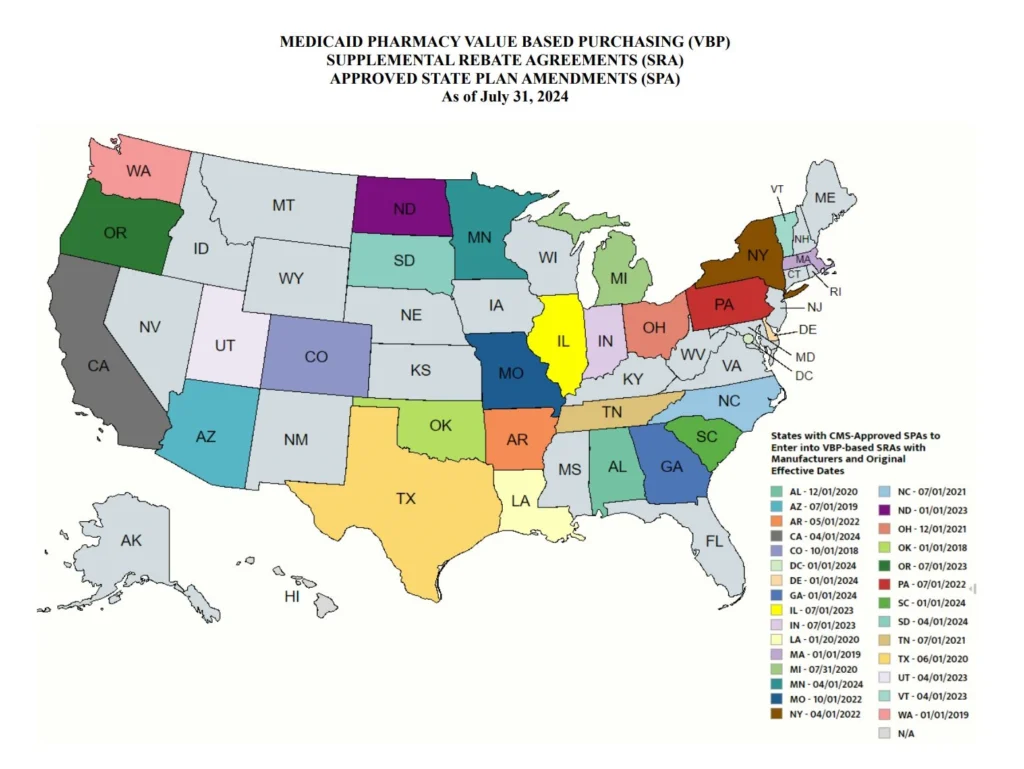
State Adoption of VBAs: Improving Patient Access to Cell and Gene Therapies
A growing number of states are actively considering entering into value-based arrangements (VBAs) with manufacturers, as pressure to improve patient access to cell and gene therapies increases. Nine states have at least one VBA in place, and 23 states reported that VBAs are among their future solutions for addressing coverage of new high-cost therapies. States will need to address common barriers to VBA implementation, which involves more upfront costs and operational challenges to implement than traditional contracts.
Subsequent to the submission of survey responses, the Centers for Medicare & Medicaid Services (CMS) released a Cell and Gene Therapy (CGT) Access Model, which begins with a focus on sickle cell disease, anticipated to go live on January 1, 2025. Under the model, CMS will negotiate outcomes-based agreements with manufacturers on behalf of the state to ensure that treatment pricing is related to treatment effectiveness. In the coming years, experiences with this model will help determine whether a CMS-led approach to developing and administering VBAs for CGTs improves Medicaid member access to innovative treatment and their impact on expenditures, if any.
Looking Ahead
Managing the Medicaid pharmacy benefit has never been more challenging. In FY 2025 and beyond, most states will be focused on managing their Medicaid pharmacy budgets, especially the development of VBAs and other policies and strategies for managing new high-cost therapies. Other top priorities and challenges cited by multiple states include management of PBM arrangements and considering coverage of the new generation of GLP-1 anti-obesity medications. States also must react to changing drug marketplace conditions driven, in part, by federal policy changes to the Medicaid drug rebate formula and changes designed to lower Medicare drug costs. Drug manufacturer responses to these changes have implications for Medicaid state budgets, but also for state PDL management decisions and beneficiary access to needed medications.
Connect with Us
The upcoming event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, hosted by HMA, will offer more opportunities to engage with report author Kathy Gifford at the pre-conference workshop Paying for Innovative Pharmaceuticals: State and Federal Trends Shaping Public Programs. Leaders from various sectors will join Kathy to discuss trends in prescription drug policies in public and commercial insurance programs.
For details about the report, contact our featured experts below.
