HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
Health Management Associates (HMA) is proud to offer a 3-part series of webinars looking at the effect of proposed regulations on delivery of opioid treatment services to the population facing addiction issues. In this second webinar, HMA consultants highlighted opportunities for state payers to improve & align incentives so that providers can expand access to treatment enabled by new federal regulations that encourage patient-centered care.
Patients seeking SUD treatment stand to truly benefit from the changes presented in the forthcoming SAMHSA regulations. However, payers need to restructure the reimbursement model to incentivize person-centered care and allow opioid treatment providers to remain fiscally viable without putting undue burden on patients. The change in regulations present a unique opportunity to advance value-based payment models in the SUD treatment system and expand access to treatment that meets patients where they are.
Learning Objectives:
How Payers Can Benefit – Understanding the opportunity for payers to close important gaps in current approaches to SUD treatment.
Innovation Inspiration – Learning from other programs to better deliver whole person care.
Tackling Challenges – Identifying the likely obstacles and how they can be overcome.
Speaker:
Chris Regal, Director, Clinical Innovation, America’s Health Insurance Plans
Stayed tuned for information on part 3 of our Opioid Treatment Providers series: Opportunities for State Regulators to Shape Policy and Regulation of Treatment for Substance Use Disorder
Correctional facilities can decrease the number of individuals with prediabetes who progress to type 2 diabetes by offering the National Diabetes Prevention Program (National DPP) lifestyle change program. HMA has published a white paper describing (1) the financial and individual impact of type 2 diabetes, (2) the prevalence of type 2 diabetes risk factors in correctional settings, and (3) how the National DPP lifestyle change program, which was created by the Centers for Disease Control and Prevention (CDC), can be used to achieve cost savings and better health for people at risk of developing type 2 diabetes in correctional settings.
This white paper also features a program spotlight from the Wisconsin Department of Corrections (DOC), where the National DPP lifestyle change program has successfully been implemented in three state correctional facilities. Wisconsin’s DOC is currently the only correctional system in the United States providing this program that has been awarded full-recognition status as a supplier of the National DPP lifestyle change program by CDC. A total of 131 individuals have participated in the program, and people who completed the program in 2018-2019 lost an average of 8.3 percent of their body weight.
Administrators of correctional settings, where the length of stay is a year or longer, might consider implementing the National DPP lifestyle change program in their facilities. A cogent argument can be made that type 2 diabetes prevention provides a good return on investment in downstream costs. Offering the program would also be an important step in promoting health equity within correctional settings.
For help starting the National DPP lifestyle change program in a correctional facility, contact the white paper’s authors below.
Managed Care Organizations (MCOs) are key partners in ensuring members have access to integrated physical and behavioral health care, which includes a robust, coordinated crisis care continuum. MCOs can also manage early intervention and help prevent crises and high-cost utilization through care coordination.
CRISIS SYSTEM AND SERVICES
Mental health and substance use distress has increased nationally and has been exacerbated by COVID-19. The Federal government in partnership with States and localities around the country are working to expand access to effective crisis interventions. The creation of the national 988 suicide and crisis hotline combined with new funding and guidance on mobile crisis services are critical to preventing and responding to behavioral health crises.
Health Management Associates (HMA) consultants have deep experience and expertise designing, operating, and overseeing crisis services. This includes a broad portfolio of current projects, working with a range of state and local policymakers, payers, providers, first responders, and communities to implement robust crisis continuums.
Opportunities for MCOs
MCOs can play an important role in informing how crisis services meet the needs of their members, and reduce high cost utilization of emergency departments and inpatient care. HMA can help you identify innovative ways to collaborate with States and community-based organizations to drive real access to crisis prevention and intervention services for individuals and families. This work includes building robust crisis continuum networks that include the full array of options, and best practices in crisis response including diversion from and alternatives to expensive emergency department and hospital visits.
This presents an opportunity for MCOs to play a pivotal role in driving better population health outcomes, expanded health equity, improved member experience, and to ultimately reduce the total cost of care.
Our Expertise and Capabilities:
Evidence-based and leading edge clinical and operational practices
Cross-sector partnerships with law enforcement, emergency service providers and community partners
System change by connecting policy to practice
Defining and measuring key performance indicators and outcomes
Identifying effective workforce strategies including training and maximizing of multi-disciplinary teams (e.g., peers, behavioral health providers, nurses, licensed health care providers)
Maximizing virtual and technology interventions
988 state planning and implementation support
Designing and implementing crisis receiving and stabilization facilities
Conducting certified community behavioral health clinic (CCBHC) readiness and implementation support
Cross-sector crisis collaboration and partnerships, including emergency management services (EMS) and law enforcement
Crisis call hotline and 911 centers collaboration
Individuals with Medicaid and justice system involvement (e.g., 1115 waivers, reentry, and care coordination during transition from jail/prison into the community)
Approaches, programs, and strategies for individuals with complex care needs and high utilizers
Identifying cross-sector technology and information sharing solutions and best practices
Crisis transportation services and financing models, including least restrictive alternatives to law enforcement transport
How HMA can assist MCOs:
Strategic Planning
Understanding emerging trends and federal and state policies that impact managed care plans, including maximizing funding streams at state and county levels, 1115 justice waivers and school-based mental health, and including key stakeholders in the planning process.
Design and Implementation
Adopting state Medicaid criminal justice reforms (e.g., in reach, care coordination, Medicaid eligibility); engaging local and county stakeholders in building partnerships with health plans; designing and developing requests for proposals (RFPs), procurement support and readiness reviews; and developing utilization management programs and care coordination strategies.
Training and Support
Assessing benefit design, and developing standards for network development, management, and adequacy; identifying quality, key performance indicators, monitoring and compliance strategies; identification and implementation of evidence-based practices across the age continuum; and developing training standards and oversight.
HMA has valued recent opportunities to support public health departments to collaborate with communities working to identify and address root causes and ultimately reduce maternal and infant mortality and racial disparities in birth outcomes in Delaware and Maryland.
In partnership with the Delaware Department of Health and Social Services’ Division of Public Health, HMA is in its fourth year of administering a mini-grant program and providing backbone services to community-based organizations. These entities provide wraparound services and a variety of other supports to pregnant and parenting people and their families, with the goal of improving maternal and infant health and reducing racial disparities. We also lead a collective impact evaluation of the programs, working closely with the participating organizations to help them build their capacity to collect and analyze data, developing interim and annual reports, and providing frequent updates to the Division of Public Health and other stakeholders in the state that are collaborating to improve health and wellbeing. HMA provides fiscal and administrative oversight, coaching and evaluation, and convenes the participating organizations for quarterly learning collaboratives, which have contributed to stronger relationships and collaboration among the mini-grantees. In addition, we are implementing and evaluating a guaranteed basic income program as part of the Social Determinants of Health committee of the Delaware Healthy Maternal Infant Consortium (DHMIC). This project is a long-term commitment to collaborating with community-based organizations to build their capacity to address racial disparities and support their work, which is driven by the needs of the people they serve and know best. Grantees are selected through a streamlined process with low administrative burden, prioritizing community input on needed services. Through a collective impact evaluation, the participating organizations are finding positive effects on the self-reported health and wellbeing of program participants.
Launch of the first cohort of Healthy Women Healthy Babies Zones Mini-grantees in 2019. Photo Credit: Division of Public Health – Delaware Health and Social Services
With the Frederick County, Maryland Health Department, HMA conducted a study in 2022 using a community-based participatory research (CBPR) approach to understand and articulate drivers of maternal and infant health disparities experienced by Black women in Frederick County. In collaboration with the health department and newly formed Community Advisory Board (CAB), we facilitated a series of in-person retreats to: collect, analyze, and share quantitative and qualitative data regarding disparities and the drivers of those disparities with stakeholders; understand the data and the story behind the health disparity numbers; and develop and deploy additional research methods, such as surveys, key informant interviews, and focus groups, to further explore the lived experience of Black Frederick County mothers. This iterative approach to conducting mixed-methods research uses the CBPR framework to ensure sustained and meaningful community engagement from project start to end. HMA also developed a driver diagram to illustrate how the root cause, systemic racism, directly influences other drivers of Black maternal health disparities such as historic disinvestment in Black maternal health, historical trauma navigating healthcare, low social capital, health insurance availability, and a perceived lack of emotional and physical safety in clinical settings. The diagram will be shared with relevant stakeholders and inform next steps.
In our reproductive health-related work, HMA has guided groups through decision-making processes, with transparency and without bias, and we understand the importance of group dynamics. Bringing decades of real-world public policy and community and key stakeholder facilitation experience, HMA collaborates with a variety of stakeholders and community members to develop and implement public policy at the local and state levels, as well as to evaluate these efforts. Our experience ranges from national, state, and county agencies, to private sector and community-based organizations that partner with governments to implement policy. Our team has extensive experience working with and within organizations to facilitate discussions, listen to and build consensus across sectors, develop strategic plans, and bring diverse perspectives together to promote health and wellness for communities.
HMA colleaguesparticipating in these projects include: Sarah Arvey, Brandin Bowden, Ana Bueno, Liddy Garcia Buñuel (Delaware project director), Akiba Daniels, Marci Eads, Michelle Ford, Allie Macdonald, Kristan McIntosh, Yamini Narayan, Diana Rodin, Hannah Savage, and Maddy Shea (Frederick County project director). The Frederick County project was done in consultation with Dr. Chidinma Ibe, Assistant Professor of General Internal Medicine at Johns Hopkins University School of Medicine with expertise in community-engaged research.
As part of recognizing Women’s History Month, HMA colleagues reflected on recent work to support maternal and infant health and reduce racial disparities in birth outcomes in collaboration with health departments and communities in Delaware and Maryland. More information on our recent projects supporting reproductive health can be found here.
Utilization of value-based payment (VBP) strategies continues to expand, with states and health plans recognizing the benefits of rewarding outcomes over volume. This includes population based VBP initiatives intended to address disparities. Health Management Associates (HMA) is at the center of these initiatives, supporting payers with development and implementation, as well as supporting providers through the transition from a traditional FFS model to maximizing reimbursement through effective care delivery, supported by the necessary administrative infrastructure and resources. As our clients in health care communities move forward with alternative payment models, we have developed tools and strategies to achieve the essential milestones to successful implementation.
Milestone 1: Provider Readiness Assessment
Successful planning for the transition to VBP begins with an understanding of where your organization is starting from, informing the targeted milestones associated with each providers’ unique strengths and challenges.
Understanding that success under VBP models requires adjustment of both clinical and administrative practices, HMA has created an assessment tool that considers the programmatic, financial, and technology resources necessary for VBP implementation. In addition to the ability to leverage these resources, organizations must have the capacity for VBP components such as cost reporting, revenue cycle management, and real time risk monitoring through the collection and analysis of data.
“With VBP on the horizon for our organization, HMA helped us to determine our readiness and to devise a strategy to remediate gaps in operations in order to be successful with the new payment model.”
– Tamara Player, CEO; Polara Health, AZ
Milestone 2: Strategy Development and Change Management
A change in reimbursement methodology requires organizational realignment of administrative and programmatic approaches. Assessing and supporting staff through these changes is a key milestone for success. Activities in which HMA have supported our clients include:
Creating leadership and governance buy-in
Preparing the Board and Staff for VBP
Aligning mission and vision with payment models and accountability metrics
Project Management, including development and monitoring of implementation plans
Cross functional team support
Milestone 3: Data Collection and Reporting Capabilities
The ability to collect and report meaningful outcomes is at the core of successful engagement in VBP. Following an assessment of current capabilities, HMA has supported provider organizations in maximizing electronic health record and other data system capabilities to capture data essential for reimbursement, as well as increasing analytic capabilities that are essential for monitoring outcomes to ensure programs can pivot when data indicates outcome achievement may be at risk. Activities include:
Technology and Data Enterprise configuration to support analytics and reporting
Creating real-time access to data
Benchmarking current outcomes against proposed VBP metrics
Alignment of current framework to payer metrics
Creation of internal clinical leadership infrastructure to support proactive monitoring and action in response to data
Milestone 4: Business Office and Finance
All aspects of an organization’s financing can be impacted by transitions in payment methodology, including cash flow, impacting cash on hand for capital and other expenses. Anticipating these changes and adjusting accordingly are key to readiness for VBP and importantly, mitigating risk during the transition. HMA can assist with:
Assessing organizational ability to accept risk
Developing a risk corridor based on organizational readiness
Negotiating alternative payment arrangements with payers
Milestone 5: Clinical Programmatic Approaches under VBP
VBP arrangements provide opportunities for organizations to move closer to the goal of achieving outcomes for their clients, rather than productivity targets and units of service. This includes incorporating approaches that could not receive reimbursement under an FFS model. With this flexibility comes the opportunity to review and adapt clinical approaches and programming, including population specific strategies. HMA is ready to support these efforts through:
Workforce analysis
Re/design of clinical workflows
Implementation of measurement-based care
Optimization of clinical templates within the EHR to support data collection and reporting
Understanding the opportunities of value-based payment across the continuum of payment models
While these activities may seem overwhelming, HMA is ready to support your organization to receive reimbursement based on meaningful improvement for your clients through technical assistance and training on each of the core elements outlined above.
Rachel Bembas is a results-driven leader in behavioral health quality and population health analytics who has worked extensively to advance … Read more
Debbi Witham is a seasoned executive with experience delivering high quality, mission driven healthcare. During her career, she has focused … Read more
HMA has published a white paper examining the use of risk mitigation strategies among state Medicaid programs and assessing their limiting impact on capitation’s incentives for managed care organizations (MCOs). This paper seeks to assist policymakers in designing future Medicaid program payment policies that advance state financial and programmatic goals. This paper offers a timely examination of this topic as state Medicaid programs emerge from the COVID-19 public health emergency (PHE) and navigate the unwinding of Medicaid continuous coverage. This paper also builds upon the Health Management Associates May 2021 white paper, Moving Beyond COVID-19 Public Health Emergency Risk Corridors, which more narrowly focused on appropriate and inappropriate use of risk corridors.
One of only two firms selected in all seven domains out of 46 vendors.
The California Department of Health Care Services (DHCS) has developed a multi-year initiative whose goal is to improve health outcomes and health care quality through broad delivery, payment, and program reforms known as California Advancing and Innovating Medi-Cal (CalAIM). This includes the introduction of new programs and changes to existing programs that will occur over the span of five years. CalAIM further expands upon prior initiatives, such as Whole Person Care, the Health Homes Program, and the Coordinated Care Initiative, and strives to integrate California’s delivery systems to better facilitate the overall Medi-Cal program.
With the rollout of these programs and the vast requirements associated with them, DHCS and California’s Medi-Cal managed care health plans are now tasked with the challenge of implementing CalAIM and enabling the participation of community providers and partners in these opportunities. To support these partners, DHCS developed a funding initiative, known as Providing Access and Transforming Health (PATH) to aid in strengthening capacity and infrastructure of Community Based Organizations, public hospitals, county agencies, and others to stand up CalAIM. This five-year, $1.85 billion initiative includes the creation of a virtual Technical Assistance (TA) Vendor Marketplace that organizations can use to request resources and support from approved vendors through services that are fully paid for by the State.
Health Management Associates (HMA) is recognized as a valued partner to Payers, Community Based Organizations, public hospitals, and county agencies and has deep expertise in CalAIM policy, operations and implementation. Recognized for our extensive capabilities in the field, HMA is one of only two firms out of 46 vendors that received State approval to serve as a technical assistance vendor on the PATH Technical Assistance (TA) Marketplace for all seven domains:
Domain 1: Building Data Capacity: Data Collection, Management, Sharing, and Use
Domain 2: Community Supports: Strengthening Services that Address the Social Drivers of Health
Domain 3: Engaging in CalAIM Through Medi-Cal Managed Care
Domain 4: Enhanced Care Management (ECM): Strengthening Care for ECM Population of Focus
Domain 5: Promoting Health Equity
Domain 6: Supporting Cross-Sector Partnerships
Domain 7: Workforce
HMA also has expertise in and hands-on experience with addressing the unique challenges experienced by providers and partner agencies serving rural communities. Please visit the PATH Technical Assistance (TA) Marketplace to access TA resources that can help strengthen capacity to provide high quality Enhanced Care Management (ECM) and Community Supports services for Medi-Cal members.
This week, our In Focus section reviews the New Hampshire Medicaid Care Management (MCM) request for proposals (RFP), which the state’s Department of Health and Human Services released on September 8, 2023. The new contracts will be worth approximately $1.1 billion and will provide full-risk, fully capitated Medicaid managed care services to approximately 190,000 beneficiaries. Implementation will begin September 2024.
MCM Program
The MCM program covers traditional Medicaid, the Children’s Health Insurance Program (CHIP), and the state’s adult Medicaid expansion Granite Advantage Health Care Program. MCM provides integrated acute care, behavioral health, and pharmacy services. Managed long-term services and supports are not included in the program.
Incumbents are AmeriHealth Caritas, Boston Medical Center/WellSense, and Centene/New Hampshire Healthy Families.
RFP
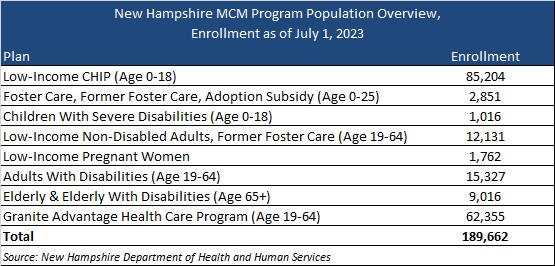
New Hampshire will award contracts to three Medicaid managed care organizations (MCOs). MCOs will cover the populations outlined in Table 1.
Table 1. New Hampshire MCM Program Enrollment as of July 1
The state outlines several key areas of focus within the RFP, including introducing a primary care and preventive services model of care—an approach centered on patient-provider relationships and provider-delivered care coordination. The RFP also will have a greater emphasis on priority populations, such as individuals with inpatient admissions for behavioral health diagnoses; children in the child welfare system; babies with low weight or neonatal abstinence syndrome; and people who are incarcerated and eligible for the Community Reentry demonstration program, pending approval from the Centers for Medicare & Medicaid Services.
Timeline
Mandatory letters of intent are due September 18, 2023, and a mandatory conference will take place September 21. Proposals are due October 30, 2023. An award date has yet to be announced, but the state contract discussions with selected MCOs will occur November 20−December 11, 2023. Contracts will run from September 1, 2024, through August 31, 2029.
Evaluation
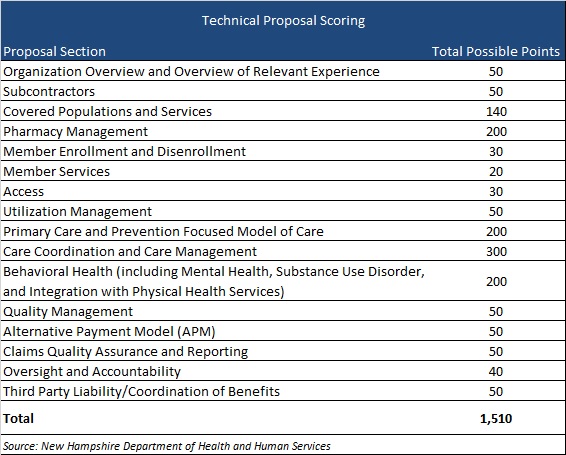
MCOs will be scored on their ability to meet a possible 2,160 points. The technical proposal comprises a possible 1,510 points, as shown in Table 2.
Table 2. Technical Proposal Scoring
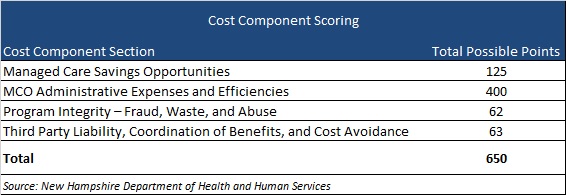
The cost component sections will make up 650 points, as shown in Table 3.
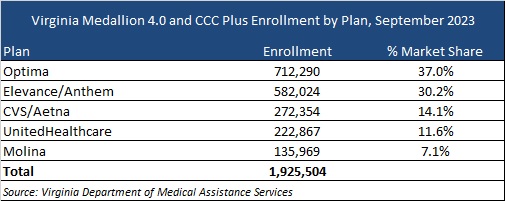
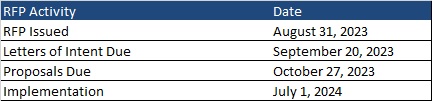
This week, our In Focus section reviews the request for proposals (RFP) for the Virginia Cardinal Care Medicaid managed care program, released by the Department of Medical Assistance Services (DMAS) on August 31, 2023. The RFP includes a new foster care specialty plan. Implementation is scheduled to begin July 1, 2024.
Cardinal Care
Cardinal Care launched in January 2023 as a rebranding of the state’s Medicaid program and Children’s Health Insurance Program—Family Access to Medical Insurance Security Plan (FAMIS). Cardinal Care Managed Care (CCMC) will combine the state’s existing Medallion 4.0 managed care program for traditional Medicaid and the Commonwealth Coordinated Care Plus (CCC Plus) managed long-term services and supports (MLTSS) program to serve 1.9 million Medicaid managed care members.
RFP
The state will award statewide fully capitated, risk-based contracts to a maximum of five health plans. A separate foster care specialty plan contract will also be awarded to one of the winners. If none of the plans win the separate foster care specialty program, all plans awarded a CCMC contract will be required to cover all services.
Selected plans will provide acute care, behavioral health, and MLTSS services to all Virginians who are eligible for Medicaid, including children, adults, and pregnant women in low-income households; children and adults with disabilities; low-income older adults; and individuals receiving LTSS, including dual-eligible populations. The foster care plan will cover children in foster care, individuals younger than 26 years old who were formerly in foster care, and children eligible for adoption assistance.
The RFP contains several targeted focus areas and changes to the managed care program. For example, it emphasizes improvements to the state’s behavioral health care system and improved health outcomes through a focus on health-related social needs such as housing stability and food insecurity for CCMC members.
Contracted plans will be required to operate a dual-eligible special needs plan (DSNP) in Virginia.
Market
CVS/Aetna, Elevance/Anthem, Sentara/Optima Health, Molina, and UnitedHealthcare are the current incumbents. Effective with the new RFP, DMAS intends to reassign most CCMC members as part of an enrollment process. At present, Optima holds the largest market share of enrollment at 37 percent, followed by Anthem at 30 percent.
Timeline
Letters of intent are due by September 20 and proposals are due on October 27. As previously mentioned, new contracts will begin July 1, 2024. Contracts will have a six-year initial term, with two two-year renewal options. Award dates have not been announced.
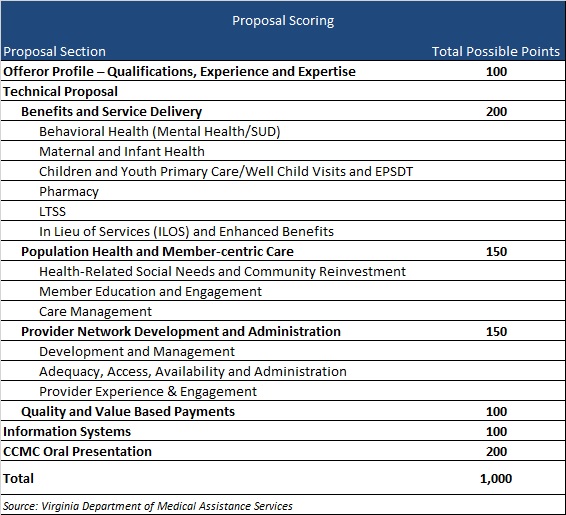
Evaluation
Plans will be awarded up to 1,000 points during the evaluation process based on the categories shown below.
Dedicated to supporting the effectiveness of publicly financed healthcare programs, Health Management Associates (HMA) is committed to promoting the design, financing and operation of effective models of person-centered long-term services and supports (LTSS) which:
Support an individual’s ability to receive services in the most integrated setting
Promote successful community living
Improve integration of LTSS with quality physical and behavioral healthcare
Support Medicare and Medicaid integration and coordination
Address the social determinants of health for people with support needs
Support direct care workforce initiatives for states, managed care organizations and long-term care providers
Support strategic planning focused on long-term care
Support managed care readiness initiatives
What we offer
With deep expertise in the field, our colleagues and the work we do help to shape current system trends. In addition, we support improved outcomes for beneficiaries and successful participation for the wide range of LTSS providers including managed care organizations, states offering critical services, and purchasers through:
LTSS Models of Care
Developing and promoting person-centered integrated, and holistic LTSS models of care
LTSS Quality Standards
Supporting the development of LTSS quality standards and metrics, including technical assistance for NCQA and other accreditation and credentialing
LTSS Regulatory Compliance
Facilitating readiness and compliance with federal and state regulations, including home and community-based settings of care, Medicaid managed care, the Fair Labor Standards Act, and the Americans with Disabilities Act
LTSS Integration
Implementing care management and service delivery models that promote integration of services across physical, behavioral, and LTSS providers and between Medicare and Medicaid including those developed under PACE, managed LTSS, and managed fee-for-service
LTSS Stakeholder Engagement
Supporting effective community engagement by public policy makers, and empowering advocacy organizations and other stakeholders in understanding, shaping, and responding to change
LTSS Delivery and Payment Models
Assisting organizations and providers to prepare and respond to payment and structural changes in LTSS (e.g., managed care, accountable care, value-based purchasing)
LTSS and Social Determinants Design
Designing innovative approaches to addressing the social determinants of health, including improved strategies for affordable and accessible housing, competitive employment for persons with disabilities, access to technology, and social equity-based care delivery models
LTSS Market Analysis
Providing expert market analysis for investors relating to LTSS providers, managed care organizations, service vendors, or emerging trends in the LTSS landscape
LTSS Research and Evaluation
Enabling the use of data to uncover opportunities for improvement and to demonstrate value to ACOs, hospital systems, payers, and funders
Our wide-ranging expertise includes:
Medicaid LTSS waiver and state plan authority options
Operation and oversight of managed LTSS
Public procurements
LTSS provider operations
Federal and state compliance
Care management and care coordination
Workforce development
Strategic planning and practice redesign
LTSS policy analysis
Value-based purchasing
Quality monitoring, evaluation and research
Community capacity and network adequacy
Readiness reviews
Our Clients Include:
Federal, state and local governments
For-profit, not-for-profit and public health plans
Institutional and home and community-based services providers and their associations
Sharon Lewis is a nationally lauded expert in federal and state disability policy, including home and community-based services (HCBS), education, … Read more
Susan McGeehan is a multi-faceted healthcare leader with extensive experience in dual eligible programs, long-term services and supports (LTSS), Medicaid … Read more