1310 Results found.


Unwinding recent Supreme Court rulings: impact on healthcare and beyond
This week, our In Focus section provides an initial overview of recent US Supreme Court rulings that reshape the landscape of national healthcare policy and operations. These decisions, ranging from redefining federal agency powers to addressing local ordinances that will affect people who are unhoused, are poised to have far-reaching implications across the federal and state governments.
The Decisions
A significant ruling came on June 29, 2024, with the Court overturning the precedent established in the 1984 Chevron v. Natural Resources Defense Council ruling. This year’s decision in Loper Bright Enterprises v. Raimondo marks a pivotal shift by eliminating the deference traditionally granted to federal agencies’ interpretations of ambiguous statutes. By empowering courts to clarify vague legislation, the ruling raises fundamental questions about the future of existing regulations and may lead to a surge in litigation challenging federal agency interpretations. The Court did state this ruling would have no impact on past decisions regarding the Chevron doctrine. The decision would apply only to current, pending, and future cases. When read in conjunction with the “major questions doctrine” announced in 2022 in West Virginia v. Environmental Protection Administration, agencies now face more challenges to regulations under a legal structure that does not provide deference to the agency.
The Court in Corner Post, Inc. v. Board of Governors of the Federal Reserve System also significantly reduced the ability of agencies to rely on statutes of limitations to avoid challenges to older regulations.
In a separate ruling that garnered attention, the Supreme Court upheld local ordinances in Grants Pass, OR, that restrict individuals experiencing homelessness from using blankets, pillows, or cardboard boxes for shelter in public spaces. The majority opinion in City of Grants Pass, Oregon v. Johnson supported the city’s stance that these ordinances, aimed at prohibiting camping on public property, do not constitute cruel and unusual punishment under the Constitution. This decision has sparked considerable debate over the balance between municipal governance and constitutional protections for people who are unhoused.
Also portending effects for the healthcare industry is the Court’s decision that defendants facing civil monetary penalties from the US Securities and Exchange Commission have a right to a jury trial. The Securities and Exchange Commission v. Jarkesy decision presents new considerations for healthcare and life sciences companies facing civil monetary penalties from the US Department of Health and Human Services.
What’s Next
The implications of these rulings are poised to reverberate throughout both federal and state governments. Stakeholders across healthcare and beyond must prepare for a period of adjustment and adaptation. Numerous questions regarding implementation and enforcement will likely emerge. The outcomes could trigger a wave of legal challenges and legislative responses as stakeholders navigate the evolving regulatory landscape.
Future In Focus sections will dive deeper into the potential impacts these decisions will have on healthcare policies and partnerships with related sectors. These insights will be pivotal in guiding strategic decisions amid the evolving legal framework.


Economic Analysis of Opioid Use Disorder in the Medicare Fee-for Service Program
This report quantifies the economic impact of opioid use disorder (OUD) specific to the Medicare fee-for-service (FFS) program, which covers approximately 51.6 percent of Medicare beneficiaries. We find that the cost to Medicare for managing these newly diagnosed patients was $29,669 more per patient than the propensity-matched control patients without OUD in 2022. We thus estimate that newly diagnosed OUD patients cost the Medicare program $4.3 billion in 2022. If these incident patient results were extrapolated into a 10-year budgetary impact analysis and if we assume constant rates of OUD incidence in the Medicare population, we estimate that the 10-year impact of OUD to the Medicare program would be $62.56 billion.
Our analysis demonstrates that OUD results in significant Medicare spending, including rising costs to beneficiaries through copayments and increased premiums. Additional work may be needed to determine whether the cost differential for incident patients with OUD generalizes to prevalent OUD patients as well. Though the 10-year budgetary impact figures require extrapolation and assumptions about future OUD use, they illustrate for policymakers the size of the fiscal challenge created by OUD in the Medicare population.
The case for a state-based marketplace
Former Speaker of the House Tip O’Neill made famous the phrase “all politics is local,” meaning electoral success is related directly to a politician’s understanding of and ability to address the local issues that matter most to constituents. The Commonwealth Fund applied this notion to health care in conclusions of a 2017 study of state year-over-year improvements in their rankings on the organization’s Scorecard on Local Health System Performance. This concluded that local knowledge of health care challenges and collaboration among local organizations to find solutions were major contributors to communities’ improvement on scorecard rankings.
One state-level decision that can boost responsiveness to local needs is whether to establish a state-based marketplace (SBM) for health insurance. Health insurance marketplaces are required in every state under the Affordable Care Act (ACA). Under the ACA, states were given a choice about whether to establish an SBM and receive some federal funding to do so or rely on the federally facilitated marketplace (FFM) to serve their residents. Marketplaces are designed to do two basic things: (1) enroll individuals and families who do not have access to Medicaid, Medicare, or employer-sponsored health insurance coverage in private coverage and (2) connect eligible individuals with financial assistance (premium tax credits and cost-sharing reductions) to reduce their cost of coverage. To date, 19 states have established SBMs and others continue to entertain the possibility of establishing one.
Why would states want to establish and operate a new agency of government to administer coverage for people who are receiving federal tax credits for their health insurance coverage? Surely this could create redundant and/or uncoordinated functions between states and the federal government and place an unwanted burden on capacity-strapped state governments. However, states that have established SBMs have not found this to be the case. Instead, in evaluating the FFM versus SBM decision, and in operating SBMs, states have found that SBMs offer distinct advantages over the FFM. These include:
- Lower Costs: States have historically demonstrated that they can operate SBMs at a lower overall cost than they would pay in fees through the FFM which has led, in part, to the recent reductions to the Healthcare.gov user fee. States also directly benefit through their ability to retain marketplace revenue and spend it locally. Lastly, SBMs can claim federal financial participation for functions they perform supporting and facilitating Medicaid enrollment.
- Better Service: States have an almost 60-year history of enrolling low-income individuals and families enroll in and stay enrolled in Medicaid. Many of these individuals cycle in and out of Medicaid eligibility due to changes in income. States can coordinate between SBMs and Medicaid to reduce gaps in coverage. They also can simplify eligibility and enrollment through SBMs that deliver a better customer experience through knowledge of their markets and residents and on the ground enrollment assistance and initiatives.
- More Policy Influence: SBMs can be launchpads for access and affordability innovations not possible with the FFM. State innovations to date include public option plans, state-funded subsidies such as premium and cost-sharing wraparound support, basic health plans, undocumented immigrant coverage programs, and collaborative enrollment initiatives with Medicaid agencies, unemployment programs, and tax departments.
In addition to states, managed care organizations (MCOs), particularly local and regional MCOs, can also reap the benefits of an SBM:
- Local Governance: With governance for an SBM taking place at the state level (versus the federal level), MCOs have the opportunity for more thorough engagement with state officials around operational and policy decisions and issues.
- Aligned Market Expectations: MCOs participating in both the marketplace and Medicaid will benefit from a higher probability of aligned expectations and priorities across both markets with those expectations and priorities being uniformly set at the state level with an SBM.
- Local Market Sensitivity: MCOs that operate and are rooted locally can count on market-specific dynamics being better reflected in decision-making with an SBM.
Establishing a SBM is not an easy or straightforward decision, but state policymakers and MCOs should consider the benefits that have accrued to other states and the role that SBMs can serve in addressing local health priorities.
If you have questions about how HMA can support your state or MCO related to SBMs, please contact our featured experts.
Zeroing in on Medicare Advantage policies set to transform the SNP landscape beginning in 2025
Regulatory policy changes finalized by CMS aim to increase the percentage of dual-eligible individuals enrolled in integrated plans
This week, our In Focus section delves into important and complex regulatory policy changes that affect coverage and services for the 12.9 million individuals who are dually enrolled in both Medicare and Medicaid. These policy changes—which were finalized as part of a broader final rule that the Centers for Medicare & Medicaid Services (CMS) released on April 4, 2023—are designed to increase the percentage of dually eligible people who are enrolled in integrated Medicare Advantage (MA) Dual Eligible Special Needs Plans (D-SNPs). The modifications will be phased in gradually, with certain provisions affecting D-SNPs starting in 2025. These adjustments forge a stronger connection between state-level policy and operational decisions, shaping the future landscape of D-SNPs.
Overview
Amid rapid growth of D-SNP plan offerings and increased enrollment of dually eligible individuals into D-SNPs, CMS has finalized an interconnected set of regulatory policy changes to increase enrollment in integrated plans while simplifying coverage and plan options for this population.
By promoting enrollment in integrated plans, CMS seeks to improve the care experience and outcomes for dually eligible individuals, with the ultimate goal of making integrated plan enrollment the standard. Integrated D-SNP plans, which consolidate Medicare and Medicaid services under one managed care organization, offer uniform consumer protections (including unified grievance and appeals process), integrated plan materials, and more coordinated care.
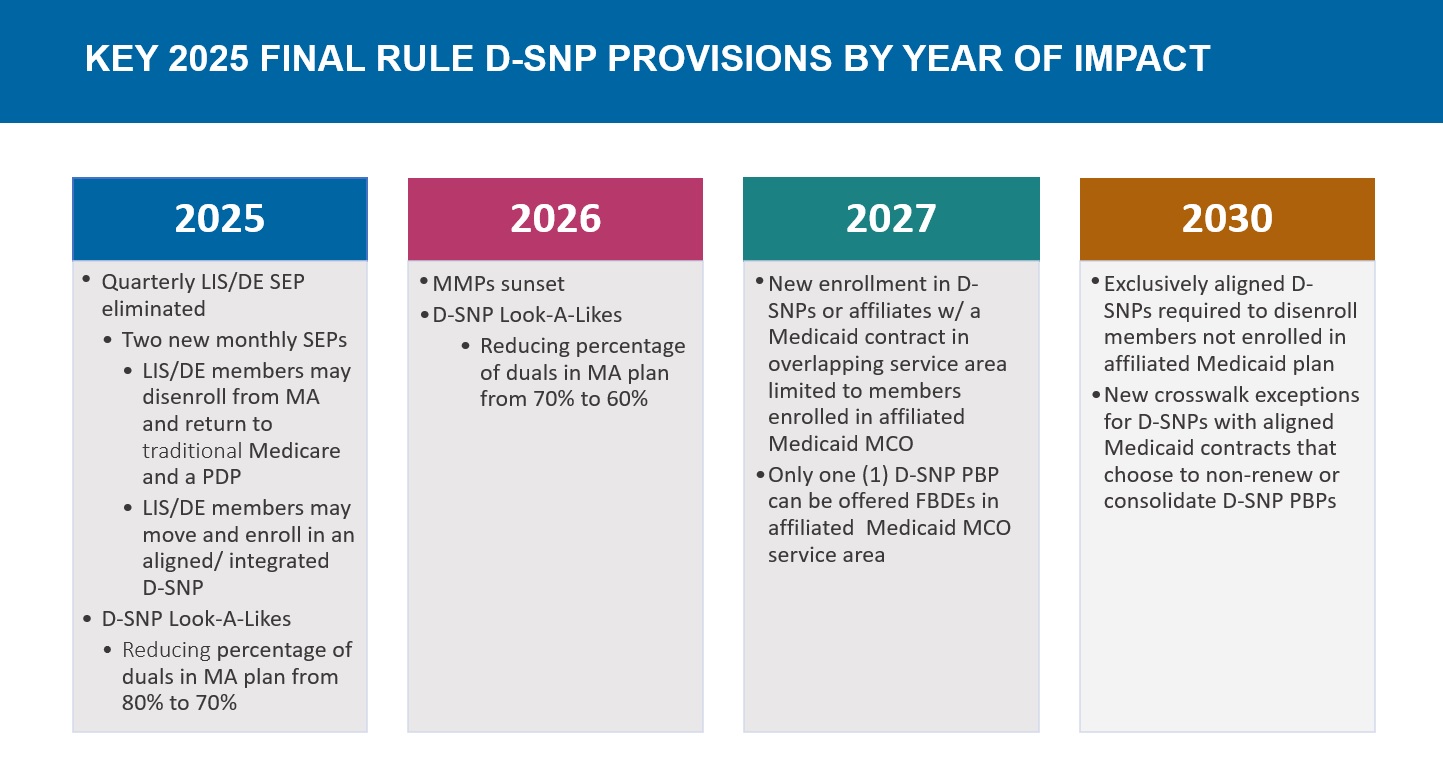
Key policy changes include:
- Replacing the current quarterly special enrollment period (SEP) with a monthly SEP for dually eligible and other low-income subsidy (LIS) individuals to enroll into a standalone prescription drug plan (PDP)
- Establishing a new integrated care SEP that will enable dually eligible individuals to choose an integrated D-SNP plan on a monthly basis
- Restricting enrollment in certain D-SNPs to individuals also enrolled in an affiliated Medicaid managed care organization (MCO)
- Limiting the number of D-SNPs an MA organization can offer in the same service area as an affiliated Medicaid MCO to reduce and simplify plan offerings for dually eligible individuals.
What Issue is CMS Trying to Solve?
CMS intends to make it easier for dually eligible people make enrollment decisions. Simplified plan options and more integrated care could prevent beneficiaries from inadvertently selecting plans that fail to provide the comprehensive Medicare and Medicaid benefits they need.
This shift toward aligned enrollment could improve beneficiary experiences, enhance outcomes, and streamline administrative processes for CMS. The introduction of a monthly SEP specifically for dually eligible individuals enrolled in Medicaid managed care plans underscores CMS’s commitment to facilitating enrollment in affiliated D-SNP plans throughout the year. Health Management Associates (HMA) experts expect these changes to affect the sales cycle for dual eligibles and potentially increase member satisfaction, expand access to care, and improve overall health outcomes for this population.
Timeline of Regulatory Changes
Considerations for Health Plans
The impact on individual health plans hinges on state-specific approaches to dually eligible beneficiaries and D-SNPs, as well as each plan’s strategy for integrating Medicare and Medicaid services. HMA experts identified the following key factors as essential for understanding and monitoring these interconnected dynamics:
- Does the state administer managed Medicaid, and if so, does it include the dually eligible population?
- Does the Medicare D-SNP (or an affiliated/ related company) hold a state Medicaid contract that covers dually eligible individuals?
- What is the state’s vision regarding duals and D-SNPs?
- Does the state require its Medicaid contractors to offer a D-SNP?
- Does the state currently or plan to restrict D-SNPs to their Medicaid contractors?
- Is the state moving toward an exclusively aligned enrollment model?
What’s Next
The changes in D-SNPs present opportunities and risks for beneficiaries, MA and Medicaid health plans, and states. Successful navigation of these changes requires proactive planning and anticipation of forthcoming federal and state regulations. Health plans operating within the D-SNP space must actively engage with state Medicaid agencies to understand and potentially help shape this evolving environment. For example, health plan strategies may include:
- Understanding the state’s priorities and its current and planned approach to integrated care for dually eligible individuals
- Participating in and/or advocating for stakeholder meetings with the state regarding dually eligible members and D-SNPs to ensure the opportunity to shape regulations
- Developing internal integration strategies that align product design, operations, quality, clinical, and member experience capabilities for D-SNPs and Medicaid
- Strategically planning actions, such as participating in Medicaid procurements, to achieve the plan’s objectives
Connect with Us
These regulatory changes significantly affect dually eligible beneficiaries, states, and both Medicare and Medicaid health plans. Though some changes may disrupt the duals’ market, others align state objectives with plan strategies. Ultimately, dually eligible individuals with full benefits will gain the most, experiencing improved opportunities to choose suitable plans, access necessary care, and achieve optimal health outcomes and well-being.
For further insights into these upcoming changes, view the D-SNP Growth and Integration: Key Implications of the 2025 CMS Final Rule webinar, featuring our experts below. Join them and other experts at HMA’s Fall Conference to stay informed about the strategic directions plans and states are pursuing.
Unlocking Solutions in the Medicaid, Medicare, and Marketplace programs
HMA is hosting its 2024 Fall Conference October 7−9 in Chicago, IL. Unlocking Solutions in Medicaid, Medicare, and Marketplace Programs promises to enhance your ability to navigate and shape healthcare programs and systems, focusing on improving health and well-being.
In a landscape dominated by endless video meetings, the HMA Fall Conference offers a refreshing change. Join us for an enriching experience featuring:
- Engagement with healthcare experts and thought leaders who are actively collaborating with stakeholders
- Participation in face-to-face discussions to exchange ideas and receive valuable feedback
- Opportunities to connect with peers who are committed to strengthening public programs and enhancing health outcomes
Keynote Address and Sessions
Darshak Sanghavi, MD, from the Advanced Research Projects Agency for Health (ARPA-H), will deliver the Keynote Address. He and other speakers will inspire attendees to explore innovative healthcare programs and their potential impacts on healthcare delivery, reimbursement, and health outcomes.
The conference will feature a diverse array of speakers and participants, including C-suite executives from national, regional, and local health plans. Federal and state leaders joining panels will include:
- State Medicaid directors from New York, Iowa, New Mexico and Alabama
- State insurance commissioners
- Behavioral health agency officials
- State housing agencies
- Leaders from the US Interagency Council on Homelessness
The conference will include a revamped pre-conference workshop on October 7, featuring hands-on exercises and interactive sessions led by HMA leaders. Sessions will include a value-based care contracting exercise, a value-based purchasing assessment discussion for providers, tips and tricks on navigating Medicaid section 1115 demonstrations, AI applications in healthcare, and more.
View the agenda and event details, including speakers confirmed to date.
Registration
Early bird registration is open until July 31. Don’t miss this opportunity to gain actionable knowledge, forge valuable connections, and discover fresh insights and best practices. Register now to secure your spot at the forefront of healthcare innovation.

Let’s Stop Doing Stupid Things: How Can We Scale Digital Healthcare Innovation to Ease the Burden on Patients and Providers?
Ryan Howells is a leading expert in digital health policy and interoperability from Leavitt Partners, an HMA company. Ryan has been a catalyst for change since the early days of the internet to his current role in advancing consumer-directed health data exchange through application programming interfaces (API). In this episode, he discusses the evolution of digital health, the challenges of data accessibility, and the transformative potential of AI in healthcare. Whether you’re a healthcare professional or simply interested in healthcare innovation, this podcast offers practical solutions and visionary insights that can help reimagine the way we deliver and experience healthcare.
HMA’s Medicare team unites consultants from multiple HMA companies to assist clients in all aspects of Medicare
As HMA has grown, we have added significant breadth and depth to our Medicare team to better offer our clients comprehensive expertise on Medicare, Medicare Advantage, Dual-Eligibles, payment systems, pricing, and more. When looking for a partner to help navigate the complexities and changes of Medicare, our clients know that by engaging HMA experts they are engaging former CMS officials, former plan executives, payment system and coding experts, policy analysts, and many others. We draw on the resources of experts from our HMA companies to provide comprehensive and end-to-end solutions, including Wakely Consulting Group and Cirdan Health Systems and Consulting for actuarial services, and Leavitt Partners for political and policy engagement. Together we bring considerable expertise in all things Medicare and can leverage our more than 700 consulting colleagues across HMA.
Our world-class Medicare team partners with clients to meet their needs, address their challenges and improve their bottom line. We provide a variety of services such as:
- Significant support for Medicare Advantage (MA) plans and stakeholders seeking to understand MA policy and operational issues including strategy, market assessment, models of care, evaluation, and audit support.
- Support MA special needs plans (D-SNP, I-SNP, C-SNP, etc.) and programs for dual eligible beneficiaries.
- Medicare regulatory, analytics and thought leadership consulting services for MA plans, providers, suppliers, value-based organizations, associations, and foundations.
- Design, implementation, evaluation and analysis of Medicare value-based payment systems and policy issues.
- Program of All-Inclusive Care for the Elderly (PACE) strategy and operations.
- Strategic advice, policy development, and budgetary analysis for clients seeking assistance with Medicare reform efforts.
- Medicare coverage and reimbursement for device, drug and biotechnology manufacturers and other stakeholders in the life sciences community.
- Assistance for clients seeking to commercialize new technologies.
- MA and fee-for-service claims analysis and actuarial services with support from actuaries within HMA plus actuaries from Wakely Consulting Group and Cirdan Health Systems and Consulting.
- Consulting and federal policy analysis, including Congressional Budget Office (CBO) scoring and legislative policy development with our colleagues from Leavitt Partners.
In 2021, HMA acquired The Moran Company (TMC), which provides extensive expertise in the design, implementation, and evaluation of various healthcare payment systems, with a particular focus on the Medicare program. As we approach the 26th anniversary of TMC’s founding and the third anniversary of joining the HMA portfolio, we want to honor the history and contributions of The Moran Company and remember the late Donald Moran who founded TMC in July 1998. He spent almost 50 years in the health policy community, including many years in government service, serving as executive associate director for Budget and Legislation at the U.S. Office of Management and Budget during the Reagan Administration.
Many of our TMC colleagues worked with Moran for more than a decade, benefiting from his mentoring and exhaustive knowledge of the industry. Since joining, TMC consultants have worked closely with our HMA colleagues and the Medicare team in particular.
As of July 1, we are retiring the Moran brand and logo and fully integrating the company into HMA as part of the Medicare team. We may be dropping the Moran brand name, but not the approach and diligence for which TMC is well known. In particular, HMA will continue to use the same methodologies for Congressional Budget Office scores and Medicare data analyses that have characterized Moran’s work for more than 25 years.
View some of our recent work from our combined team:
Case Studies
- Appropriate payment for transformative therapies to secure patient access to CAR Ts
- Patient journey analysis for a new oncology drug
- Helping life science manufacturers navigate Medicare payment systems
Reports
Webinar

HMA helps Justice Involved/Behavioral Health services implement the Sequential Intercept Model (SIM)
The Sequential Intercept Model (SIM) provides a framework to help local governments divert individuals with behavioral health issues from the criminal justice system into community resources.
The model serves communities by helping them identify opportunities for diversion programs, known as “intercepts”, with the highest potential for success based on community strengths and needs. Created by Policy Research Associates in 2004 and promoted by SAMHSA’s GAINS Center, SIM identifies critical diversion points tailored to each community’s strengths and needs.
Key Benefits of Implementing SIM
Guides ongoing stakeholder meetings and county programming by establishing a common language for justice and diversion programs to support sustainability and adaptability over time.
Supports community analysis and integration of new policies by providing a clear visualization of system resources and gaps.
Facilitates collaboration and ensure efficient use of resources by enhancing communication and relationships across systems.
Collects local data for system analysis to identify grant opportunities and funding for critical intercept program development.
Development of a SIM report that highlights current state, gap, and opportunities for improvement.
Educates county leaders on best practices to help assess new programs and identify areas for improvement.
Addressing Community Challenges
SIM supports development of community prevention programs that lower the chance of initial involvement into criminal justice for many, helping provide the needed level of treatment support. The framework further allows jurisdictions to develop meaningful and effective programs to address issues faced by justice-involved individuals, such as unstable housing and income, high overdose risks, and the impact of evolving policies. Many existing programs lack sustainability due to reliance on temporary funding, and traditional planning has been reactive rather than proactive. SIM offers a comprehensive framework for communities to support individuals with behavioral health issues, improving safety and resource efficiency.
HMA’s services include:
- Facilitating stakeholder meetings and data collection.
- Mapping current systems and identifying key intercepts.
- Developing SIM reports to highlight gaps and opportunities.
- Leading strategic planning for program development.
- Setting measurable goals and evaluation plans.
If you are ready to talk about implementing a SIM and the next steps for your organization, reach out to our experts today.
Contact our experts:
