HMA is pleased to welcome new experts to our family of companies in April 2023. This diverse team brings significant expertise in Medicare, Medicaid, regulatory strategies, and managed care, strengthening HMA’s capabilities in healthcare consulting across areas like actuarial support, regulatory compliance, and strategic leadership in Medicare Advantage and Medicaid programs.
COVID-19 Resources & Support





The end of the public health emergency: imminent changes to the coverage of virtual care services
Policy crossroads and the end of the public health emergency due to COVID-19
This is part of a three-part series on significant implications of the end of the Public Health Emergency (PHE).
The end of the Public Health Emergency on May 11, 2023 is likely to mark a transitional point in the rapidly evolving arena of virtual care services and not a dramatic end of coverage. Coverage of virtual care services will continue to evolve significantly over the next five years given the exponential growth in the public’s awareness of, and comfort with, these services — all hastened by the COVID-19 Federal Public Health Emergency.
The U.S. Congress and the Centers for Medicare and Medicaid Services (CMS) used its authority during the PHE to significantly expand Medicare coverage for virtual care services, covering telehealth visits in urban areas and from patient’s homes. In addition, Medicare began covering a wide range of clinical services virtually such as behavioral health and physical therapy; it also expanded coverage for different service delivery modalities to include audio-only visits. As a result of the changes, Medicare became a leading payer for virtual care nationally between 2020 and 2022. Over this same period, private insurers and state Medicaid programs largely followed Medicare’s lead by expanding their own virtual care coverage.
One of the consequences of the PHE is that most payers have embraced Medicare’s basic definitional structure for types of virtual care services. As a part of this typology, virtual care services are divided into two general buckets of services: telehealth visits (physician office visits conducted via audio and video technology), which are typically prohibited by statute in urban areas or a patient’s home; and Communication Technology-Based Services (CTBS) which can be conducted anywhere. CTBSs include: remote patient monitoring (RPM); virtual check-ins (brief patient-to-clinician exchanges); e-visits (online portal or email visits); and e-consults (clinician to clinician interaction).
With the end of the PHE on May 11, Medicare coverage of virtual care services and coverage offered by other payers will change. The details and scope of this change have many stakeholders concerned and confused. HMA has a keen sense for which virtual care services may get a new lease on life in the coming months and which are likely to be hotly debated in the years ahead. The one certainty is that the last 3 years have altered the landscape for virtual care services for years to come.
Shift in Virtual Care Landscape
As a result of the statutory geographic limitations and restrictions placed on traditional fee-for-service (FFS) Medicare coverage, use of telehealth services was minimal most of the last decade, with only one-quarter of 1 percent (0.25%) of beneficiaries in FFS Medicare using virtual care services.[1] Even among Medicare Advantage plans and Medicare Accountable Care Organizations (ACOs), neither of which which face the same restrictions, virtual care was utilized very rarely before 2019.
This sluggish use of telehealth was radically altered when HHS used its PHE authority to relax constraints on the use of use virtual care services by Medicare beneficiaries and providers.[2],[3] Among the most consequential changes made by policymakers at the outset of the PHE were:
- Enabling telehealth services to be provided anywhere (e.g., urban areas and patients’ homes);
- Allowing Federally Qualified Health Centers (FQHC) and Rural Health Clinics (RHC) to conduct virtual care services;
- Granting various types of clinicians permission to deliver virtual care services;
- Enabling new patients to receive virtual care services;
- Authorizing audio-only services;
- Permitting telehealth services for more than 200 different types of clinical services (e.g., mental health, emergency department, physical and occupational therapy, critical care, inpatient care);
- Relaxing HIPPA rules to enable the broad use of smartphones for virtual care.
Due to these policy changes, rates of virtual care skyrocketed during the PHE (Figure 1). In April of 2020 the number of Medicare claims for any type of virtual care service exceeded 9 million, while 2019 the number of these services provided monthly never exceeded 100,000 (Figure 1). On an annual basis, from 2019 to 2021 the number of virtual care visits jumped from roughly 1 million to 39 million and the number of unique beneficiaries receiving these services increased from 300,000 to nearly 12 million.
Figure 1: Number of Virtual Care Service Visits, Number of Unique Medicare Fee-For-Service Beneficiaries, and Number of visits per Utilizer by Month, December 2019 to December 2021.

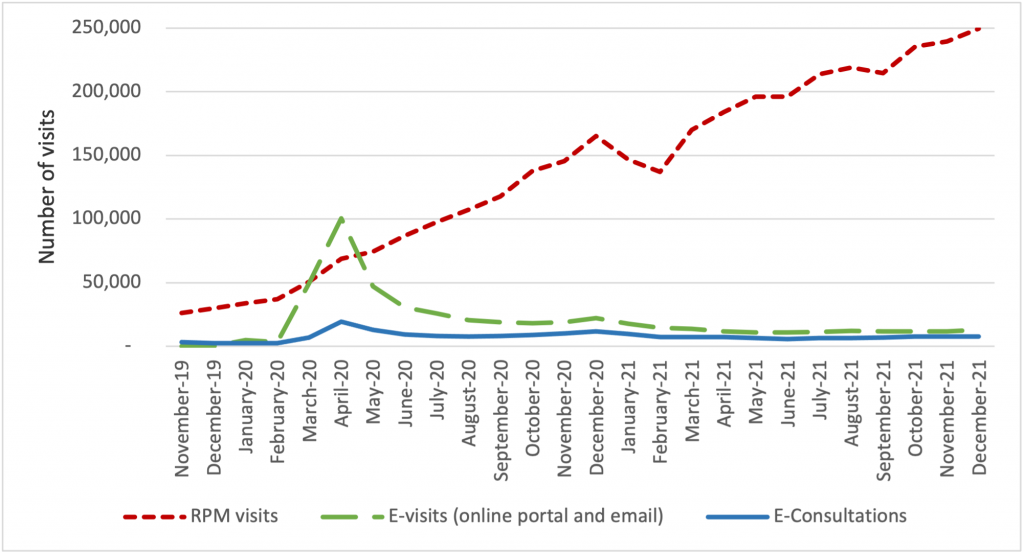
The growth of virtual care services has largely been driven by an increase in telehealth visits, but we observe important trends in the use of CTBSs, as well. In late 2021, more than 90 percent of visits were associated with telehealth, while 10 percent were associated with CTBSs. Early in the PHE, all of these service types experienced an initial, abrupt increase in use (Figure 2). By contrast, the growth in the use of remote patient monitoring (RPM) has been continuous since 2020. The growth in use of RPM reflects the general movement of services into patients’ homes and has been accelerated by specialist such as cardiologists and endocrinologists beginning to leverage the power of RPM. We expect greater diffusion and use of RPM and other CTBSs in the next five years.
Figure 2: Number of Virtual Care Service Visits for Remote Patient Monitoring, Virtual Check-ins, E-visits, and E-Consultations by Month, December 2019 to December 2021.
Policies temporarily in place until the end of 2024
During the PHE, Congress made critical long-term changes to Medicare’s coverage of virtual care services that continued to spur the use of these services and offer access to care for beneficiaries. In 2021, Congress changed the law to permanently allow Medicare beneficiaries to receive behavioral/mental telehealth services regardless of location (urban or rural) and for this care to be available to patients in their own homes.
In 2022, Congress severed the link between the PHE declaration and Medicare coverage policies for virtual care services, extending those benefits through the end of calendar year 2024. We expect that coverage for all telehealth services will receive considerable attention from federal policymakers and stakeholders towards the end of 2024.
Immediate impact of expiring policies
Certain aspects of Medicare’s virtual care policies will, however, terminate May 11, 2023, when the PHE declaration comes to an end. Several of the expiring policies have a broader impact beyond the Medicare program, affecting patients insured by private payers and State Medicaid programs.
Specifically, when the PHE ends, policymakers will need to address the following anticipated changes:
- The Office for Civil Rights (OCR) will return to imposing penalties on providers who violate the provisions of the Health Insurance Portability and Accountability Act (HIPAA) by using public-facing remote communication technologies which are not HIPAA-compliant. This may prohibit the use of some of the most common smartphone-based video conferencing tools for health care visits.
- Medicare beneficiaries without an existing relationship with a clinician will be unable to receive CTBSs such as RPM, virtual check-ins, and e-visits.
- Providers will no longer be allowed to provide virtual care services across state lines, because most state medical licensure boards will return to pre-PHE policy.
- Federal rules from the Drug Enforcement Agency (DEA) may revert to the pre-PHE requirement that clinicians establish a patient-provider relationship in-person before being permitted to prescribe controlled substances for substance use disorder treatment.
Potential policy changes occurring before 2025 As explained earlier, Medicare coverage for many virtual care services will remain in place for the next 19 months. Before the end of 2024, Congress will need to address several policy questions, and among the most widely debated are whether to:
- Restore Medicare’s statutory prohibition on telehealth services being delivered in urban areas or in home settings;
- Allow Federally Qualified Health Centers and Rural Health Clinics to provide telehealth services to Medicare beneficiaries; or
- Continue to cover audio-only telehealth visits under Medicare.
Lawmakers will look to payers, patients, and providers for feedback before making these policy decisions. Among the most critical pieces of information they will also consider will be the results of the study Congress has required of HHS regarding trends in the use of virtual care. This study’s final report is due in 2026, which has led some to speculate that Congress will delay action on virtual care coverage policy until then. In the meanwhile, we expect HHS will be assessing the overall volume of virtual care use, who is using which types of services, and the levels of related fraud and abuse.
Looking Ahead
In the United States, our experience during the acute phase of the pandemic demonstrated that patients and providers are more receptive than previously thought to utilizing digital technologies for the delivery of care. This experience may also influence policymakers’ decisions about reimbursement and coverage of wearable devices, as well as other cutting-edge tools that rely on artificial intelligence or machine learning.
HMA believes payers and providers alike can take steps now to strategically prepare for the still evolving and growing landscape of digital health care.
Based on the various changes that have occurred in the virtual care environment over the last 3 years, we are intently watching several areas of potential change in the practice of medicine and the ways payers set coverage policy. Below are some of the trends we anticipate in the years ahead:
- Continued use of virtual care services at levels observed in 2021.
- An expansion of CMS’s programs to protect against fraud and abuse related to virtual care.
- Notable growth in the use of RPM, and related services for physical and occupational therapy services.
- The proliferation of innovative home-based screening and testing technologies. We anticipate payers will encourage the use of these at-home tests for things like kidney function, liver function, and colorectal cancer screening in order to limit care delivery in higher cost settings.
- Growth in “virtual-first” insurance plans, where patients are encouraged to use virtual care first – prior to being seen in person. As these plan options expand, we anticipate virtual care use will rise, and reimbursement rates will begin to change.
Virtual care services are primed for additional growth and HMA is working with a wide variety of payers, providers, and foundations to develop strategies for adapting to state and federal rules and regulations related to virtual care. Changes in this landscape will hinge on research CMS will complete by the end of 2026, and coverage decisions made by states and commercial payers. HMA is well positioned to assist stakeholders with work in this area and can leverage access to Medicare and Medicaid claims data to conduct health services research to illustrate geographic variations in the use of virtual care.
If you have questions on how HMA can support your agency before or after the end of the PHE, please contact our experts below.
Read other parts of this blog series:
[1] (2016) https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Information-on-Medicare-Telehealth-Report.pdf
[2] Centers for Medicare & Medicaid Services. Medicare telemedicine health care provider fact sheet. March 17, 2020. https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
[3] HHS Administration for Strategic Preparedness & Response (ASPR). https://aspr.hhs.gov/legal/PHE/Pages/default.aspx
Evaluating the delivery of virtual child welfare services
This week, our In Focus reviews a new Health Management Associates (HMA) report, highlighting hybrid (in-person & virtual visits) as the future of child welfare service delivery. During the COVID-19 public health emergency (PHE), the federal government waived the requirement for “once every 30 days” in-person visits by caseworkers for children in foster care, allowing these visits to occur virtually. In 2021, Casey Family Programs (CFP) commissioned HMA to evaluate the delivery of virtual child welfare services and outline the implications of the COVID-19 PHE on the child welfare system.
The report “Evaluating the Delivery of Virtual Child Welfare Services” is now available. It summarizes HMA’s findings and elevates the voices of staff in public and private child welfare agencies, and of youth and families with lived experiences, and examines their perspectives on how well virtual services have worked. It also details the implications of the COVID-19 PHE, the response from public child welfare agencies, and offers guidance on a hybrid (part in-person, part virtual) service model, which we believe will continue to be a factor in the future delivery of child welfare services.
As the COVID-19 PHE accelerated the spread and scale of telehealth adoption in health care, we surmised that the experience offered valuable opportunities to learn more about how the health care sector’s adoption of telehealth services could be applied in the child welfare community. While cognizant of the unique considerations for child welfare, this disruption also represents a substantial opportunity to rethink the child welfare system and advance both the use of technology as well as a more prevention- and strengths-based approach to child welfare.
The report highlights innovative approaches in the field, offers questions to frame a jurisdiction’s decision-making process, and provides a tool to facilitate an informed decision on the hybrid model. The report also offers a broader value proposition that outlines policy, practice, workforce, and technology imperatives to develop a hybrid approach to the delivery of child welfare services.
For questions, please contact our experts below.
HMA in Health Affairs Forefront: imminent VFC decisions are critical for RSV therapy access
As respiratory syncytial virus (RSV), a seasonal pathogen in young children is challenging the national health care system as part of an unprecedented “tripledemic” with COVID-19 and flu this winter, HMA authors weigh in on potential coverage pathways for new monoclonal antibody (mAb) preventive therapies for RSV and their implications for access.
The Vaccines for Children (VFC) program is a proven vehicle for ensuring comprehensive coverage of immunizations based on recommendations from the Advisory Committee on Immunization Practices (ACIP). An ACIP workgroup is actively discussing potential recommendations for immunization with RSV mAbs.
In the recent Health Affairs Forefront article, “Coverage By Vaccines For Children Program Is Critical For RSV Therapy Access,” HMA authors Helen DuPlessis, MD, FAAP, Diana Rodin, and Matt Wimmer explore the implications of ACIP recommendations, Medicaid coverage pathways, and children’s access to the new therapies.
Congress sets date for Medicaid “unwinding”: what now?
This week, our In Focus section reviews changes to Medicaid’s COVID-19 Public Health Emergency (PHE) unwinding. People enrolled in the Medicaid program have been continuously enrolled for almost three years, but that situation is about to change. In December 2022, Congress passed, and the President signed into law a massive compromise bill to fund the government. It includes an important change to Medicaid’s continuous enrollment policy, which has been in effect since the early days of the COVID-19 PHE in March 2020.
Congress passed the Families First Coronavirus Relief Act (FFCRA) in March 2020. This legislation has allowed states to receive a 6.2 percentage point increase in their federal matching rate for Medicaid. As a condition for receiving the enhanced funding, states have been prohibited from disenrolling individuals who were otherwise determined ineligible for Medicaid. As a result, nearly 20 million more people are now enrolled in the Medicaid program.
The 2023 spending bill severs the link between the COVID-19 PHE declaration, the continuous enrollment requirement, and the higher federal match rate. The new law:
- Ends the Medicaid continuous coverage policy on March 31, 2023, even if the PHE declaration remains in effect. States may begin issuing terminations of ineligible individuals as early as February 1, with an effective date of April 1.
- Phases down the 6.2 percentage point increase in the federal matching rate rather than ending it abruptly at the end of the PHE as required under the FFCRA. Specifically, the increase will drop to 5 percentage points in April−June 2023, 2.5 percentage points in July−September 2023, and 1.5 percentage points in October−December 2023.
- Does not end the PHE or other flexibilities linked to the PHE.
Congress also added new parameters and reporting requirements for states as they resume annual eligibility renewals with coverage cancellation for individuals who no longer qualify. These requirements are in addition to data the Centers for Medicare & Medicaid Services (CMS) previously directed states to report. For example:
- States must maintain up-to-date enrollee contact information for individuals who will undergo an eligibility redetermination.
- States cannot disenroll individuals based only on returned mail.
- Prior to disenrolling an individual, the state must make a “good faith effort” to contact the person using more than one communication mode.
- States must submit to CMS “on a timely basis” a report explaining their eligibility redetermination activities.
- States must submit data related to individuals whose eligibility information was transferred between Medicaid and the Marketplace, with some exceptions for states that have integrated Medicaid and Marketplace eligibility systems and those that use the Federally Facilitated Marketplace.
Beyond the “Delinking”
The new law includes other important eligibility-related policies that may affect state and stakeholder planning for what is often referred to as the “unwinding” of continuous enrollment. Notably, the state Medicaid and CHIP programs will now be required to provide 12 months of continuous coverage for children. A total of 24 states already have adopted the 12-month continuous eligibility option for all children enrolled in Medicaid. While the new requirement will not take effect until January 1, 2024, additional states could adopt this option as they resume normal eligibility operations.
In addition, the new law makes permanent the option for states to extend Medicaid postpartum coverage to 12 months, up from 60 days. The one-year postpartum coverage option initially was approved in the American Rescue Plan but for a limited period of five years. Making the option permanent provides more certainty for states. Nearly two-thirds of states have already implemented or are planning to implement the 12-month postpartum coverage extension.
What Happens Next?
The definitive end date for the continuous enrollment policy sets in motion certain federal and state actions and the process for unwinding. On January 5, 2023, CMS published its first guidance to states on processes related to the new unwinding date. The agency is developing additional guidance and will use other communication tools to provide states with greater clarity on the new statutory reporting, matching rate, and federal agency expectations and oversight.
State plans: All states must submit unwinding plans to CMS by February 15; however, February 1 is the deadline for states that intend to begin renewals in February. These proposals must provide details regarding unwinding strategies, the timeline for starting enrollee renewals, and the pace of ongoing renewal processes. The specific end date for the continuous enrollment policy is driving more states to review and finalize their initiatives and engage with stakeholders.
Impact on health plans and providers: The unwinding process will create important decision points and considerations for Medicaid health plans and providers that have members and patients whom the unwinding process may affect in the next 12-18 months. The law’s requirements reinforce the imperative for states, Medicaid health plans, providers, and other partners to renew efforts to confirm enrollee contact information. The unwinding all will create new considerations for Medicaid health plans with respect to enrollee support, case mix, and rate setting issues.
State budgets and legislation: Many states will kick off their legislative sessions this month. The unwinding process—especially the phase-out of higher federal funding—has important implications for state budgets. State legislatures also may address the new continuous eligibility requirements for children and the permanent option for 12 months of postpartum coverage. As a result, Medicaid will likely remain a top priority during upcoming legislative sessions.
Federal oversight and enforcement: The law’s enhanced reporting provision is intended to provide safeguards to ensure eligible individuals remain enrolled in Medicaid. The reporting also focuses on data related to identifying and directing individuals likely to be eligible for the Marketplace program. Although CMS must publicly report these data, the agency has offered no specific timeline for posting the information. Notably CMS has oversight tools and may impose financial penalties on states that are noncompliant with the unwinding requirements.
Forthcoming federal guidance will confirm the parameters for state unwinding actions, CMS’s plans for oversight of state work, and how these efforts affect current Medicaid enrollees. Medicaid partners should closely monitor state level actions, including announcement of state unwinding plans and opportunities for collaboration. Earlier blogs describe the strategies and actions HMA is working with states and partners to undertake as they prepare for this significant change in Medicaid eligibility policies.
Please contact HMA experts below for more information.
2022 Yearly Roundup: a year of successful partnerships
The holiday season is grounded in gratitude. At HMA, we are grateful for successful partnerships that have fueled change to improve lives.
We are proud to be trusted advisors to our clients and partners. Their success is our success. In 2022 our clients and partners made significant strides tackling the biggest healthcare challenges, seizing opportunities for growth and innovation, and shaping the healthcare landscape in a way that improves the health and wellness of individuals and communities.
Reforming Colorado’s Behavioral Health System
HMA partnered with the Colorado Department of Human Services to support the planning and implementation of a new Behavioral Health Administration (BHA). HMA provided technical research and extensive stakeholder engagement, drafted models for forming and implementing the BHA, employed an extensive change management approach, and created a detailed implementation plan with ongoing support. Today the BHA is a cabinet member-led agency that collaborates across agencies and sectors to drive a comprehensive and coordinated strategic approach to behavioral health.
Wakely Consulting Group, an HMA Company, was engaged to support the launch of a Medicare Advantage (MA) joint venture partnership between a health plan and a provider system. Wakely was responsible for preparing and certifying MA and Medicare Part D (PD) bids, a highly complex, exacting, and iterative effort. The Wakely team quickly became a trusted advisor and go-to resource for the joint venture decision makers. The joint venture has driven significant market growth over its initial years, fueled by a competitive benefit package determined by the client product team.
Laying the Foundation for Modernizing Indiana’s Public Health System
In 2021 Indiana Governor Eric Holcomb appointed a 15-member commission to assess Indiana’s public health system and make recommendations for improvements. The Indiana Department of Health (IDOH) engaged HMA to provide extensive project management and support for six workstreams. HMA prepared a draft report summarizing public input as well as research findings and recommendations. The commission’s final report will form the basis of proposed 2023 legislation, including proposals to substantially increase public health service and funding across the state.
Multiple Clients Accepted into ACO REACH Model
In early 2022 HMA and Wakely Consulting Group, an HMA Company, assisted multiple clients with their applications to participate in the new CMS ACO REACH model. The purpose of this model is to improve quality of care for Medicare beneficiaries through better care coordination and increased engagement between providers and patients including those who are underserved. The team tailored their support depending on each client’s needs. The application selection process was highly competitive. Of the 271 applications received, CMS accepted just under 50 percent. Notably, nine out of the 10 organizations HMA and Wakely supported were accepted into the model.
Pipeline Research and Policy Recommendations to Address New Innovative Therapies
HMA, and subsidiaries The Moran Company and Leavitt Partners, were selected by a large pharmaceutical manufacturer to analyze the current pipeline of innovative therapies, examine reimbursement policies to assess long-term compatibility with the adoption of innovative therapies and novel delivery mechanisms, and make policy recommendations to address any challenges identified through the process. The project equipped the client with a holistic understanding of future potential impacts and actions to address challenges in a detailed pipeline analysis of innovative therapies.
Should you put the PHE’s Medicaid unwinding at the top of your to-do list?
While the current federal COVID-19 Public Health Emergency (PHE) declaration could be in place through the winter months, HMA’s team of experts see many reasons to put the PHE’s Medicaid unwinding planning at the top of your list now.
Without an extension, the PHE declaration will expire on January 11, 2023. U.S. Department of Health and Human Services (HHS) officials pledged to provide 60-days’ notice before ending the PHE. As a result, since HHS did not announce an extension by November 12, we can assume that HHS Secretary Xavier Becerra will extend the PHE beyond January.
However, congressional leaders are again considering proposals that would impact the PHE’s Medicaid policies. Such a change could advance during the lame duck session of Congress. For a variety of reasons, lawmakers could seek a statutory change that would de-link Medicaid’s continuous enrollment requirement, the 6.2 percentage point increase in the federal Medicaid match, and other Medicaid maintenance of effort policies from the PHE declaration. Congress could set a specific date for ending these Medicaid policies. Doing so would provide more certainty for planning for the end of the continuous Medicaid enrollment policy and its downstream implications for health insurance programs.
What can Medicaid agencies, health plans, providers and other stakeholders do now?
The transition from Medicaid’s continuous enrollment requirement to normal eligibility operations involves a myriad of policy decisions and operational changes that will impact enrollees. In turn, the end of Medicaid’s continuous coverage policy will also have great bearing on the business and operational strategies of managed care plans, providers and other stakeholders participating in the Medicaid and Marketplace programs.
HMA’s experts are working with state agencies, health plans, hospitals and health systems, and other stakeholders to identify options and workable solutions to prepare for these major changes. This work touches policy, organizational workstreams, systems, and payment. There are issues specific to Medicaid as well as the intersection with Marketplace, the Supplemental Nutrition Program (SNAP), and other public programs.
Combining our collective on-the-ground experience in states with our federal policy insights, experts from across the HMA family of companies list below themes and immediate actions stakeholders can consider. These action steps are focused on ensuring states, managed care plans, providers and other stakeholders are prepared to immediately respond to the end of the Medicaid continuous enrollment policy and work with individuals to provide information and other support they may need to stay enrolled in a coverage program.
- Monitor and prepare for federal activities, particularly during the lame duck session of Congress and into 2023.
Healthcare policies are likely to feature prominently in Congress’ lame duck session in November and December. Decoupling the Medicaid continuous enrollment and enhanced Federal Medical Assistance Percentage (FMAP) policies from the PHE is one issue under consideration. Any statutory changes to these policies may also include new requirements for the unwinding process. Stakeholders will want to closely monitor these discussions. If Congress sets a statutory end date for the PHE’s Medicaid eligibility policies, this will provide the certainty needed for states to finalize PHE unwinding action plans with target dates for resuming normal eligibility operations. Notably, this may also drive conversations during states’ 2023 legislative sessions. - Stay informed about state-specific landscapes.
With statewide elections largely decided and expectations for a PHE end date sometime in the first part of 2023, now is the time for stakeholders to revisit when and how to engage with state Medicaid and other state agencies to support Medicaid eligibility unwinding plans. Stakeholders will want to solidify strategies and timing for engaging with states as unwinding plans are further solidified and eventually implemented. Stakeholders can also monitor changes to states’ eligibility and enrollment rules – including initiatives designed to simplify eligibility rules, enhance eligibility and enrollment systems, and adjust managed care rate setting policies, among others. Many states are utilizing the temporary federal Medicaid flexibilities to alleviate the significant eligibility unwinding workload. Federal agencies also continue to regularly publish new information for states and stakeholders to consider. Some states are implementing policies designed to improve the transition from Medicaid to Marketplace. Understanding the implications of such policies will help stakeholders anticipate how ending Medicaid’s continuous coverage requirement will directly affect them. - Refresh strategies and messaging for outreach and assistance.
While the PHE end date remains in flux, state plans for ending the Medicaid continuous coverage policy are still evolving. States are refining their beneficiary communication plans and may be developing updated guidance for stakeholders. Health plans, providers, and other stakeholders should align their messaging and outreach work accordingly and continue to build partnerships in communities across the state. However, outreach alone will not be enough to reach all Medicaid enrollees. Many will need assistance in understanding and complying with changes that come with the end of the continuous enrollment policy. For example, stakeholder-provided redetermination assistance will be key to minimizing the number of enrollees who lose coverage for failure to complete the redetermination process and state requirements for stakeholder assistance will vary state by state. - Update projected impact of enrollee transitions between Medicaid and Marketplace programs. For states and stakeholders, especially health plans, it is time to update projections about 2023 Medicaid and Marketplace enrollment. This may also require new analysis and strategies to address the changing population acuity and resulting impact on capitation revenue. For healthcare providers, health systems, and other healthcare facilities, the end of the Medicaid continuous enrollment policy is expected to drive significant changes in payer mix, and it could reduce revenue as well as impact qualifications for special payment programs, the 340B program, among others. Understanding these dynamics can help with budgeting and implementation of specific patient outreach and support strategies.
5. Develop strategies to translate experiences from Medicaid to Marketplace. Medicaid agencies, managed care plans, and providers have gained valuable insights about the needs of individuals who have remained continuously enrolled in Medicaid during the COVID-19 PHE. This is particularly true for Medicaid enrollees diagnosed with a mental illness, substance use disorder, or both. Medicaid providers and health plans have gained valuable insight on effective clinical care models, whole person care, partnerships with community-based organizations and reimbursement strategies that can better meet the needs of complex populations. Providers and plans can utilize these experiences to better support the millions of individuals who are expected to become eligible for Marketplace coverage after Medicaid’s continuous enrollment policy ends.
The HMA team continues to monitor the dynamic state and federal policy landscapes, including state planning documents and new federal guidance and informational tools. We have the ability to support stakeholders to prepare for the end of PHE and to support state and communities by modeling projected enrollment and payer mix changes across health coverage categories. Stakeholders should be using this time to address gaps in their plans for PHE unwinding and continue to identify and evaluate new options that may emerge to support beneficiaries in retaining health coverage.
For more information, contact our experts below.
HMA identifies key trends in emerging Medicaid Section 1115 demonstration proposals
As the urgent needs of COVID-19 Public Health Emergency (PHE) continue to subside, state Medicaid agencies are exploring pathways and concepts to further address the historic inequities and health disparities laid bare by the pandemic. These efforts are closely aligned with the current Administration’s policy objectives for the Medicaid program, specifically:
- Addressing health equity
- Improving access and coverage
- Promoting whole person care
For several decades, Medicaid Section 1115 demonstration programs have provided a powerful lever for federal and state policymakers to design, implement, and evaluate transformative initiatives. All states administer at least one Section 1115 demonstration program. Some demonstrations are narrowly tailored to address services or populations while others capture broader features pertaining to coverage, benefits, and payment and delivery system innovations.
Notably, a new wave of comprehensive and transformative Medicaid Section 1115 demonstration proposals is emerging.
Working closely with the Centers for Medicare and Medicaid Services (CMS), states are developing proposals that place individuals at the center of health care in an entirely new way – by recognizing their medical needs as well as the complexity of circumstances and environmental factors that shape the individual’s medical, physical, and behavioral care needs and outcomes.
Teams of experts from across the HMA family of companies are supporting state agencies, counties, health plans, providers, community and consumer organizations, and other stakeholders with translating federal goals and parameters into concrete proposals as these move through the stages of concept paper, application and negotiation, and implementation. Demonstrations will reflect each state’s unique political and policy landscapes, but the programs will be grounded in certain federal goals and expectations to enhance accountability and improve outcomes.
Our experts identified three trends in state 1115 demonstration programs. In this and subsequent In Focus posts we will share our team’s initial insights and considerations for stakeholders based on our collective “on the ground” expertise. We include illustrative examples from some states with approved and pending Section 1115 proposals.
Section 1115 Trend #1: States are advancing a new vision for Medicaid’s role in addressing health equity, influenced by social drivers and grounded in a community’s needs.
CMS is strongly encouraging states to consider initiatives that address health inequities and community specific social drivers of health. As evidenced by the current state initiatives, Section 1115 demonstration programs will be a primary — but not the only — pathway states utilize to design strategies to address health inequities driven by non-health systems and circumstances. Based on our work with states and stakeholders, it is critical that states ensure the services are directly linked to factors that impact health outcomes for Medicaid enrollees and that they have mechanisms to evaluate the impact of community and social care services.
Several state proposals already signal CMS’ current vision for using Section 1115 authority to test new types of assistance within service categories to include non-medical services, services tailored to populations, and assistance that is linked to desired outcomes. For example:
North Carolina’s Section 1115 pilot program will provide support to certain groups of consumers for an array of community supports ranging from housing related services and transportation access to interpersonal violence and access to food and nutrition services. The program includes help for consumers related to utility set up and moving costs, and support to connect with community services to address legal issues impacting housing and thereby impacting health.
 In December 2021, CMS approved California’s Section 1115 demonstration program and linked this to a separate waiver approval allowing the state to further enhance services and accountability within its managed care program. As part of California’s implementation of its statewide whole person care initiative, the state will be able to pay for housing navigation and tenancy services and assistance with first month deposits for certain populations enrolled in its statewide managed care program. This proposal is grounded in the state’s commitment to ensure that the non-medical services were clearly defined and clinically oriented for the intended population.
In December 2021, CMS approved California’s Section 1115 demonstration program and linked this to a separate waiver approval allowing the state to further enhance services and accountability within its managed care program. As part of California’s implementation of its statewide whole person care initiative, the state will be able to pay for housing navigation and tenancy services and assistance with first month deposits for certain populations enrolled in its statewide managed care program. This proposal is grounded in the state’s commitment to ensure that the non-medical services were clearly defined and clinically oriented for the intended population.
CMS’ approval of the North Carolina and California programs is paving the way for conversations in other states, including New York, New Jersey, and Oregon among others. Negotiations on similar initiatives to address health equity in other states, include:
 New York, like North Carolina, plans to seek CMS’ approval to offer a range of community services that would be provided through newly established networks of community-based organizations in all regions of the state. The state envisions that the CBO networks will include small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. In addition, New York is asking CMS to support a health equity focused proposal which would provide certain “in-reach” services for incarcerated individuals before they are released.
New York, like North Carolina, plans to seek CMS’ approval to offer a range of community services that would be provided through newly established networks of community-based organizations in all regions of the state. The state envisions that the CBO networks will include small neighborhood organizations familiar with their communities’ needs and the capacity to address multiple social risk factors as well as larger county or regionally focused entities. In addition, New York is asking CMS to support a health equity focused proposal which would provide certain “in-reach” services for incarcerated individuals before they are released.
 Oregon submitted a request to use federal Medicaid spending authority to address community-based health inequities and to establish statewide health equity investments (HEIs). The state is especially focused on supporting consumers during disruptions in coverage, life transitions, or disruptions caused by climate events. Community-based investments will reflect empirical evidence and community assessments and may include efforts to improve building environments and expand culturally and linguistically. Addressing climate events may be of particular interest as it addresses multiple priorities for Administration.
Oregon submitted a request to use federal Medicaid spending authority to address community-based health inequities and to establish statewide health equity investments (HEIs). The state is especially focused on supporting consumers during disruptions in coverage, life transitions, or disruptions caused by climate events. Community-based investments will reflect empirical evidence and community assessments and may include efforts to improve building environments and expand culturally and linguistically. Addressing climate events may be of particular interest as it addresses multiple priorities for Administration.
Conclusion
North Carolina and California offer important insights into what may be possible and as importantly, what may be beyond the bounds of CMS’ Medicaid authority. Chief among the outstanding issues for states and stakeholders is whether additional innovative programs for addressing health disparities among justice-involved populations is possible under Medicaid’s demonstration authority.
CMS may use the experience with initial states to provide more concrete information on these general parameters and expectations. Formal guidance would prove helpful to states and stakeholders seeking to apply new knowledge and experiences with health inequities into practice within the Medicaid programs.
HMA’s interdisciplinary teams of Medicaid, human services, and actuarial experts are assisting states as well as stakeholders as they conceptualize, develop, and implement Section 1115 programs. To learn more about our work and the breadth of our service, contact our expert below.
The PHE is continuing—what’s next for Medicaid?
On May 16, 2022, no announcements were made concerning the impending end of the COVID-19 Public Health Emergency (PHE) declaration. What does this mean for state Medicaid programs and stakeholders, including consumers? When will the PHE declaration expire?
Which Medicare changes should continue beyond the COVID-19 pandemic? Four questions for policymakers
In an issue brief prepared for The Commonwealth Fund and The SCAN Foundation, HMA consultant Jennifer Podulka and Vice President Jonathan Blum, analyze the temporary COVID-19-related changes to Medicare regulations, described the benefits and risks of the changes, and offered a framework to support policymakers’ decisions on the future of these temporary policies.