1305 Results found.


Raising the bar: Improving health equity through actionable frameworks
This week, our In Focus section highlights an initiative, Raising the Bar: Healthcare’s Transforming Role (RTB), which is designed to strategically address inequities in the healthcare system. Leading this effort is the National Alliance to Impact the Social Determinants of Health (NASDOH), an alliance convened by Leavitt Partners, a Health Management Associates (HMA) Company, with support from the Robert Wood Johnson Foundation (RWJF).
Overview
There is significant and increasing demand across health and human services to address health inequities and eliminate disparities in service delivery and positive health outcomes. Organizations are asked to provide healthcare in holistic ways that recognize both individual and population-level needs.
Raising the Bar is a framework and a call to action for the healthcare sector to embrace all levers, resources, and opportunities available to advance equity and excellence. Raising the Bar seeks to accelerate the healthcare sector’s efforts to achieve equity and to improve the healthcare experience and well-being of individuals, families, and communities.
The Framework for Driving Action
The RTB project worked with healthcare leaders and people who have experienced inequities in the system to develop an actionable framework for the entire healthcare sector, which would embed equity and excellence throughout its work. The NASDOH convened extensive discussions with providers, hospitals, payers, and community leaders to develop foundational principles, essential roles, and concrete actions for the sector to achieve equity goals, big and small.
Raising the Bar Principles. The project generated five principles that put the priorities of individuals, families, and communities at the center of healthcare. They were informed by discussion with organizations and people who give, get, and pay for care.

Raising the Bar also identified four essential roles for individual contributors to the healthcare system and provide concrete actions they can take to transform how care is delivered.

Embedding Approaches to Address Health Inequities
Now in the next phase of this work, HMA consultants are working one-on-one with five organizations committed to embedding approaches to address health inequities by implementing the framework within their own systems of care. Participating organizations include a multi-site, multi-state Catholic health system, an academic medical center, an independent health system, one certified community behavioral health clinic, and one county public health department. The entities vary by geography, demographics, population size, and rural and urban location.
Each of the following sites is using the Raising the Bar framework and individualized coaching to meet their equity goals:
- Charles County Department of Health, White Plains, MD
Charles County is working to develop and strengthen trusting partnerships with local community organizations representing diverse populations to address health inequities in the county. - CHRISTUS Health, Texas, Arkansas, and Louisiana
CHRISTUS is developing an enterprise-wide six-year health equity road map that includes a strategy to build a community health worker sustainability. - Gaudenzia, Baltimore, MD
Gaudenzia is working to develop and implement a road map for establishing a Consumer Advisory Committee (a Substance Abuse and Mental Health Services Administration requirement for certified community behavioral health centers) that other Gaudenzia sites can use and spread nationwide. - Jefferson Health, Philadelphia, PA
Jefferson is conducting an enterprise-wide assessment and creating a governance structure for its health equity initiatives across multiple healthcare and medical education sites throughout their catchment area, which crosses state lines. - Sturdy Health, Attleboro, MA
Sturdy is creating an enterprise-wide health equity dashboard with measures that align with organizational goals and strategies and developing staff training to improve service delivery for populations who experience inequities in care.
The five entities are receiving individualized coaching from HMA health equity experts over a one-year period using the Raising the Bar framework and each organization’s self-identified goals and objectives. At the project’s completion, findings from the project will be published in the Raising the Bar implementation guidance, developed in partnership with the Health Care Transformation Taskforce.
Continue the Conversation
Raising the Bar will be featured in discussions during the HMA Fall conference in Chicago, October 7-9. In the opening plenary session on social determinants of health, Leticia Reyes-Nash and Sara Singleton will describe some of the work, and during a breakout session, speakers from some the organizations participating in this project will share their experiences.
For more information about Raising the Bar or the types of technical assistance that HMA can provide to organizations seeking to further develop equity in their practices and communities, contact our featured experts below.
Learn more at rtbhealthcare.org.
For details about HMA’s work in health equity, visit:
- Health Equity and Equity-Centered Strategic Approaches
- Rural Health and Challenges with Health Equity
Continue the Conversation
Raising the Bar will be featured in discussions at Unlocking Solutions in Medicaid, Medicare, and Marketplace, a conference powered by HMA taking place in Chicago, October 7-9.

How Can We Better Transition Healthcare Services for People Leaving Incarceration?
Linda Follenweider, an advanced practice registered nurse and board-certified family nurse practitioner with extensive experience in correctional healthcare, discusses the critical gaps in continuity of care for incarcerated individuals. She emphasizes how many receive necessary medical care while in jail or prison but struggle to maintain this care upon release. Highlighting the significant health risks and economic costs associated with this disconnect, she advocates for integrating correctional healthcare into the broader healthcare continuum. The episode showcases the opportunities presented by adopting routine screening questions about incarceration history to ensure better health outcomes and resource utilization.
CMS’s CY 2025 Medicare proposed rules support primary care, care coordination, and increased access for beneficiaries
This week, our In Focus section provides an overview of the two key Medicare proposed payment rules that the Centers for Medicare & Medicaid Services (CMS) released last week—the Physician Fee Schedule (PFS) and the Hospital Outpatient Prospective Payment System (OPPS). These two rules include policies that will affect a variety of providers. Below we highlight some key provisions. Comments on these proposals are due to CMS in early September.
PFS Proposed Rule for 2025
Released on July 10 and with comments due by September 9, this wide-ranging regulation proposes policy changes for many different types of providers.
PFS Payment Update: The estimated 2025 PFS conversion factor is $32.36, a $0.93 or 2.80 percent decrease from the calendar year (CY) 2024 level of $33.29, which included a one-time update required by statute. In previous years with cuts like this one looming, Congress has stepped in and adjusted the payment update in the positive direction. Congress is now considering approaches to do so again for this year.
Caregiver training services (CTS): CMS is proposing a new code for caregiver training for direct care services and supports such as wound dressing changes, infection control, and medication administration. These services could be provided via telehealth.
Telehealth services: CMS is proposing to add several new codes to the telehealth list and to refine a variety of policies related to the type of technology that must be used and what supervision must be provided for telehealth services and other requirements such as removing frequency limitations. Nonetheless, several telehealth flexibilities will end December 31, 2024, because of the expiration of pandemic era expansions unless Congress extends or makes telehealth flexibilities permanent.
Advanced primary care management services (APCM): CMS proposes to create a new set of APCM codes that would incorporate parts of several existing care management and communication technology-based services into a monthly bundle of services. The billing codes are differentiated by three levels based on a person’s number of chronic conditions and enrollment as a qualified Medicare beneficiary to reflect patient medical and social complexity. These APCM services could be provided by advanced primary care teams and are tied to primary care quality measures.
CMS seeks feedback on whether the agency should consider additional payment policies to recognize the delivery of advanced primary care, including on potential changes to coding and payment policies within traditional Medicare such as for additional bundles of services.
Behavioral health services: CMS is proposing new codes for behavioral health crisis services, including safety planning and interventions for patients at risk of suicide or overdose, follow-up contact after a crisis emergency department (ED) visit, for digital mental health treatment (DMHT) services, and for nonphysician practitioners to bill for interprofessional consultations.
Screening and risk assessment: The agency updates and expands coverage for screening and preventive services, including proposals to cover screening computed tomography colonography (CTC) for colorectal cancer, drugs covered as additional preventive services, the hepatitis B vaccine, and cardiovascular risk assessment and risk management.
Dental and oral health services: CMS proposes to add services provided to Medicare beneficiaries with end-stage renal disease to the list of clinical scenarios in which Medicare payment may be made for dental services. CMS also seeks comments on other clinical conditions appropriate for coverage.
Improving ambulatory specialty care: CMS seeks stakeholder feedback about a potential Innovation Center model that would increase specialist participation in value-based care through Merit-based Incentive Payment System (MIPS) Value Pathways (MVPs) and expand incentives for primary and specialty care coordination.
Medicare Shared Savings Program (MSSP): CMS is proposing several refinements to the permanent accountable care program. These include a prepaid shared savings option that lets eligible accountable care organizations that have previously earned shared savings to receive advanced earned shared savings to make investments that support beneficiaries, the addition of a health equity benchmark adjustment (HEBA) that increases an ACO’s historical benchmark based on proportion of beneficiaries who are enrolled in the Medicare Part D low-income subsidy (LIS) or dually eligible for Medicare and Medicaid, changes to the MSSP quality measure set to align the measure with the universal foundation measure set and seeking comment on creating a risk track that is higher than what currently exists.
Rural health clinics and federally qualified health centers: CMS proposes several changes to update payment and coverage of services provided in these facilities including care coordination services, vaccines, and dental services.
Payment for major surgical procedures: CMS makes coding proposals to address scenarios in which follow-up care for beneficiaries who have undergone major surgical procedures is provided by different clinicians in different group practices.
Opioid treatment programs: CMS makes several proposals related to opioid treatment programs, including allowing assessments conducted via audio-only telecommunications, and increasing payments for social determinants of health (SDOH) risk assessments. CMS also proposes to pay for new FDA-approved opioid agonist and antagonist medications.
2025 Medicare Hospital OPPS Proposed Rule
CMS released the Medicare Hospital OPPS proposed rule on July 10, 2024, with comments due by September 9, 2024. This regulation proposes policy changes that largely impact hospital outpatient departments and ambulatory surgery centers (ASCs).
OPPS and ASC Updates: CMS proposes to update OPPS rates for hospitals that meet applicable quality reporting requirements as well as ASCs by 2.6 percent.
Access to non-opioid pain relief: The Consolidated Appropriations Act (CAA) of 2023, provides temporary additional payments for certain non-opioid treatments for pain relief in hospital outpatient department (HOPD) and ASC settings from January 1, 2025, through December 31, 2027. CMS proposes to implement this law with proposals on the evidence requirements for medical devices and the Food and Drug Administration (FDA)-approved indications that would meet the criteria for the temporary additional payments. CMS has identified seven drugs and one device that would qualify as non-opioid treatments for pain relief and proposes that they receive separate payment in 2025. CMS also is soliciting comments on other products that may qualify for these payments.
Justice-involved individuals: To support individuals returning to the community from incarceration, CMS proposes to narrow the definition of “custody” in Medicare’s payment exclusion rule and to revise the Medicare special enrollment period (SEP) for formerly incarcerated individuals. These modifications would remove real or perceived barriers to Medicare access for individuals who have recently been released from incarceration or are on parole, probation, or home detention.
Maternal health: CMS is proposing several new maternal health related requirements for hospitals and critical access hospitals (CAHs). The proposed changes to conditions of participation, include new requirements for maternal quality assessment and performance improvement; baseline standards for the organization, staffing, and delivery of care within obstetrical units; and annual staff training on evidence-based maternal health practices. CMS further proposes changes to the emergency services requirements related to emergency readiness for hospitals and CAHs that provide emergency services.
Connect with Us
HMA’s Medicare policy experts collaborate to monitor legislative and regulatory developments in the physician, outpatient, and ASC policy arenas and to assess the impact of changes in these reimbursement systems. HMA’s Medicare experts interpret and model policy proposals and use these analyses to assist clients in developing their strategic plans and comment on proposed regulations.
For more information or questions about the policies described below, please contact our experts below.
CMS invites states to apply for transforming maternal health model
This week, our In Focus section reviews the notice of funding opportunity (NOFO) for the Transforming Maternal Health (TMaH) Model, which the Centers for Medicare & Medicaid Services (CMS) Center for Medicaid and Medicare Innovation (the Innovation Center) announced on December 15, 2023. States interested in participating in this model must submit an application to CMS during the competitive application process.
As described in a December 2023 In Focus, pregnancy-related deaths have more than doubled since 1987 to 17.6 deaths per 100,000 live births, with health disparities only worsening outcomes for different racial and ethnic groups. For example, the pregnancy-related mortality rates for Black and Native American and Alaska Native people are approximately two to three times higher than the rate for White people. In recent years, 38 states have extended postpartum coverage, and 11 states now offer doula coverage for Medicaid enrollees. This initiative accelerates the focus on maternal outcomes and, with Medicaid paying for nearly 43 percent of births, has the potential to affect health across generations.
This model is designed exclusively to improve maternal healthcare for people enrolled in Medicaid and the Children’s Health Insurance Program (CHIP). The TMaH model takes a whole-person approach to pregnancy, childbirth, and postpartum care, addressing the physical, mental health, and social needs people experience during pregnancy.
Model Overview
Up to 15 participating state Medicaid agencies (SMAs) will receive as much as $17 million over the 10-year period to develop a value-based alternative payment model for maternity care services, with the intention of improving quality and health outcomes and promoting the long-term sustainability of services. TMaH will focus on three pillars:
- Access to care, infrastructure, and workforce capacity
- Quality improvement and safety
- Whole-person care delivery
The TMaH model is designed to support birthing persons along their care journey, expanding continuity, and improving outcomes.
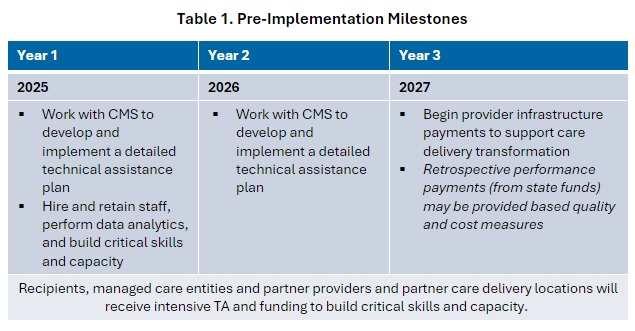
During the model’s first three years, states will receive targeted technical assistance to achieve pre-implementation milestones. The table below highlights the key activities in the pre-implementation phase.
Following pre-implementation, participants will enter a seven-year implementation period during which the SMAs will implement the program with partners, such as managed care organizations (MCOs), perinatal quality collaboratives, hospitals, birth centers, health centers and rural health clinics, maternity care providers, and community-based organizations.
In year four, states will offer partnering providers and care delivery sites upside-only performance payments from state funds (no cooperative funds may be used). In year five, states will transition partner provider and partner care delivery locations to a new value-based payment model. CMS will lead the development of the value-based model, and it will be finalized during the pre-implementation period.
The model also requires a health equity plan, which has been a consistent requirement across models from the Innovation Center. Awardees must develop a plan that addresses disparities among underserved populations, such as racial and ethnic groups and people living in rural areas, who are at higher risk for poor maternal outcomes.
State Medicaid Agency Requirements
For states considering TMaH, the NOFO outlines the requirements for participating SMAs, which include:
- States must include CHIP if pregnant people receive services through CHIP
- States that have managed care plans must contract with at least MCO for implementation
- Collaborate with partner providers (e.g., OBs, midwives, doulas), care delivery location (e.g., hospitals, birth centers, federally qualified health centers), and partner organizations
- Collaborate in the process to create cost and quality benchmarks with CMS
- Be actively involved in technical assistance activities, including attending regularly scheduled calls, providing input and working on portions of documents as appropriate
- Execute the data-sharing agreements necessary to support the exchange of data and information related to the TA activities and completion of milestones
- Provide CMS and contractors the necessary information and data to support the development of documents to help reach milestones
- States must demonstrate their ability to meet these requirements as part of the NOFO process, and CMS will evaluate their responses as part of the selection process
TMaH Opportunities and Considerations
The model offers states resources and technical assistance to develop value-based alternative payment models to support whole-person pregnancy, birth, and postpartum care and improved outcomes. Many SMAs already are working on programs to innovate care and payment, and the TMaH is an opportunity to expand and accelerate those programs.
The model offers an opportunity for states that have yet to expand postpartum coverage or added doula benefits to adopt these policies with the funding and technical assistance they may need to support their efforts.
SMAs interested in this opportunity should evaluate their application readiness and pre-plan for the application.
What’s Next?
States interested in TMaH should submit a letter of intent by August 8, 2024. Applications are due by September 20, 2024, and the model is expected to start January 2025.
The Health Management Associates team will continue to evaluate the TMaH model as more information becomes available. For more information, contact our featured experts below.
Unwinding recent Supreme Court rulings: impact on healthcare and beyond
This week, our In Focus section provides an initial overview of recent US Supreme Court rulings that reshape the landscape of national healthcare policy and operations. These decisions, ranging from redefining federal agency powers to addressing local ordinances that will affect people who are unhoused, are poised to have far-reaching implications across the federal and state governments.
The Decisions
A significant ruling came on June 29, 2024, with the Court overturning the precedent established in the 1984 Chevron v. Natural Resources Defense Council ruling. This year’s decision in Loper Bright Enterprises v. Raimondo marks a pivotal shift by eliminating the deference traditionally granted to federal agencies’ interpretations of ambiguous statutes. By empowering courts to clarify vague legislation, the ruling raises fundamental questions about the future of existing regulations and may lead to a surge in litigation challenging federal agency interpretations. The Court did state this ruling would have no impact on past decisions regarding the Chevron doctrine. The decision would apply only to current, pending, and future cases. When read in conjunction with the “major questions doctrine” announced in 2022 in West Virginia v. Environmental Protection Administration, agencies now face more challenges to regulations under a legal structure that does not provide deference to the agency.
The Court in Corner Post, Inc. v. Board of Governors of the Federal Reserve System also significantly reduced the ability of agencies to rely on statutes of limitations to avoid challenges to older regulations.
In a separate ruling that garnered attention, the Supreme Court upheld local ordinances in Grants Pass, OR, that restrict individuals experiencing homelessness from using blankets, pillows, or cardboard boxes for shelter in public spaces. The majority opinion in City of Grants Pass, Oregon v. Johnson supported the city’s stance that these ordinances, aimed at prohibiting camping on public property, do not constitute cruel and unusual punishment under the Constitution. This decision has sparked considerable debate over the balance between municipal governance and constitutional protections for people who are unhoused.
Also portending effects for the healthcare industry is the Court’s decision that defendants facing civil monetary penalties from the US Securities and Exchange Commission have a right to a jury trial. The Securities and Exchange Commission v. Jarkesy decision presents new considerations for healthcare and life sciences companies facing civil monetary penalties from the US Department of Health and Human Services.
What’s Next
The implications of these rulings are poised to reverberate throughout both federal and state governments. Stakeholders across healthcare and beyond must prepare for a period of adjustment and adaptation. Numerous questions regarding implementation and enforcement will likely emerge. The outcomes could trigger a wave of legal challenges and legislative responses as stakeholders navigate the evolving regulatory landscape.
Future In Focus sections will dive deeper into the potential impacts these decisions will have on healthcare policies and partnerships with related sectors. These insights will be pivotal in guiding strategic decisions amid the evolving legal framework.


Economic Analysis of Opioid Use Disorder in the Medicare Fee-for Service Program
This report quantifies the economic impact of opioid use disorder (OUD) specific to the Medicare fee-for-service (FFS) program, which covers approximately 51.6 percent of Medicare beneficiaries. We find that the cost to Medicare for managing these newly diagnosed patients was $29,669 more per patient than the propensity-matched control patients without OUD in 2022. We thus estimate that newly diagnosed OUD patients cost the Medicare program $4.3 billion in 2022. If these incident patient results were extrapolated into a 10-year budgetary impact analysis and if we assume constant rates of OUD incidence in the Medicare population, we estimate that the 10-year impact of OUD to the Medicare program would be $62.56 billion.
Our analysis demonstrates that OUD results in significant Medicare spending, including rising costs to beneficiaries through copayments and increased premiums. Additional work may be needed to determine whether the cost differential for incident patients with OUD generalizes to prevalent OUD patients as well. Though the 10-year budgetary impact figures require extrapolation and assumptions about future OUD use, they illustrate for policymakers the size of the fiscal challenge created by OUD in the Medicare population.