
May 1, 2024
Medicaid Unwinding Check-in: Data Informed Observations to Guide Future Action
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
Medicaid Unwinding Check-in: Data Informed Observations to Guide Future Action

More than 100,000 people in the United States die every year from drug overdoses, driven by the availability of illicitly manufactured fentanyl. On March 19, 2024, HMA held the Compassionate Overdose Response Summit to discuss overdose response and reversal drugs like naloxone in the context of a fluctuating drug supply. Forty experts participated in consensus-building discussion on a standard of care opioid overdose response protocol. Throughout four panel presentations, a critical message emerged: those responding to an overdose should aim to restore breathing without causing withdrawal by supporting the person’s breathing, giving low or standard doses of naloxone (0.4 mg intramuscular injection and <4 mg intranasal spray) until spontaneous breathing is restored, and creating a calm environment. Despite fluctuations in the drug supply, standard dose naloxone is effective.
The standard dose of naloxone is considered 0.4 mg intramuscular injection and <4 mg intranasal spray. It is extremely effective and preferred by people who experience overdose. Reports at the Summit from four states (Missouri, Kentucky, Pennsylvania, and New York) made clear that an increase in naloxone dose is not a necessary response to the presence of fentanyl in the drug supply. Negative reactions following naloxone administration may be avoided, and anger can potentially be managed via low-dose naloxone titration and a calm, compassionate, and considerate communication style between the person who overdosed, the person who administered an opioid antagonist, and bystanders, including EMS.
Another key takeaway from the Summit, and shared in the report released today, was the acute and long-term adverse outcomes of withdrawal on people who experience overdose. The way a person is treated during an overdose, i.e., the communication style of the responder, likelihood of withdrawal, and the care they are offered after, affects their risk behavior such as using more opioids to feel better. In a study from New York State, those who received 8 mg nasal spray were more likely to experience withdrawal than those who received 4 mg nasal spray. People who experience withdrawal after an overdose may be discouraged from seeking help in the future.
“A compassionate overdose response is looking at the entire person. It’s not that moment of reviving them. It’s [also] what happens afterward.” – Joy Rucker, Summit Panelist
The findings shared at the Summit are timely given the availability of high-dose and long-acting overdose reversal products in the US. The FDA continues to ignore the life-threatening side-effects of high-dose products and recently approved a 10 mg nasal spray. This trend has drawn concern from addiction medicine providers, emergency medical services, toxicologists, harm reductionists and people who experience overdose alike. Standard dose products are available at the lowest cost for bulk purchase and decades of research show their use in the community reduces overdose mortality. A chart with currently available opioid overdose reversal products is available at PrescribetoPrevent.org.
To learn more about compassionate overdose response and the significance of overdose reversal product selection, listen to the event proceedings and read the report below. View the webinar replay with links to download PDFs of speakers’ presentations.
Contact Erin Russell to discuss the policy and program implications of the Summit’s findings.
The Compassionate Overdose Summit was presented with support from HMA, Harm Reduction Therapeutics, Vital Strategies, the Bloomberg American Health Initiative, and the University of Pittsburgh Graduate School of Public Health. Funds were used to secure event space and speaker stipends to cover their time and travel needs, hotels, meals, AV equipment, and event staffing.

This webinar was held on May 1, 2024
The final webinar of this three-part series emphasized the importance of a comprehensive and interconnected spectrum of engagement and treatment strategies. To truly build and maintain a substance use disorder (SUD) ecosystem with accountability across the system and ‘no wrong door,’ best practices must embrace a systems-thinking approach. An interconnected system requires building strong partnerships across the SUD ecosystem and engagement and treatment strategies will focus on leveraging those partnerships to facilitate engagement of individuals throughout the system.
Learning objectives included discussing approaches to system alignment that emphasize impact and ensure individuals remain engaged no matter where they are in their SUD journey and how to describe a comprehensive approach to systems thinking that builds accountable relationships and partnerships to ensure that the system has no wrong doors for engagement of individuals throughout the system.
THE CLIENT
The New Mexico Office of the Superintendent of Insurance (OSI) was directed by its state legislature to explore hospital global revenue budgets and other innovative hospital payment models over several years, and to explore key elements of affordability and accessibility of coverage and care, including hospital global budgeting.
BACKGROUND
OSI contracted with Health Management Associates (HMA) to build on previous hospital global budgeting research and provide technical assistance in resolving the complex issues surrounding global budgeting, including development of a potential global budget payment model framework. The contract also called for HMA to prepare an implementation framework that involves stakeholder engagement, including a plan for engagement with the Centers for Medicare and Medicaid Services (CMS) Innovation Center and to identify key administrative and data challenges.
APPROACH
HMA divided the project’s scope into two phases:
Phase 1:
Develop preliminary policy and model options, including submission of two deliverables:
Phase 2:
Refine the hospital global budgeting model based on OSI’s input on the Hospital Global Budget Options Paper and develop and submit three additional reports:
TESTIMONIAL
“Beginning with a solid proposal, HMA built on previous research conducted on New Mexico and other states’ experiences, evaluated options, highlighted administrative and data needs to produce a comprehensive study and an implementation action plan. The team exhibited superb professionalism and attention to high quality work.”
Sahar Hassanin, Senior Economist, OSI, NM
RESULTS
HMA developed an overview of principles and global budgeting models developed by other states, policy options, recommendations for how to work with CMS, a blueprint for stakeholder engagement, and an assessment of data needs and challenges. The proposed hospital global budget payment model was informed by the HMA team’s expertise and research on three states’ experience with CMS Innovation Center payment models (Maryland, Pennsylvania, and Vermont). The five public reports can be found at Healthcare Affordability and Accessibility Research Projects. These reports detail a plan for budgeting and governance that will enable the creation of a value-based payment system that supports a delivery system in which hospitals provide services that their communities need, rather than focus on the services most likely to merely enhance revenue. Through leadership and innovation, the state can help ensure a sustainable provider network is available to deliver high-quality and efficient care to all New Mexicans.
HMA can help other states and organizations with financial and strategic planning to optimize value-based care, budgeting, affordability, and accessibility for beneficiaries of publicly-funded healthcare programs.

Our second In Focus section reviews the policy changes proposed by the Centers for Medicare & Medicaid Services (CMS) on April 10, 2024, for the Fiscal Year (FY) 2025 Medicare Hospital Inpatient Prospective Payment System (IPPS) and Long-Term Acute Care Hospital (LTCH) Proposed Rule (CMS-1808-P). This year’s IPPS Proposed Rule includes several policy changes that will alter hospital margins and change administrative procedures, beginning as soon as October 1, 2024.
We highlight five proposed policies that are likely to have the greatest impact on Medicare beneficiaries, hospitals and health systems, payors, and manufacturers:
Stakeholders have until June 10, 2024, to submit comments to CMS on the contents of this regulation and request for information.
Market Basket Update
Proposed rule: Overall CMS’s Medicare 2025 Hospital Inpatient Proposed Rule will increase payments to acute care hospitals by an estimated $3.2 billion in 2024−2025; however, recent trends in economy-wide inflation may alter this estimate by the time the agency releases the final regulation in August 2024.
HMA/Moran analysis: CMS’s 2.6 percent increase is based largely on an estimate of the rate of increase in the cost of a standard basket of hospital goods—the hospital market basket. For beneficiaries, this payment rate increase will lead to a higher standard Medicare inpatient deductible and increase out-of-pocket costs. For hospitals and health systems, payors, and manufacturers the proposed payment increase (2.6%) falls below economywide inflation over the past year (3.5%) and below what Medicare Advantage plans will receive for 2025 (3.7%).1,2 Importantly, based on our expertise with the calculation of the hospital market basket, we anticipate the proposed 2.6 percent increase will increase slightly by the time rates are finalized later this year.
New Technology Add-on Payments (NTAPs)
Proposed Rule: CMS proposes three changes to the NTAP program and discusses NTAP applications for FY 2025:
HMA/Moran Analysis: The first two proposed changes are in response to concerns about more restrictive application requirements finalized last year. When CMS shifted the FDA approval deadline to May 1 last year, commenters noted that fewer products would be eligible to receive NTAPs in their third year of the newness period. Allowing all products with a third anniversary that falls within a fiscal year (rather than only those with expirations in the second half of the fiscal year) to receive NTAPs narrowly addresses this concern. More products will qualify for NTAPs during their third year of newness, but that does not necessarily mean that more products will receive three years of NTAPs.
The second proposal tweaks last year’s change requiring a “complete and active” FDA application at the time an NTAP application is submitted to ensure that NTAP applications were far enough along in the FDA review process that information about the product would be available to the public and for CMS staff review. CMS proposal acknowledges that the original bright line rule may have inappropriately excluded potential applicants.
Finally, CMS’s proposal to increase the NTAP percentage for gene therapies treating sickle cell disease aligns with the Cell and Gene Therapy Access Model’s focus on sickle cell therapies. Of note, CMS seeks comment on whether the increased NTAP percentage should be applied only to applicants that have entered value-based purchasing agreements or are “otherwise engaging in behaviors that promote access to these therapies at lower cost.” CMS seems willing to increase NTAP payments in limited situations to boost selected policy goals, but the proposals in this regulation do not represent widespread NTAP payment increases.
Transforming Episode Accountability Model (TEAM)
Proposed Rule: CMS proposes to establish a new mandatory episode-based CMS Innovation Center model, Transforming Episode Accountability Model (TEAM). In the TEAM model, selected acute care hospitals would coordinate care for people with traditional Medicare who undergo one of the five specified surgical procedures:
Hospitals in the model will assume responsibility for the cost and quality of care from surgery through the first 30 days after the Medicare beneficiary leaves the hospital. Hospitals also must refer patients to primary care services to support optimal long-term health outcomes.
In a first of its kind program, CMS has created a voluntary decarbonization and resilience initiative through which participating hospitals can report metrics related to greenhouse gas emissions to CMS. CMS will provide individualized feedback reports and public recognition of participation and potential performance in the initiative.
HMA/Moran Analysis: The critical aspect of the TEAM model that stakeholders need to understand is that it will be mandatory. TEAM will begin in 2026 and continue for five years. The TEAM model builds on and combines previous models such as the Bundled Payment for Care Improvement (BPCI) model and the Comprehensive Care for Joint Replacement (CJR) model. Hospitals will be required to report various quality measures, and payment will be based on spending targets and include retroactive reconciliation. TEAM also seeks to integrate specialty and primary care. The model complements existing accountable care organization (ACO) models such as ACO REACH or the Medicare Shared Savings Program as beneficiaries would be able to be assigned to both TEAM and ACO programs.
Hospital Wage Index Adjustments and Labor Market Changes:
Proposed Rule: CMS proposes two wage index policies for FY 2025. First, CMS proposes to extend the temporary policy finalized in the FY 2020 IPPS/LTCH PPS final rule for three additional years to address wage index disparities affecting low-wage index hospitals, which includes many rural hospitals. Second, as required by law, CMS proposes to revise the labor market areas used for the wage index based on the most recent core-based statistical area delineations issued by the Office of Management and Budget (OMB) based on 2020 Census data.
HMA/Moran analysis: The two wage index policies that CMS proposes for FY 2025 will have important positive and potentially negative consequences for hospital payment. The policy to extend the low-wage index policy for three additional years will allow many hospitals with low wage indexes to increase their wage index and their payment rates across all MS-DRGs. This policy will bring millions of additional dollars to rural hospitals in FY 2025.
The second policy is a statutorily required update to the labor markets used to establish CMS’s hospital wage indexes. CMS will redefine 53 counties from urban to rural and 54 counties from rural to urban, which will disrupt various hospital payment policies for hospitals in the affected counties. The overall impact of both proposed geographic policy changes for FY 2025 will be to increase inpatient payment rates for rural hospitals.
Revision to Housing-Related Diagnosis Coding
Proposed Rule: CMS proposes to change the severity designation of the seven ICD-10-CM diagnosis codes that describe inadequate housing and housing instability from non-complication or comorbidity (non-CC) to complication or comorbidity (CC).
HMA/Moran Analysis: In proposing this change, CMS is building on its previous policy of including diagnosis codes for describing when a beneficiary is homeless (e.g., unspecified, sheltered, unsheltered). Importantly, this new policy proposal will enable hospitals to be paid higher inpatient payment rates when patients with inadequate or unstable housing are served. Specifically, this proposal would result in cases involving patients to whom these codes apply to be coded in a higher-level MS-DRG within a given family of MS-DRG codes. If finalized, this change in coding policy will result in higher payment rates for hospital patients who are experiencing housing insecurity.
Connect with Us
HMA’s Medicare Practice Group, including consultants from The Moran Company, works to monitor legislative and regulatory developments in the inpatient hospital space and to assess the impact of inpatient payment, quality, and policy changes on the hospital sector. Our Medicare experts interpret and model inpatient policy proposals and use these analyses to assist clients in developing their strategic plans and commenting on proposed regulations. We replicate the methodologies CMS uses in setting hospital payments and model alternative payment policies using the most current Medicare (100%) claims data. We assist clients with modeling for DRG reassignment requests and to support NTAP applications. We also support clients in analyzing CMS Innovation Center alternative payment models.
For more information or questions about the policies described above, contact our featured experts.
This week, our In Focus section reviews significant Medicaid policy announcements from the Centers for Medicare & Medicaid Services (CMS). For example, both the Medicaid and Children’s Health Insurance Program Managed Care Access, Finance, and Quality Final Rule (CMS-2439-F) (view the CMS fact sheet available) and the separate Ensuring Access to Medicaid Services Final Rule (CMS-2442-F) (view the CMS fact sheet) were released April 22, 2024.
Taken together, these two final rules create new flexibilities and requirements aimed at enhancing accountability for improving access and quality in Medicaid and the Children’s Health Insurance Program (CHIP) across the fee-for-service and managed care delivery systems and provide targeted regulatory flexibility in support of this goal.
HMA’s April 11, 2024, “What to Watch For” article outlined several proposed changes that CMS was poised to advance in the Medicaid managed care program. We focus today on the approved changes, including:
Following are HMA’s insights on the key takeaways in each of these major areas for states, managed care organizations (MCOs), providers, and other stakeholders. In addition, HMA experts will discuss the final rule during a LinkedIn Live on event at 2:00 pm (EDT) April 25, 2024. Go to the HMA LinkedIn feed to watch.
In future weeks, HMA will review the Ensuring Access to Care final rule.
ILOSs
The final rule makes clear that CMS remains committed to the conviction that ILOSs can play an important role in supporting state and MCO efforts to address many of the unmet physical, behavioral, developmental, long-term care, and other enrollee needs. At the same time, CMS continues to put forward requirements in this area to ensure adequate assessment of these substitute services and settings in advance of approval, ongoing monitoring for sufficient beneficiary protections, and financial accountability for related expenditures.
The final rule presents an opportunity to leverage ILOSs to improve population health, reduce health inequities, and lower total healthcare costs in Medicaid and CHIP, including by addressing unmet health-related social needs as well as through other avenues. To take full advantage of this opportunity, states and MCOs must ensure that that they are prepared to meet the accountability measures outlined in the final rule and partner with existing providers and community-based organizations that already provide such services and settings.
Medicaid and CHIP Quality Rating System
CMS finalized most proposed provisions related to mandatory quality measures, the process used to update these measures, the ability of states to include additional measures, and the ability of states to apply an alternative QRS if desired. On this last point, CMS is making several modifications to its MAC QRS proposal to clarify the scope of and to reduce the implementation resources needed for an alternative MAC QRS if a state elects to implement one.
States will be required to collect from MCOs the data necessary to calculate ratings for each measure and ensure that all data collected are validated. This will require MCOs to assess their capability to produce the mandated data upon request by states and, to the extent possible, to assess baseline performance on measures and proactively operationalize strategies to improve performance where necessary.
Medical Loss Ratios
The final rule aligns Medicaid and CHIP MLR QIA reporting requirements with the private market to ensure that only those expenses that are directly related to healthcare QIAs are included in the MLR numerator. CMS notes that this provision will allow for better MLR data comparisons between the private market and Medicaid and CHIP markets as well as reduce administrative burden for MCOs participating across these markets.
MCOs will need to model the impact of QIA expenditures that are no longer available for inclusion in the MLR numerator to ensure that a resulting failure to meet any minimum MLR requirements can be avoided, and, if it is projected to occur, a strategy can be developed and executed to avert the problem. CMS made this requirement effective as of the effective date of the final rule with no delay because it believes it is critical to the fiscal integrity of Medicaid and CHIP, adding urgency to MCO compliance action here.
Network Adequacy
The final rule makes clear that CMS has been persuaded that it needs to increase oversight of network adequacy and overall access to care through a new quantitative network adequacy standard. To measure network adequacy, the agency intends to implement wait time standards, complemented by secret shopper surveys to support enforcement.
Wait time standards and secret shopper surveys present opportunities for states, MCOs, and providers to collaborate to enhance access where needed and ensure compliance with the final rule. Undertaking secret shopper surveys ahead of implementation of the wait time standards (effective the first rating period beginning on or after three years after the effective date of the final rule) to determine the current performance relative to maximum wait times is a proactive step that is worth consideration by states and MCOs and can also be employed to foster dialogue with providers to address any areas of concern identified.
State Directed Payments
CMS is adopting its proposal in the final rule to use the average commercial rate as a limit for SDPs for inpatient and outpatient hospital services, nursing facility services, and professional services at academic medical centers. CMS believes that this approach represents a reasonable limit that is supportive of appropriate fiscal guardrails, while still affording states the flexibility to achieve SDP policy goals. States and providers will need to account for this requirement, along with others, as SDPs are developed going forward.
Connect with Us
HMA is ready to support your efforts to understand and take action to account for the managed care final rule’s effects on your state or organization’s strategy and operations. Please reach out to [email protected] to connect with our expert team members on this vital set of issues.

Tim Murray is a principal and senior consulting actuary of Wakely Consulting Group, an HMA Company. With over two decades of experience as a health actuary, Tim illuminates the challenges and opportunities within Medicare, particularly focusing on value assessment and the pivotal role of data collection. Digging into the complexities of Medicare Advantage, he discusses predictive modeling, innovative supplemental benefits, and the need for structured data metrics to drive sustainable healthcare solutions.
This week, our second In Focus explores a new Issue Brief published by Leavitt Partners, a Health Management Associates, Inc. (HMA) Company, which addresses the February 21, 2024, cyberattack on Change Healthcare. The cyberattack is one of the most significant on the healthcare industry and has had short-term effects on the entire healthcare sector, with potential for longer-term impacts across the industry.
Because of the ransomware attack, more than 100 applications were taken offline, preventing medical professionals from conducting out many patient-facing activities, including filling prescriptions, managing care plans, and performing prior authorization checks. Six weeks after the crippling cyberattack on Change Healthcare, some systems are still only partially operational and many claims remain unpaid. This situation has disrupted patient access to care and placed significant financial strain on providers.
Change Healthcare is maintaining a daily status report on operations on their website. In addition, the Department of Health and Human Services (HHS) provided the following resource to the healthcare provider community to work with payers directly.
With billions of dollars in loans and advance payments already disbursed and ongoing investigations into Health Insurance Portability and Accountability Act (HIPAA) violations, the healthcare industry is bracing for long-term impact, while the Administration and Congress are just beginning to act. Leavitt Partners experts, an HMA Company, is monitoring and analyzing the impacts on payers and providers, as well as current and future policy implications.
For more information and to obtain in-depth issue briefs, including “Cyberattacks: Health Care Industry Impacts and the Federal Response,” contact our featured experts.
This week, our In Focus section reviews recent Medicaid enrollment trends in capitated, risk-based managed care in 30 states.1 Many state Medicaid agencies post monthly enrollment figures by health plan for their Medicaid managed care population on their websites. These data allow for timely analysis of enrollment trends across states and managed care organizations. All 30 states highlighted in this review have released monthly Medicaid managed care enrollment data into quarter four (Q4) of 2023. The analysis that follows reflects the most recent data posted. HMA continues tracking enrollment as states work towards concluding their Public Health Emergency (PHE) unwinding-related redeterminations and resuming normal eligibility operations.
Health Management Associates, Inc., (HMA) has reviewed the Q4 enrollment data (see Table 1) and offers the following observations:
Table 1. Monthly MCO Enrollment by State, October 2023−December 2023
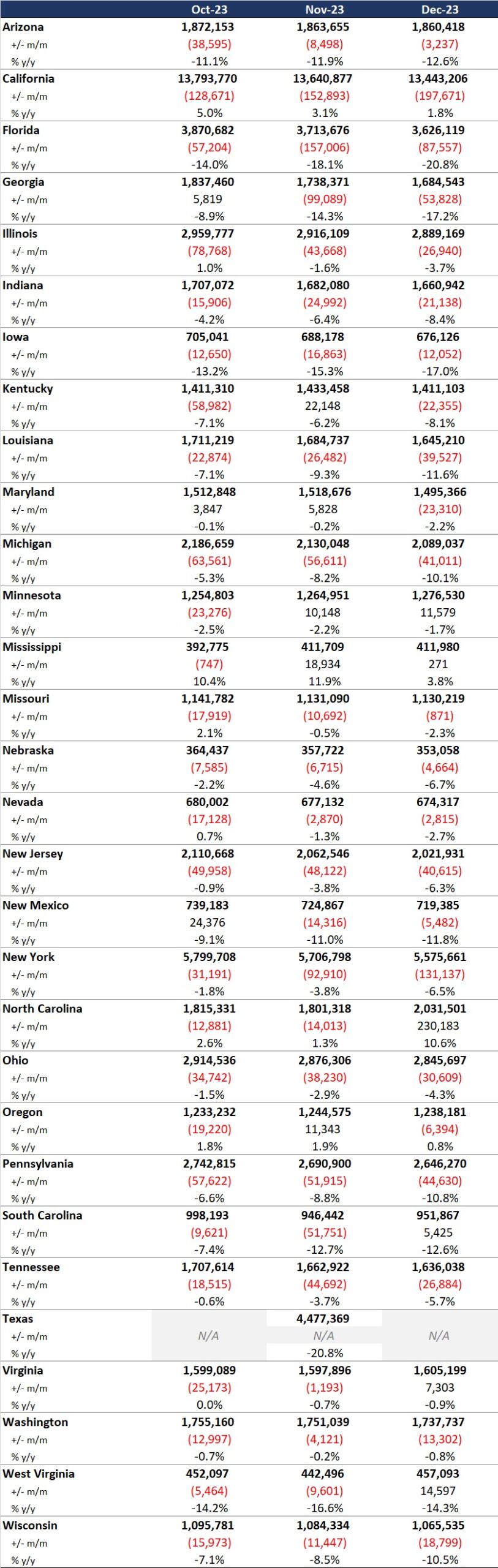
It is important to note the limitations of the data presented. First, not all states report the data at the same time during the month. Some of these figures reflect beginning of the month totals, whereas others provide an end of the month snapshot. Second, in some cases the data are comprehensive in that they cover all state-sponsored health programs offering managed care; in other cases, the data reflect only a subset of the broader managed Medicaid population, making it the key limitation to comparing the data described below and figures that publicly traded Medicaid MCOs report. Consequently, the data in Table 1 should be viewed as a sampling of enrollment trends across these states rather than a comprehensive comparison, which cannot be developed based on publicly available monthly enrollment information.
Expand Your Awareness about Medicaid and Medicare Advantage via HMAIS
If you are interested in gaining access to detailed information on the Medicaid managed care landscape, an HMAIS subscription is the key to unlock important data. The HMA Information Services (HMAIS) collects Medicaid and Medicare Advantage Special Needs Plan (SNP) enrollment data, health plan financials, as well as developments on expansions, waivers, and demonstrations. Your HMAIS login also provides access to a library of public documents all in one place, including Medicaid RFPs, responses, model contracts, scoring sheets and other procurement related materials. HMAIS combines this publicly available information along with HMA expert insights on the structure of Medicaid in each state, as well as a proprietary HMA Medicaid Managed Care Opportunity Assessment.
For information on how to subscribe to HMA Information Services, contact our featured experts.
Health Management Associates’ CEO Douglas Elwell Retiring; COO Charles (Chuck) Milligan to Lead Firm
