As states and stakeholders seek greater transparency and accountability in Medicaid, a new analysis from Health Management Associates (HMA), offers a fresh perspective on how dollars flow through the system. Drawing on publicly available data from the Transformed Medicaid Statistical Information System (T-MSIS), HMA disaggregated funding dispersed to Medicaid managed care organizations to discern spending for specific categorically eligible populations. The findings significantly enhance policy discussions and can facilitate development of pragmatic and specific care management interventions that support quality patient care.
For policymakers, regulators, and other stakeholders, this level of disaggregation provides a clearer view of how public dollars are used—and where there may be opportunities to improve performance or reinvest savings. It also supports more informed rate development and contract negotiations, particularly as states pursue value-based purchasing and other reforms. As Medicaid continues to evolve, especially in the context of budget pressures and changes in enrollment and risk profiles of enrollees, understanding the financial picture of managed care programs is essential to ensuring sustainability.
HMA’s team of experts—including actuaries, former Medicaid directors, and data analysts—has deep experience working with T-MSIS data and advising states, plans, and providers on Medicaid program analysis, evaluation, and strategy. For more information about working with T-MSIS data and the insights it can provide, contact our experts below.
In this week’s In Focus section, Health Management Associates Information Services (HMAIS) draws on its database of monthly enrollment in Medicaid managed care programs to provide the latest quarterly analysis of Medicaid managed care enrollment, offering a snapshot of developments across 28 states.[1] The data and insights are particularly timely as stakeholders, including states, Medicaid managed care organizations (MCOs), hospitals and health systems, and providers, continue to plan for multiple possible federal policy changes and the operational realities that will follow.
HMAIS also compiles a more detailed quarterly Medicaid managed care enrollment report representing nearly 300 health plans in 41 states. The report provides by plan enrollment plus corporate ownership, program inclusion, and for-profit versus not-for-profit status, with breakout tabs for publicly traded plans. Table 1 shows a sampling of plans and their national market share of Medicaid managed care beneficiaries based on a total of 66 million enrollees. These data should be viewed as a broader representation of enrollment trends rather than as a comprehensive comparison.
Key Insights from Q1 2025 Data
The 28 states included in our review have released monthly Medicaid managed care enrollment data via a public website or in response to a public records request from Health Management Associates (HMA). This report reflects the most recent data posted or obtained. HMA has made the following observations related to the enrollment data:
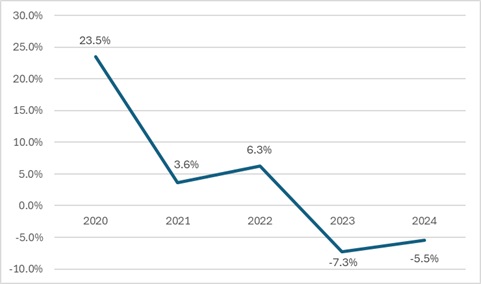
Year-over-year growth. As of March 2025, across the 28 states reviewed, Medicaid managed care enrollment declined by 2.5 million members year-over-year, a 3.9 percent drop as of March 2025 (see Figure 1). This marks a continuation of the downward trend reported in late 2024, though with notable variation across states.
Figure 1. Year-over-Year Growth in Medicaid Managed Care States, 2020−24, March 2025
Localized growth amid broader declines. While most states experienced enrollment reductions, Indiana and North Carolina bucked the trend with measurable gains, suggesting the influence of state-specific policy shifts or demographic factors. Oregon and Texas also saw modest growth.
Sharpest contractions. Illinois, Maryland, and South Carolina, reported double-digit percentage drops, underscoring the uneven impact of redeterminations and eligibility changes.
Difference among expansion and non-expansion states. Among the 21 states included in our analysis that expanded Medicaid, enrollment fell by 1.8 million (-3.6%) to 48.6 million. In contrast, the seven non-expansion states saw a steeper proportional decline (-5.4%), to a total of 12.2 million enrollees.
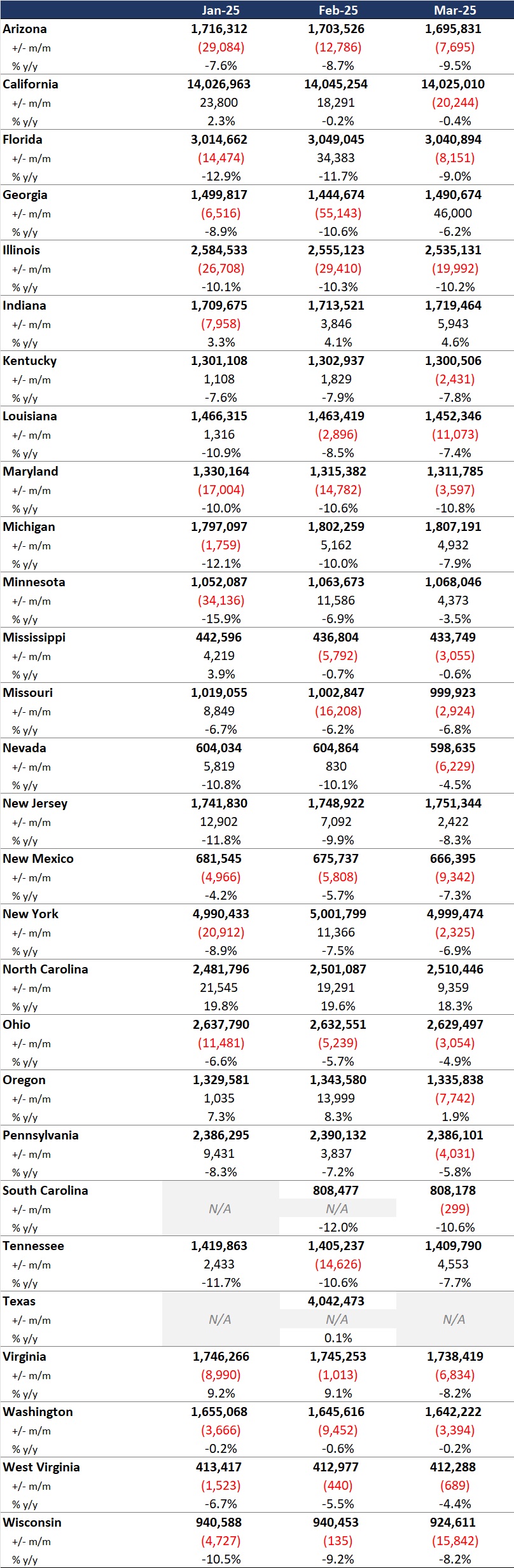
Table 1. Monthly MCO Enrollment by State, January 2025 through March 2025
Note: In Table 1 above and the state tables that follow, “+/- m/m” refers to the enrollment change from the previous month, and “% y/y” refers to the percentage change in enrollment from the same month in the previous year.
It is important to note the limitations of the data presented. First, states report the data at the varying times during the month. Some of these figures reflect beginning of the month totals, whereas others reflect an end of the month snapshot. Second, in some instances, the data are comprehensive in that they cover all state-sponsored health programs that offer managed care options; in other cases, the data reflect only a subset of the broader managed Medicaid population. This limitation complicates comparison of the data described above with figures reported by publicly traded Medicaid MCOs. Hence, the data in Table 1 should be viewed as a sampling of enrollment trends across these states rather than a comprehensive comparison, which cannot be established solely based on publicly available monthly enrollment data.
Market Share and Plan Dynamics
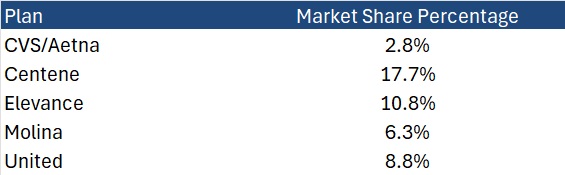
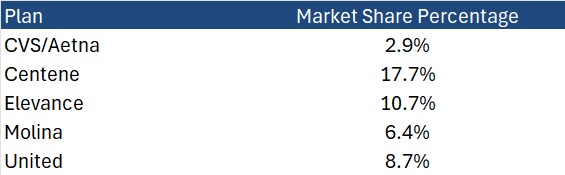
Using our data repository from 300 health plans across 41 states, HMAIS’s report addresses corporate ownership, program participation, and tax status. As of March 2025, Centene continues to lead with 17.7 percent of the national Medicaid managed care market, followed by Elevance (10.8%), United (8.8%), and Molina (6.3%), as Table 2 shows.
Table 2. National Medicaid Managed Care Market Share by Number of Beneficiaries for a Sample of Publicly Traded Plans, March 2025
What to Watch
The policy backdrop remains fluid. The US House of Representatives’ passage of the One Big Beautiful Bill Act introduces sweeping changes to Medicaid financing, including proposed cuts of up to $715 billion. Additional federal proposals, such as mandatory work requirements, could further reshape enrollment patterns.
Stakeholders should prepare for:
Implementation of work/community engagement mandates for certain adult populations
Potential redesign of Affordable Care Act expansion programs
Retraction of federal regulations focused on streamlining of eligibility and redetermination processes to improve accuracy and efficiency
Connect with Us
HMA is home to experts who know the Medicaid managed care landscape at the federal and state levels. As the Medicaid landscape continues to evolve, HMAIS equips stakeholders with timely, actionable intelligence. Our subscription service includes enrollment data, financials, waiver tracking, and a robust library of public documents.
For more information about the HMAIS subscription, contact our experts below.
[1] Arizona, California, Florida, Georgia, Illinois, Indiana, Kentucky, Louisiana, Maryland, Michigan, Minnesota, Mississippi, Missouri, Nevada, New Jersey, New Mexico, New York, North Carolina, Ohio, Oregon, Pennsylvania, South Carolina, Tennessee, Texas, Virginia, Washington, West Virginia, Wisconsin.
Our second In Focus section reviews the most recent Medicaid enrollment trends in capitated risk-based managed care programs in 29 states.[1] Health Management Associates Information Services (HMAIS) collected and analyzed monthly Medicaid enrollment data from the fourth quarter (Q4) of 2024.
The data offer a timely overview of trends in Medicaid managed care enrollment and valuable insights into state-level and managed care organization (MCO)-specific enrollment patterns. This information allows state governments, their partners, and other organizations interested in Medicaid to track enrollment shifts. Understanding the underlying drivers of enrollment shifts is critical for shaping future Medicaid policies and adjusting program strategies amid a dynamic healthcare landscape.
Overview of the Data
The 29 states included in our review have released monthly Medicaid managed care enrollment data via a public website or in response to a public records request from Health Management Associates (HMA). This report reflects the most recent data posted or obtained. HMA has made the following observations related to the enrollment data (see Table 1):
As of December 2024, across the 29 states tracked in this report, Medicaid managed care enrollment was 61.7 million, down by 3.6 million (-5.5%) year-over-year.
Though most states experienced declines in enrollment, six states saw enrollment increases as of December 2024—double the number of states from the previous year.
Figure 1. Year-Over-Year Medicaid Managed Care Enrollment Percent Change in Select States, 2020−24
Among the 22 expansion states included in this report, net Medicaid managed care enrollment has decreased by 2.1 million (-4%) to 49.5 million members at the end of Q4 2024, compared with the same period in 2023.[2]
Among the seven states included in this report that had not expanded Medicaid as of December 2024, net Medicaid managed care enrollment decreased by 1.5 million, or 1 percent, to 12.3 million members at the end of Q4 2024 compared with to the same period in 2023.
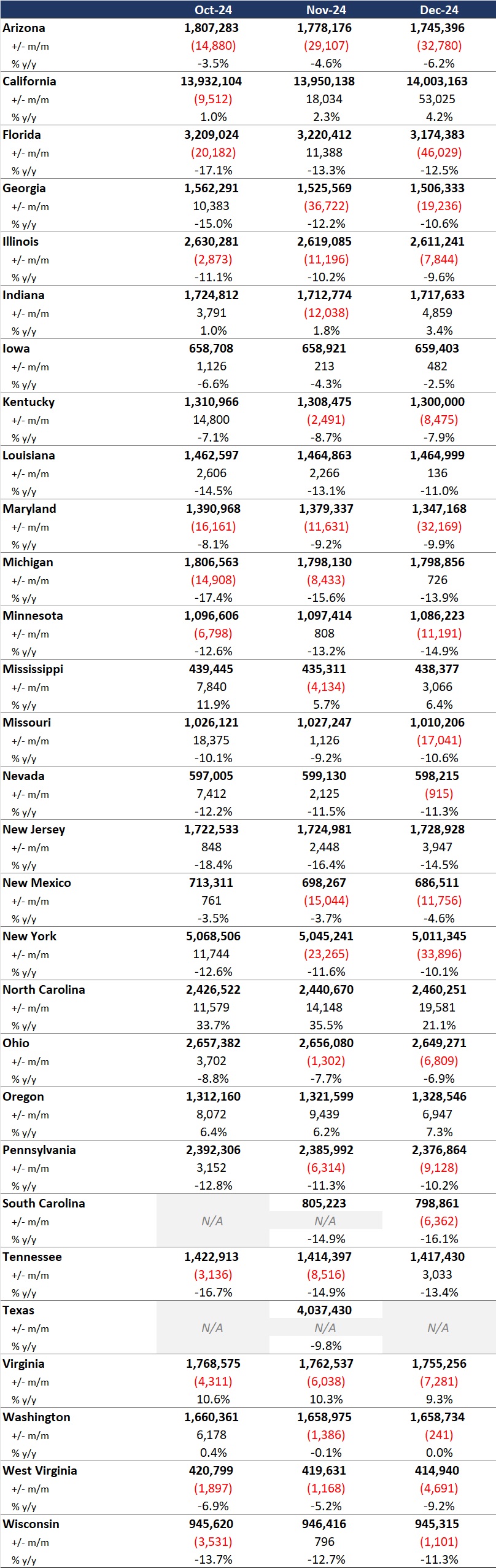
Table 1. Monthly MCO Enrollment by State—October through December 2024
Note: In Table 1 above, “+/- m/m” refers to the enrollment change from the previous month. “% y/y” refers to the percentage change in enrollment from the same month in the previous year.
It is important to note the limitations of the data presented. First, not all states report the data at the same time during the month. Some of these figures reflect beginning of the month totals, whereas others reflect an end of the month snapshot. Second, in some cases the data are comprehensive in that they cover all state-sponsored health programs that offer managed care options; in other cases, the data reflect only a subset of the broader managed Medicaid population. This limitation complicates comparison of the data described above with figures reported by publicly traded Medicaid MCOs. Hence, the data in Table 1 should be viewed as a sampling of enrollment trends across these states rather than as a comprehensive comparison, which cannot be established based solely on publicly available monthly enrollment data.
HMAIS also compiles a more detailed quarterly Medicaid managed care enrollment report representing nearly 300 health plans in 41 states. The report provides by plan enrollment plus corporate ownership, program inclusion, and for-profit vs. not-for-profit status, with breakout tabs for publicly traded plans. Table 2 shows a sampling of plans and their national market share of Medicaid managed care beneficiaries based on a total of 66.3 million enrollees. These data too should be viewed as a broader representation of enrollment trends rather than as a comprehensive comparison.
Table 2. National Medicaid Managed Care Market Share by Number of Beneficiaries for Sample of Publicly Traded Plans, 2024
What to Watch
Enrollment in Medicaid MCOs has experienced significant fluctuations recently, influenced both by policy changes and economic factors. Since April 2023, Medicaid enrollment has been on a downward trajectory as states complete eligibility redeterminations after the end of the COVID-19 public health emergency. This trend, coupled with financial and political challenges, necessitates strategic planning for stakeholders to navigate the evolving Medicaid landscape effectively.
Potential changes that may affect enrollment and require scenario and readiness planning include:
Federal requirement, or a new state option, to implement Medicaid work requirements for at least some categories of enrollees
Changes to the federal financial match policy, which may cause some states to make different decisions about their Affordable Care Act expansion program for adults
Modifications in requirements and expectations for more efficient eligibility processes to improve the accuracy of determinations and assignment to eligibility categories
Connect with Us
HMA is home to experts who know the Medicaid managed care landscape at the federal and state levels. The HMAIS subscription provides point-in-time and longitudinal Medicaid enrollment data, health plan financials, and additional actionable information about eligibility expansions, demonstration and waiver initiatives, as well as population- and service-specific information. HMAIS also includes a comprehensive public documents library containing Medicaid requests for proposals and responses, model contracts, scoring sheets, and protests.
For detail about the HMAIS enrollment report and subscription service, contact our experts below.
[1] Arizona, California, Florida, Georgia, Illinois, Indiana, Iowa, Kentucky, Louisiana, Maryland, Michigan, Minnesota, Mississippi, Missouri, Nevada, New Jersey, New Mexico, New York, North Carolina, Ohio, Oregon, Pennsylvania, South Carolina, Tennessee, Texas, Virginia, Washington, West Virginia, Wisconsin.
Notably, because of the timing of the draft notices and proposed rule, Trump Administration officials ultimately had more input into policies omitted from the rate notice and final policy rule than on policies that were finalized. For example, the final rule is exclusive of proposals to expand coverage for anti-obesity medications, guardrails for artificial intelligence (AI), and new requirements related to utilization management and prior authorization procedures.
In his confirmation hearing, CMS Administrator Mehmet Oz, MD, cited Medicare Advantage prior authorization practices and health risk assessments that lead to upcoding as areas that deserve further consideration and scrutiny, raising the potential for future regulatory shifts and even legislative reform. With the possibility of Medicare, including MA, facing cuts as part of broader budget negotiations in Congress, the rate notice and policy rule offer program stability counterbalancing the political and fiscal pressures that may emerge this year.
CMS has sought to stabilize MA and Part D programs into 2026, and stakeholders can benefit from understanding the impact in markets for 2026 and the signals of potential regulatory changes to come. For more in-depth analysis and insights on the rate notice, look for our policy and actuarial experts’ brief due out next week.
The remainder of this In Focus article reviews CMS’s decisions on major payment and policy proposals in the Rate Announcement and Final Rule and examines key considerations for healthcare stakeholders.
Payment Impact on Medicare Advantage Organizations
In the CY 2026 Rate Announcement, CMS projects that federal payments to MA plans will increase by 5.06 percent from 2025 to 2026, which represents a $25 billion increase in expected payments to MA plans next year. According to CMS, this represents an increase of 2.83 percentage points compared with the CY 2026 Advance Notice that is largely attributable to an increase in the effective growth rate. The increase in the effective growth rate—increasing to 9.04 percent in the Rate Announcement from 5.93 percent in the Advance Notice—is primarily the result of the inclusion of additional data on Medicare fee-for-service (FFS) expenditures, including payment data through the fourth quarter of 2024.
The Rate Announcement estimates represent the average increase in payments to MA plans and actual payments will vary from plan to plan. Below, Table 1 provides CMS estimates of the impact of finalized payment changes on net MA plan payments.
MA Risk Adjustment Changes
As expected, CMS finalized the last year of the three-year phase-in of the MA risk adjustment model, which requires calculating 100 percent of the risk scores using only the 2024 CMS-HCC (Hierarchical Condition Category) model in 2026. CMS also addressed stakeholder concerns with the planned transition toward a risk adjustment model based on MA encounter data, as previewed in the CMS CY 2026 Advance Notice. CMS pledged to engage stakeholders in this model development process while continuing to evaluate the feasibility, transparency, and timing of a future transition to an encounter-based risk adjustment model.
CMS also finalized the MA coding pattern adjustment factor of 5.9 percent for CY 2026, which is the statutory minimum adjustment factor to account for differences in coding patterns between MA plans and providers under Medicare FFS Parts A and B.
Part D Risk Adjustment
For CY 2026, CMS finalized the revised 2026 RxHCC model with adjustments for maximum fair price drugs. Importantly, CMS also finalized using separate FFS normalization factors for MA-Prescription Drug (MA-PD) plans and Prescription Drug Plans (PDPs), making 2026 the second year CMS will vary normalization for these two markets. The calculation of the factors for CY 2026 is different, however, and will have substantially greater impact than the method used previously. It also will reduce Part D risk scores significantly for MA-PD plans while increasing scores for PDPs.
MA Star Ratings
CMS continues to solicit feedback from stakeholders on ways to simplify and refocus MA Star Ratings measures to focus more on clinical care, outcomes, and patient experience of care measures. Also included in the CY 2026 Rate Announcement are non-substantive measure specification updates and a list of measures included in the Part C and Part D improvement measures and categorical adjustment index for the 2026 Star Ratings.
Separately, in the policy and technical changes rule, CMS finalized new regulatory requirements designed to enhance MA beneficiary protections in an inpatient setting, provisions related to allowable special supplemental benefits for the chronically ill (SSBCI), and the care experience for dually eligible beneficiaries enrolled in MA special needs plans.
Enhancing MA Beneficiary Appeal Rights and Notification Requirements
CMS is finalizing provisions that limit the ability of MA plans to reopen and modify a previously approved inpatient hospital decision on the basis of information gathered after the approval. Under the final rule, MA plans will be able to reopen an approved hospital admission only due to error or fraud. In addition, CMS finalized several provisions to enhance beneficiary appeal rights and new reporting and notice requirements, including:
Ensuring that MA appeals rules apply to adverse plan decisions, regardless of whether the decision was made before, during, or after the receipt of such services
Codifying existing guidance that requires plans to give a provider notice of a coverage decision
Ensuring enrollees have a right to appeal MA plan coverage denials that affect their ongoing source of treatment
Non-Allowable Special Supplemental Benefits for the Chronically Ill
The final rule establishes guardrails for SSBCI benefits by codifying a list of non-allowable examples (e.g., unhealthy food, alcohol, tobacco, life insurance). CMS did not finalize proposals that were designed to improve administration of supplemental benefits and enhance transparency of the availability of such benefits.
Improving Care Experience for Dual Eligibles
CMS finalized new requirements for dual eligible special needs plans (D-SNPS) that are applicable integrated plans (AIPs) as follows:
D-SNPs will be required to have integrated member ID cards for their Medicare and Medicaid plans
D-SNPs will be required to conduct an integrated health risk assessment for Medicare and Medicaid, rather than separate ones for each program.
These provisions affecting certain D-SNPS plans will be effective for the 2027 plan year.
Provisions Pertaining to the Medicare Part D Inflation Reduction Act
CMS is finalizing proposals to codify existing requirements related to key provisions of the Inflation Reduction Act, including no cost sharing for adult vaccines and capping monthly copayments for insulin at $35. In addition, CMS is codifying existing guidance related to the implementation of the Medicare Prescription Payment Plan, which is also part of the Inflation Reduction Act.
Key Proposals CMS Has Yet to Finalize
As noted earlier, CMS finalized a streamlined rule that excluded several regulatory changes identified in the November 2024 proposed rule. In addition to provisions related to coverage of anti-obesity medications, guardrails for AI, and mandatory analysis of the health equity impact of MA plans utilization management practices, the following proposals were not finalized. CMS notes that these proposals might be finalized in future rulemaking.
Expanding Medicare Part D Medication Therapy Management (MTM) eligibility criteria
Ensuring equitable access to behavioral health services by applying MA cost-sharing limits
Enhancing the Medicare Plan Finder to include information on plan provider directories
Promoting informed choice by enhancing CMS review of MA marketing and communication materials
Enhancing rules on MA plans’ use of internal coverage criteria
Key Considerations
The policies finalized in the CY 2026 Rate Announcement are projected to increase average Part C payments to MA plans by 5.06 percent in CY 2026—a significant uptick from the payment updates originally proposed in the CY 2026 Advance Notice. Nonetheless, the final rate increase will have varying effects across MA plans, with some experiencing larger or smaller impacts in CY 2026. MA plans should assess these outcomes as they prepare their bid submissions for 2026.
According to the CY 2026 Rate Announcement, CMS expects that the 5.06 percent increase will provide continued stability for the MA program and its beneficiaries while ensuring accurate and appropriate payments to Medicare Advantage organizations.
In the CY 2026 MA and Part D Final Rule, CMS adopted a significantly scaled-back final rule, which omitted some of the more far-reaching proposals for MA and Part D that were originally proposed in November 2024. CMS, however, could potentially revisit and finalize some of these proposals in future rulemaking. Moreover, new regulatory requirements that enhance enrollee protections in inpatient care settings and improving the care experience for dual eligibles signal CMS’s continued interest in improving program oversight and enhancing consumer protections for MA beneficiaries.
Connect With Us
MA stakeholders need to undertake scenario planning and be prepared to adapt to a rapidly evolving federal policy environment. From modeling and impact assessments of specific policy changes to strategy development and implementation, HMA is home to experts with diverse skill sets. Our team can help stakeholders assess and prepare for potential changes to prior authorization, looking holistically at their organization’s operations, patient care models, and reimbursement strategies. Our team also provides detailed modeling and assessments to ensure health plans are prepared for changes in risk adjustment and coding policies, supplemental benefits, and other key issues affecting capitation payment, bids, and care delivery models.
For details about the finalized payment and policy rules contact our featured experts below.
Medicare stakeholders are awaiting the imminent release of the Centers for Medicare & Medicaid Services (CMS) final Medicare Advantage and Part D rate notice and technical updates, as well as a final policy rule that establishes a significantly new direction for Medicare Advantage (MA) stakeholders. These final rules typically are released in April of each year.
In addition, the agency kicks off the annual cycle of payment rules for traditional fee-for-service Medicare, including the first wave of proposed rules that typically are released in April for the forthcoming payment year. These proposed rules for 2026 pertain to the following: Hospital Inpatient Prospective Payment System for Acute Care Hospitals, the Inpatient Rehabilitation Facility Payment System, the Home Health Payment System, and the Inpatient Psychiatric Facility Payment System. A second wave of 2026 proposed rules are typically released in July, including the Medicare Physician Fee Schedule and the Hospital Outpatient Prospective Payment System.
The MA rules and the first wave of Medicare Part A and Part B rules are highly anticipated regulations and now under review at the Office of Management and Budget. These rules are expected to be released in the coming days and weeks.
Why These Rules Matter
The rules set the rates for MA and reimbursement for a significant number of healthcare providers and facilities that serve Medicare beneficiaries. The rules also contain important information about CMS’s quality reporting programs and bonus payments and other changes required for Medicare stakeholders to ensure compliance.
What’s Different About 2025 Proposals
In the first year of a new presidential administration, CMS leaders have a limited window to include their policy priorities in the MA and Part D Final Rate Notice. CMS may, however, decline to finalize some or all of the prior administration’s proposals. Key issues that Health Management Associates (HMA), experts are watching for in the final rules include:
Whether CMS chooses to delay or not finalize significant policy changes proposed by the Biden Administration, including new requirements and guardrails around the use of prior authorization
Potential finalization of improvements to the Medicare plan finder
Direction on oversight of MA plan marketing activities
CMS decision and response to the proposal to expand coverage of anti-obesity medications under Medicare Part D and Medicaid
Similarly, in the first year of a presidential transition, CMS has a narrower opportunity to shape Medicare’s first set of proposed payment and policy rules. The agency may, however, begin to signal important policy direction on a global level and technical issues that can have an impact on Medicare stakeholders. HMA experts are watching in particular for requests for information and other signals of CMS’s Medicare priorities, including reforms in quality reporting, value-based contracting, pricing and contract transparency, among others.
Connect with Us
HMA’s expert consultants provide the advanced policy, tailored analysis, and operational skills you need to navigate today’s rapidly evolving regulatory landscape and to support implementation of final policies. Don’t let the uncertainty of future policies derail your strategic plans or burden your teams.
For details about the forthcoming Medicare Advantage and traditional Medicare regulations, contact one of our featured experts below.
This week, our In Focus section highlights insights from a new Health Management Associates (HMA), issue brief, “New Insights on Medicaid Spending: An Analysis of Disaggregated Managed Care Spending.” Until now, most Medicaid cost data have focused on enrollees in fee-for-service (FFS) programs. HMA used the Centers for Medicare & Medicaid Services (CMS) Transformed Medicaid Statistical Information System (T-MSIS) database to analyze Medicaid managed care organization (MCO) spending in major categories of healthcare, including inpatient and outpatient hospital care, physician and other professional services, skilled nursing facilities (SNFs) and home and community-based services (HCBS), clinics, pharmaceuticals, and other services. HMA’s methodology can be applied to all 50 states and allows us to determine prices for these services, which, combined with data on the number of encounters, yields reliable cost figures.
Findings
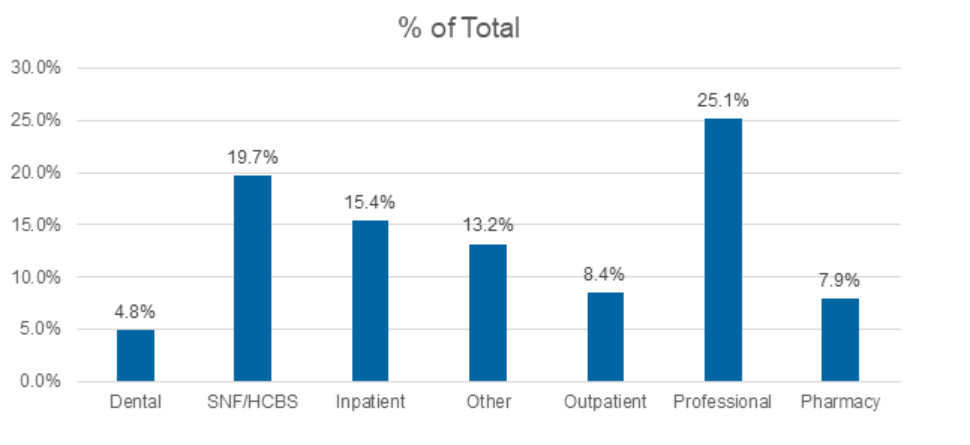
Medicaid managed care accounted for $420 billion of the total $717 billion in Medicaid spending for federal fiscal year 2021. Professional claims accounted for the largest portion of Medicaid spending, totaling 25.1 percent, followed by SNFs at 19.7 percent, and inpatient claims at 15.4 percent.
Figure 1. T-MSIS Medicaid Spending by Service Category 2021 (MCO Disaggregated plus FFS)
What’s Next
This analysis can be replicated for subsequent years and will provide important information on Medicaid spending trends. This work also sets the stage for analyses and comparisons of cost categories by variables such as eligibility category (e.g., dual eligibles, children, parents, adults without children, the Medicaid expansion population, and designated as aged/frail/disabled); race and ethnicity; frequent users of hospital services; and people with multiple chronic illnesses. This type of analysis allows us to answer fundamental questions about the Medicaid program and can pinpoint areas of high need within the Medicaid population, such as:
How much do we spend on services for people with diabetes?
How much do we spend during childbirth/first year of life and in the last year of life?
How much do we spend for Medicare-Medicaid dual eligibles?
Data-informed discussions on these and other topics can help identify opportunities for efficiencies and timely care management to slow the growth in total healthcare spending. This information will provide important context for the policy debate, offering a full view of the relative magnitude of the major categories of Medicaid spending.
Connect with Us
Medicaid providers, MCOs, states, and policymakers all have an interest in identifying high-cost drivers of Medicaid managed care. The methodology applied in the analysis for the HMA issue brief can be applied and adapted for future analysis.
For details about this analysis, its implications for state and local policies, and additional research using T-MSIS, contact our experts below.
The transition of MyCare Ohio to the Next Generation of its program on January 1, 2026, marks a significant evolution in the way Ohio provides healthcare services to its dual-eligible population – those who qualify for both Medicaid and Medicare services. This evolution moves Ohio to a Fully Integrated Dual Eligible Special Needs Plan model (FIDE SNP) that aims to achieve several key goals through a population health approach, designed to address inequities and disparities in care for dual-eligible individuals. These goals include:
Improved Care Coordination. Strengthening integration between Medicare and Medicaid services to provide seamless, holistic care for individuals, reducing fragmentation and ensuring comprehensive management of medical, behavioral, and social needs.
Personalized Care. Utilizing data analytics and technology to create more tailored care plans, with a focus on proactive care to address the unique health needs of each individual, especially those with chronic conditions.
Expanded Access to Services. Increasing accessibility, particularly through telehealth and digital tools, to reach underserved populations and improve convenience for patients, particularly those in rural or remote areas.
Enhanced Quality of Care. Shifting focus from service volume to outcomes, encouraging providers to deliver high-quality care and improve patient satisfaction, while incentivizing preventive care to reduce hospital admissions and other high-cost interventions.
Technology Integration. Leveraging advanced technologies like mobile apps, predictive analytics, and telemedicine to monitor patient health, improve communication between patients and providers, and enable more efficient care delivery.
The current MyCare program is offered in 29 counties across Ohio but will transition to a statewide program as a part of the Next Generation changes. Additionally, Coordination Only Dual Eligible Special Needs Plans (CO DSNP) will no longer be permitted.
After the Ohio Department of Medicaid (ODM) publicly released the request for applications (RFA) and evaluated submitted proposals, they selected four Managed Care Organization (MCOs) that will become the Next Generation MyCare plans. The ODM awarded the following MCOs to serve MyCare members beginning in January 2026: Anthem Blue Cross and Blue Shield, Buckeye Health Plan, CareSource, and Molina HealthCare of Ohio.
The shift to the FIDE SNP model and selection of four participating health plans will have a considerable impact on the competitive landscape for Medicare and Medicaid managed care in Ohio. The resulting changes can affect both selected and non-selected participants in different ways, including:
Increased competition among chosen MyCare MCOs. MCOs will need to focus on enhancing their care coordination systems, adopting new technologies, and developing personalized care plans to compete not just on the volume of services provided but also on the quality and effectiveness of care. Those who can best integrate services, offer proactive care management, and improve patient outcomes through value-based care and advanced technology initiatives will gain the competitive advantage, potentially attracting more beneficiaries.
Strategic responses of nonparticipating MCOs to counter potential membership and financial losses. MCOs that lose membership by not being selected, or are unable to offer CO DSNPs moving forward, will likely strategize how to gain membership through other product lines or benefit design to offset losses. Strategies may vary but could include tactics such as enhancing benefits or decreasing member cost shares to entice member movement across carriers for non-DSNP plans; finding innovative ways to further reach different segments within the Medicare population, such as Value Based Insurance Design (VBID) packages or Chronic SNP plays; or shifting focus to product lines outside of Medicare Advantage and Medicaid.
Ohio is one of many states transitioning to a FIDE model beginning January 2026. Health Management Associates (HMA) has successfully supported participating and non-participating carriers throughout the transition process and continues to be a dedicated partner to organizations navigating Medicare and Medicaid changes across the country. Contact one of HMA’s many experts for more details on how to navigate this evolution in health care.
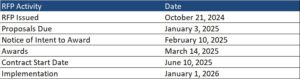
This week, our In Focus section highlights the State of Nevada’s October 21, 2024 request for proposals (RFP), which will expand Medicaid managed care to cover nearly all populations in all counties. The Department of Health and Human Services’ Division of Health Care Financing and Policy (DHCFP) estimates that the expansion statewide will cover 75,000 additional individuals who live in rural areas, including children, parents, and adults without children. The expansion to rural areas in all counties presents new opportunities and critical issues for managed care plans, ensuring that they meet the needs of rural populations effectively.
Background
In 2024, Nevada covers 788,000 Medicaid members, with risk-based capitated Medicaid managed care making up about 75 percent of the total Medicaid population. Managed care covers traditional Medicaid and expansion, the Children’s Health Insurance Program (CHIP) known as Nevada Check Up, and children who have aged out of foster care. Enrollment in an MCO is mandatory for these populations. Currently, Medicaid managed care is only offered in the urban Washoe and Clark counties, which include cities such as Reno and Las Vegas.
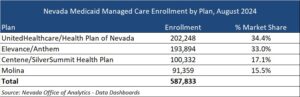
Nevada has four MCOs that were procured in 2021: Centene/SilverSummit HealthPlan, Elevance/Anthem, Molina, and UnitedHealthcare/Health Plan of Nevada. These MCOs serve approximately 588,000 beneficiaries in Urban Washoe and Urban Clark counties as of August 2024.
United and Elevance make up the majority of market share by enrollment, with 34.4 percent and 33 percent respectively.
Individuals who receive Medicaid through fee-for-service (FFS) are Medicaid-enrolled children in foster care, juvenile justice, and child welfare systems; individuals with disabilities; seniors; and individuals receiving services through one of the three 1915 home and community-based waiver programs. These individuals will continue to receive services through FFS.
RFP Highlights
The RFP describes the state’s three managed care service areas (SA): Urban Washoe, Urban Clark, and Rural. The Rural SA will include all other counties in Nevada in addition to the rural areas of Washoe and Clark counties.
MCOs must bid on all service areas. DHCFP anticipates selecting four plans. The two awarded vendors with the highest rural care score will operate in all three SAs. The remaining awarded vendors will operate in Urban Clark and Urban Washoe SAs. The state has the option to award a fifth contract to an MCO to operate in the Urban Clark SA only.
The RFP focuses on rural care and policies designed to improve outcomes and access to care, reduce burdens for providers to participate, and simplify administrative tasks for the state. MCOs will need to show their understanding of the unique challenges facing rural providers. They will describe their approach for provider outreach, contracting, and provider training strategies in rural areas, with a focus on primary care, maternal and child health, and behavioral health. Due to the geographic limitations, telehealth will also play a strong role. MCOs will need to address limitations such as access to internet and provide an approach to help members access telehealth. Additionally, MCOs will need to provide their experience in managing non-emergency medical transportation (NEMT) in rural areas and describe an approach for establishing and maintaining a network of transportation providers in these remote areas.
MCOs also will be required to offer at least one Silver and one Gold Qualified Health Plan (QHP) on Nevada Health Link Marketplace by the 2026 coverage year. The state expects this contractual requirement will help reduce churning and improve continuity of care for individuals and families who have a change in eligibility status.
MCOs must also contract with providers that use alternative payment methodologies (APMs), and plans will need to outline value-based purchasing (VBP) strategies within their proposals. APM contracting strategies must support priority areas such as addressing health-related social needs (HRSNs) and improving health equity, access, behavioral health, and maternal and child health outcomes. APM contracting strategies must include quality measures in the payment methodology and outline reporting and estimated financial details. Additionally, MCOs are required to develop a Population Health Program, so proposals must outline how it will leverage specific APMs to meet the program’s goals.
Evaluation
MCOs will require a minimum score of 945 points (out of 1,350 points) on the Technical Proposal to be eligible to win a contract. The Building Provider Networks and Access to Care technical questions is worth the most points, 450, while 300 points are available under the Rural Care and Service Area Expansion section. The table below provides a breakdown of the Technical Proposal Scoring.
The state assigns the highest number of points to the section addressing provider networks and access to care followed by the section addressing rural care and service area expansion.
Timeline
Key Considerations
HMA experts identified the key considerations for MCOs, partners to MCOs, providers who will furnish services to members, and other interested stakeholders.
The Building Provider Networks and Access to Care Rural Care and Service Area Expansion sections together are worth 750 points, most of the minimum needed, and more than half of the total available points. This is a strong indicator of that MCOs need to demonstrate capacity and innovation to ensure access to members using multiple strategies. Ensuring a robust network of healthcare providers in rural areas is crucial. This includes recruiting and retaining providers who are willing to serve in these regions.
In this RFP, DCHFP is evolving its value-based payment (VBP) initiatives and expectations for MCOs. The VBP strategies are intended to enhance care quality, improve patient outcomes, and ensure the sustainability of the Medicaid program. MCOs will need to design these models and successfully work with providers to implement the strategies and models.
Both improving maternal and child health outcomes and addressing mental health and substance use disorders are priorities for the state. These can be more challenging in rural settings due to limited access to specialized care and will require rural specific solutions.
Changing the Medicaid delivery system model in some rural areas may create the need for building awareness and understanding for the changes that come with this transition. MCOs should be prepared to effectively address the issues of equity and disparities that are present in in rural communities.
Connect with Us
HMA’s experts understand the Medicaid managed care environment and specific issues presented by rural areas. We work with clients to address the multilevel challenges for delivery of quality healthcare and social services to rural populations, and the workforce concerns they create. We identify and help plan for access issues such as lack of services, transportation difficulties, and socio-economic barriers. HMA knows the difficulties that often keep rural providers and organizations from achieving their full potential to serve and support their communities’ need and help Medicaid clients in rural areas in states around the country to solve these difficult problems.
Read more about the work we are engaged in with a range of healthcare industry leaders focused on rural and frontier areas.
The report, released in August 2024 with support from Arnold Ventures, includes survey responses from 47 states (including DC) for state fiscal years (SFYs) 2023 and 2024. The survey instrument builds on questions posed in the 2019 Medicaid Pharmacy Study of all 50 states and the District of Columbia, which HMA and the Kaiser Family Foundation conducted.
The report discusses state trends for how Medicaid pharmacy benefits are administered across the country, including planned priorities and anticipated challenges in SFY 2025 and beyond. The findings are based on information provided by the nation’s state Medicaid Directors, Medicaid Pharmacy Directors, and other Medicaid agency experts.
Pharmacy Benefit Administration
In many states, managed care delivery systems play a pivotal role in administering Medicaid benefits, including prescription drugs. As of July 1, 2023, survey results found that:
A total of 33 states carved pharmacy benefits into managed care organization (MCO) contracts, with one state, Kentucky, directing its MCOs to use a single state-selected pharmacy benefit manager (PBM).
Eight states carve-out the pharmacy benefit—double the number in 2019.
MCO states were surveyed about their use of carve outs for certain drug products/classes, inclusive of physician-administered drugs covered under the medical benefit.
In all, 19 states reported carving out one or more drug classes or select agents within a drug class—often high-cost specialty drugs.
Of those states, 13 reported using the carve-out as part of a risk mitigation strategy.
Pharmacy Benefit Managers
The significant role and market power of PBMs have prompted many state legislatures to enact greater transparency practices and require health plans to accept more responsibility for monitoring the PBMs they contract with, which reflect notable changes since the 2019 survey. More specifically:
A total of 33 states reported contracting with a PBM.
The most frequently reported PBM functions included utilization management, drug utilization review, claims processing and/or payment, and rebate administration activities.
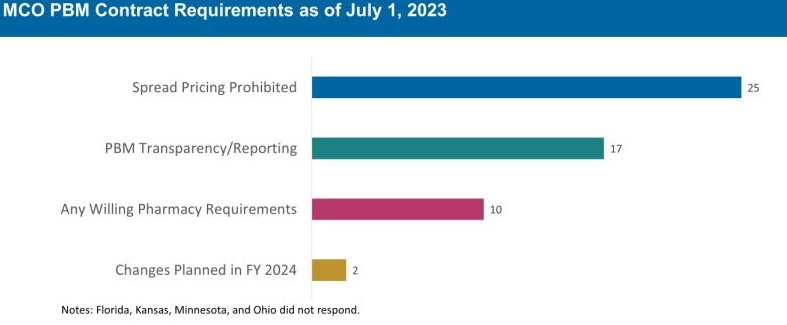
The 30 MCO states that carve in pharmacy benefits responded to survey questions about PBM transparency and spread pricing requirements. Of these states:
25 prohibit spread pricing in MCO PBM contracts—more than double the number of states reporting prohibitions on spread pricing in 2019.
17 reported having PBM transparency reporting requirements.
10 states reported having “any willing” pharmacy requirements.
The Role of PDLs, Prior Authorization, and Step Therapy in Controlling Drug Costs and Utilization
HMA’s experts also sought information on state payment strategies and utilization management protocols that are used to manage pharmacy expenditures. Nearly all responding states (44) have a preferred drug list (PDL) in place for fee-for-service prescriptions, which allow states to drive the use of lower cost drugs by encouraging providers to prescribe preferred drugs. Further, nearly two-thirds of responding MCO states (19 of 30 states) that do not carve out the pharmacy benefit reported having a uniform PDL for some or all drug classes, requiring all MCOs to cover the same drugs.
Many states have implemented step therapy and prior authorization (PA) guardrails in their Medicaid programs through legislation. However, 85.1 percent of responding states (40 of 47) report utilization controls like PA or step therapy applied to drugs that are reimbursed through the medical benefit to control utilization and costs. States also play an active role in managing MCO clinical protocols or medical necessity criteria, with 22 out of 30 MCO pharmacy carve-in states reporting that they require uniform clinical protocols for some or all drugs with clinical criteria. Approximately one-half of responding MCO carve-in states also require review and approval of MCOs’ PA criteria (15 of 30 states) and step therapy criteria (14 of 30 states).
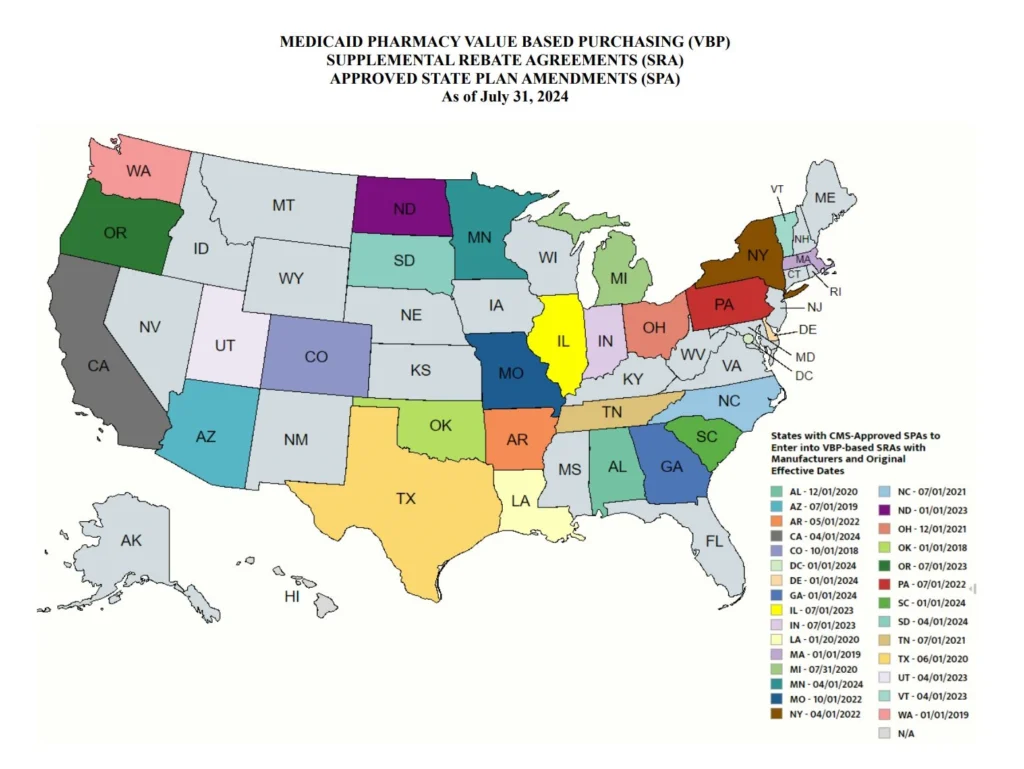
State Adoption of VBAs: Improving Patient Access to Cell and Gene Therapies
A growing number of states are actively considering entering into value-based arrangements (VBAs) with manufacturers, as pressure to improve patient access to cell and gene therapies increases. Nine states have at least one VBA in place, and 23 states reported that VBAs are among their future solutions for addressing coverage of new high-cost therapies. States will need to address common barriers to VBA implementation, which involves more upfront costs and operational challenges to implement than traditional contracts.
Subsequent to the submission of survey responses, the Centers for Medicare & Medicaid Services (CMS) released a Cell and Gene Therapy (CGT) Access Model, which begins with a focus on sickle cell disease, anticipated to go live on January 1, 2025. Under the model, CMS will negotiate outcomes-based agreements with manufacturers on behalf of the state to ensure that treatment pricing is related to treatment effectiveness. In the coming years, experiences with this model will help determine whether a CMS-led approach to developing and administering VBAs for CGTs improves Medicaid member access to innovative treatment and their impact on expenditures, if any.
Managing the Medicaid pharmacy benefit has never been more challenging. In FY 2025 and beyond, most states will be focused on managing their Medicaid pharmacy budgets, especially the development of VBAs and other policies and strategies for managing new high-cost therapies. Other top priorities and challenges cited by multiple states include management of PBM arrangements and considering coverage of the new generation of GLP-1 anti-obesity medications. States also must react to changing drug marketplace conditions driven, in part, by federal policy changes to the Medicaid drug rebate formula and changes designed to lower Medicare drug costs. Drug manufacturer responses to these changes have implications for Medicaid state budgets, but also for state PDL management decisions and beneficiary access to needed medications.
Connect with Us
The upcoming event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, hosted by HMA, will offer more opportunities to engage with report author Kathy Gifford at the pre-conference workshop Paying for Innovative Pharmaceuticals: State and Federal Trends Shaping Public Programs. Leaders from various sectors will join Kathy to discuss trends in prescription drug policies in public and commercial insurance programs.
For details about the report, contact our featured experts below.
HMA works with managed care plans to maximize Star ratings and improve program quality.
Star Ratings have been on a steady decline over the last two years resulting in large reductions in quality bonus and rebate payments, potentially impacting opportunities to improve member health outcomes.
How HMA can help improve a plan’s Star rating:
We have developed a playbook that captures The HMA Stars Accelerator Solution with proven strategies for Stars improvement based on our diverse and extensive expertise in managed care plan (MCP) operations, MCP strategy, performance improvement, actuarial science, data analytics, risk adjustment, and federal and state policy.
Using our vast experience in the Medicare and Medicaid space, HMA can help you maximize ratings in programs like Medicare Stars and Medicaid quality performance. Together with our actuarial colleagues from Wakely Consulting Group and federal policy expert colleagues from Leavitt Partners, both HMA companies, we can provide the assistance you need to move your organization to a higher Star rating level. With guidance from HMA experts, the Accelerator is scalable for both functional and matrix organizations.
Want a copy of HMA’s Stars Accelerator Playbook?
Fill out this form and one of our consultants will get back to you.
HMA can help your organization create momentum by combining HMA’s programmatic strategies with a robust actuarial and analytical basis, inclusive of integrated risk adjustment.
Meaningful data analysis ensures plans can prioritize the most important areas for strategic focus. Improving performance in Stars requires a multi-pronged, multifactorial approach. The HMA Stars Accelerator Solution is consumer-oriented and customizable to meet the unique needs of your members’ needs. It facilitates understanding of the organization’s current state, identifies opportunities for improvement, provides best practices for design of meaningful solutions to implement, and measures the effectiveness of improvements.
Why is a high Star rating important for a health plan?
The Centers for Medicare & Medicaid Services (CMS) publishes the Medicare Advantage (Medicare Part C) and Medicare Part D Star ratings each year to measure the quality of health and drug services received by consumers enrolled in Medicare Advantage (MA) and Prescription Drug Plans (PDPs or Part D plans). Star ratings impact a managed care plan’s financial performance, competitiveness, growth, and member retention. They are based on measures of multiple aspects of plan performance including:
Member experience and satisfaction
Administrative performance
Medication safety and/or adherence
Hospital readmissions
Healthcare Effectiveness Data and Information Set (HEDIS) and Health Outcomes Survey (HOS), both of which measure performance improvement.
Contracts are rated on a scale of one to five stars (rounded to nearest half star) based on approximately 45 measures related to preventive care, member experience (health plan customer service, physician point of service care, and perceived health), prescription drug monitoring, health plan operations, etc.
The industry has meaningfully improved traditional quality metrics (e.g. preventative care and medication adherence rates). As performance peaks in those measures, CMS is placing increasing emphasis on the member experience with their health plan and their providers during care.
Plans with 5 stars can market year-round.
The marketing advantage is a distinction for a high rated plan.
Poor performers (under 3 Star rating for 3 years) receive a Poor Performance Icon and may not be able to renew with CMS.
In 2024 there were 29 Part C (Medicare Parts A & B) and 11 Part D (Pharmacy) measures, and they can change every year. CMS recently released plan preview Star performance data for health plans to review. Final scores and Star ratings will be released by CMS in early October 2024 for Star Year 2025 based upon 2023 dates of service.
Star Rating High Level Timeline
CMS Star Ratings are a lagged pay-for-performance system. For 2026 Star Ratings, 2024 and early 2025 performance timeframes are critical to success, even though payments for this performance will not be received until 2027.
What plans do in 2024 and 2025 impacts your 2026 Star rating which will affect your plan’s revenues in 2027.
Is your plan building a strategy for next year based upon underperforming measures? Are you looking for ways to lean in on any remaining Consumer Assessment of Healthcare Providers and Systems (CAHPS) and HOS opportunities? Do you know where to start?