HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
HMA’s webinar series, 1115 Medicaid Justice Demonstration Waivers: Bridging Healthcare, focused on helping stakeholders optimize the continuity of care for persons in carceral settings and during their transition back to the community.
Part 3 focused on optimizing key partnerships before, during and after transition from a carceral setting into the community to ensure the best outcomes for individuals eligible for 1115 approved waiver services.
Learning Objectives:
Health Assessments and Transition Planning: Understand the health and resource needs of returning citizens (health, behavioral health and social issues).
Collaboration with Community Providers: Identify key partners and formalize collaborations to strengthen the quality of transitions care and support provided to individuals transitioning to the community.
Insurance Enrollment Strategies: Develop Medicaid enrollment strategies that apply to your state and local framework.
Other webinars in this series:
Watch a replay of Part 1: Medicaid Authority and Opportunity to Build New Programs for Justice-Involved Individuals
Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth
Pre-Conference Workshop: October 29, 2023 Conference: October 30−31, 2023 Location: Fairmont Chicago, Millennium Park
Health Management Associates has announced the preliminary lineup of speakers for its sixth annual conference, Innovations in Publicly Sponsored Healthcare: How Medicaid, Medicare, and Marketplaces Are Driving Value, Equity, and Growth.
Hundreds of executives from health plans, providers, state and federal government, investment firms, and community-based organizations will convene to enjoy top-notch content, make new connections, and garner fresh ideas and best practices.
A pre-conference workshop, Behavioral Health at the Intersection of General Health and Human Services, will take place Sunday, October 29.
Confirmed speakers to date include (in alphabetical order):
Jacey Cooper, State Medicaid Director, Chief Deputy Director, California Department of Health Care Services
Kelly Cunningham, Administrator, Division of Medical Programs, Illinois Department of Healthcare and Family Services
Karen Dale, Chief Diversity, Equity, and Inclusion Officer, AmeriHealth Caritas
Peter Lee, Health Care Policy Catalyst and former Executive Director, Covered California
John Lovelace, President, Government Programs, Individual Advantage, UPMC Health Plan
Julie Morita, MD, Executive Vice President, Robert Wood Johnson Foundation
Anne Rote, President, Medicaid, Health Care Service Corp.
Drew Snyder, Executive Director, Mississippi Division of Medicaid
Tim Spilker, CEO, UnitedHealthcare Community & State
Stacie Weeks, Administrator/Medicaid Director, Division of Health Care Financing and Policy, Nevada Department of Health and Human Services
Lisa Wright, President and CEO, Community Health Choice
Publicly sponsored programs like Medicare, Medicaid, and the Marketplaces are leading the charge in driving value, equity, and growth in the U.S. healthcare system. This year’s event will highlight the innovations, initiatives, emerging models, and growth strategies designed to drive improved patient outcomes, increased affordability, and expanded access.
Early bird registration ends July 31. Questions may be directed to Carl Mercurio. Group rates, government discounts, and sponsorships are available.
HMA is pleased to welcome new experts to our family of companies in April 2023.
Jed Abell – Consulting Actuary Wakely
Jed Abell is a professional health insurance actuary with over 20 years of experience focusing on Medicare Advantage, Part D, and commercial employer group plans.
Surah Alsawaf – Senior Consultant HMA
Surah Alsawaf is a senior consultant with experience in creating and implementing regulatory strategies and workflows, conducting reviews and audits, and leading cross-functional teams to complete complex deliverables.
Elrycc Berkman – Consulting Actuary Edrington
Elrycc Berkman is experienced in Medicaid managed care rate development including managed long-term services and supports (MLTSS) and program of all-inclusive care for the elderly (PACE) rate development.
Monica Bonds – Associate Principal HMA
Monica Bonds is an experienced managed care professional with over 15 years of experience working in large and diverse organizations.
Yucheng Feng – Senior Consulting Actuary Wakely
Yucheng Feng has over 15 years of experience providing actuarial support for Medicare Advantage clients, including bid preparation, reserve, actuarial analytics and providing strategic recommendations. Read more about Yucheng.
Melanie Hobbs – Associate Principal HMA
Melanie Hobbs is an accomplished healthcare executive, consultant, and thought leader specializing in Medicare, Medicaid, and Special Needs Plans (SNPs).
Daniel Katzman – Consulting Actuary Wakely
Daniel Katzman is experienced in Medicare Advantage bid pricing and modeling as well as claims trend analytics and affordability/cost-savings analysis. Read more about Daniel.
Supriya Laknidhi – Principal HMA
Supriya Laknidhi has over 20 years of experience in the healthcare industry and a proven track record in driving growth and innovation for companies.
Donald Larsen – Principal HMA
Dr. Donald Larsen is a C-suite physician executive with over 30 years of experience spanning complex academic medical centers, community health systems, acute care hospitals, and research institutes.
Ryan McEntee – Senior Consultant Wakely
Ryan McEntee is an experienced managed care executive specializing in strategic leadership within Medicare Advantage plans. Read more about Ryan.
Nicole Oishi – Principal HMA
Nicole Oishi has over 30 years of experience in senior leadership roles as a healthcare clinician and executive.
This is part of an ongoing series highlighting efforts in Human Services and Family Wellbeing.
During the month of May, National Foster Care Month provides an opportunity to raise awareness on issues related to foster care and to celebrate those who are dedicated to serving our children, youth, and families. Yet it is important to note that unfortunately issues surrounding children and youth experiencing foster care are not limited to one month a year. As noted in our recent child well-being blog, Child welfare services face challenges every day to prevent, treat, and reduce risk of maltreatment, neglect, trauma, housing instability, and violence in communities. All these issues contribute to the significant number of children and youth who enter or remain in the foster care system. These issues are year-round and decades in the making. They need to be seen as a priority for public health and community wellbeing and not just the jurisdiction and responsibility of child welfare agencies.
To positively impact the number of children and youth experiencing foster care, there are some strategies that can be implemented now to promote change:
We must meaningfully elevate the voices of those with lived experience to help us design systems that meet their needs. For foster care, working to hear and understand the voices of youth based on how they have experienced foster care will help create opportunities to improve the system from those most impacted. Further, the meaningful elevation of these voices helps to ensure their input is not contributing towards tokenism and re-traumatization.
Multi-system involvement is important. We can work together to enhance access, increase prevention-oriented services, improve community health, and well-being, and achieve better outcomes using an equity lens, but proposed system reforms cannot be successful without shared ownership within the community and across government agencies. This requires building a responsive and integrated system of care approach to allow communities to seek solutions with the necessary support of the highest leadership within their organizations.
Continue to find ways to assure that mandated reporters and staff who work within child welfare understand that poverty is not neglect, and poverty alone should not be a reason children and youth are removed from their home(s).
System redesign is needed. From front end reporting and assessment, to working with court systems, to building up networks of caring service providers, each component of the current child welfare system and human services partners can strive to find areas needing improvement and collectively change the experiences for children and youth engaged in the child welfare system.
Focus on mental health. This year’s theme from the Children’s Bureau for national foster care month is “Strengthening Minds, Uplifting Families” and is dedicated to supporting children and youth mental and behavioral health as the largest unmet need related to foster care. According to the Children’s Bureau, Up to 80 percent of children experiencing foster care have significant mental health issues, compared with approximately 18 to 22 percent of the general population.[1]
HMA can help public sector and community partners align themselves to improve and develop new delivery systems that will work to address inequalities and disparities as communities strive to meet the needs of children, youth and families impacted by issues like mental health and substance use disorder, domestic violence, child abuse and neglect, food insecurity, housing instability, incarceration and other traumas that impact them greatly.
HMA can help support foster care prevention or reunification program efforts in the following ways:
Creating additional human service system integration of prevention services to help support families and youth experiencing child welfare interventions or foster care.
Increasing Medicaid providers who offer more Evidenced Based and Informed Practices (EBP) among Community Based Organizations (CBO), Providers, and Local Government.
Supporting Managed Care Organizations to develop programs specifically designed to support the wellbeing of children and youth in the foster care system and their families.
Connecting the Family First Prevention Services Act (FFPSA) & Medicaid funding together to ensure that funding supports the need and enhance service implementation.
Working to implement School Based Mental Health programs in communities. We can help convene stakeholders, create process flows, and support the development of sustainable funding for such programs.
Increasing the meaningful use of youth voice for true collaboration in system redesign.
Enhancing judicial engagement with the child welfare system in a way that supports meaningful youth and family voice and representation in court while maintaining the child welfare system’s responsibilities around assuring child safety. Making the court process less traumatic for children and youth and more part of a solution for them will support better outcomes.
Recognizing longstanding racial inequities in foster care experiences that can and should be addressed holistically in communities and supporting efforts to understand the root causes for the disparities in foster care placement.
If you have questions on how HMA can support your efforts in Child and Family Wellbeing, please contact: Uma Ahluwalia, MSW, MHA, Managing Principal, John Eller, Principal, Jon Rubin, Principal, or Nicole Lehman, Senior Consultant.
[1] Data: National Foster Care Month Outreach Toolkit | Child Welfare Information Gateway
The public health workforce is in the midst of a crisis, dealing with staff shortages, accelerated retirements and unfilled positions.
The current climate was exacerbated by Covid-19, but many challenges began long before 2020’s pandemic. The public health system underwent a significant contraction following the Great Recession in 2008-2009, losing more than 40,000 positions in state and local governments across the country. While some of those positions were regained with Covid-19 funds during the pandemic, recruitment, diversity and retention remain as challenges, especially for hard to fill positions in nursing and epidemiology. Public health staff report high rates of burnout due to the Covid-19 response and the political climate that resulted, including suffering symptoms of post-traumatic stress disorder. It is likely that there will be staff shortages for the foreseeable future, increased retirements, and departures to other parts of the healthcare industry competing for skills with higher compensation.
New Funding Streams Available
State and local health departments have been receiving significant amounts of one-time money, including the Centers for Disease Control and Prevention (CDC) recent allocation of $3.5 billion specifically for governmental public health efforts.
Health Resources and Services Administration (HRSA) has created a new workforce research center for public health. The AmeriCorps program has developed a specific public health component. These new initiatives were designed to build and support the workforce in governmental public health. As state and local health departments receive or apply for these various sources of workforce development funding, HMA can provide existing technical assistance and training to minimize inefficiencies and duplication of efforts that might be created by a fragmented approach across state and local units of government developing independent approaches to the utilization of WFD funds.
HMA Workforce Expertise
The public health group at Health Management Associates (HMA) is made up of more than 100 colleagues with expertise in public or population health improvement, experienced working with national, state or local organizations seeking to improve public health outcomes. If your organization is looking to improve your public health workforce efforts, it is important to utilize expertise and consolidate efforts across the country so each unit of government is not “reinventing the wheel.” HMA can help multiple organizations in developing plans and coordinating processes for recruiting, training and development of the public health workforce.
HMA understands the skills that are needed to achieve high-performing public health and accountable care. Our expertise developing workforce within safety net delivery systems and accountable care organizations involve transferrable skills for the current challenges in building and developing the public health workforce. We have expertise in recruiting and are creating new training and retraining methods to meet the needs of public health teams, accountable care organizations, graduate medical education, nursing education, learning collaboratives, online training and team simulation training. We understand the care coordination, care management and IT support systems needed to backstop the workforce and meet quality and equity goals.
This week our In Focus section reviews the Illinois Healthcare Transformation 1115 Waiver Extension request, posted for review on May 12, 2023.
In pursuing this waiver extension, Illinois joins a growing list of states taking advantage of new Centers for Medicare & Medicaid Services (CMS) policy flexibilities to address health-related social needs (HRSNs) through Medicaid and test community-driven initiatives that are focused on improving health equity, improving access to care, and promoting whole-person care.
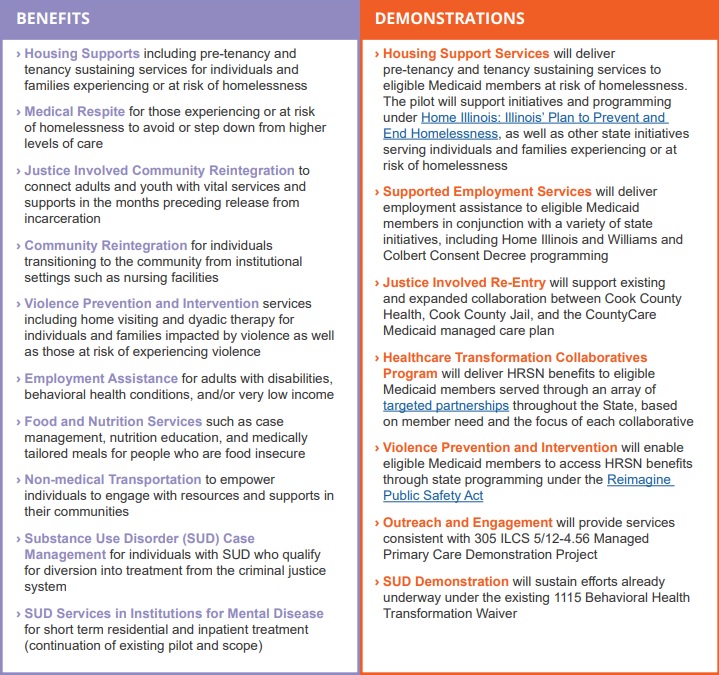
The Illinois waiver incorporates two of the most significant new opportunities in the CMS demonstration waiver flexibilities by proposing to incorporate housing supports for people who are experiencing or at risk of homelessness. The waiver also would extend community reintegration services for justice-involved adults and youths for up to 90 days before their release from incarceration. For a full list of proposed benefits and demonstrations, see Table 1.
Table 1. Summary of Illinois Medicaid 1115 Waiver Extension
The Illinois waiver represents an unprecedented opportunity to demonstrate the long-term, positive impact of providing HRSN services to achieve health equity and create a sustainable, community-driven system for delivering those services. The demonstration proposes to offer a range of HRSN services that are focused on the unmet needs of people who are homeless and housing insecure, are justice-involved, have behavioral health conditions, are pregnant, are unemployed, are food insecure, and/or have been exposed to violence or are at risk of violence with the goal of eliminating health disparities.
The waiver projects a five-year total of $4.4 billion in HRSN services expenditures and another $800 million in HRSN-related infrastructure, indicating Illinois’ long-term commitment to healthcare transformation and to building an equitable, accessible, and high-quality delivery system.
Healthcare executives gathered with HMA leaders in March to learn and share about new initiatives in quality improvement. Panels and discussions were led by esteemed experts, who provided important insight into the multitude of opportunities to improve quality and equity:
From the Experts: CMS has doubled down on its commitment to improve healthcare quality, equity, and access.
The HMA Point of View: Current leadership in Washington has set very clear goals to improve health equity, aligning federal policy as a lever to improve healthcare outcomes. Federal dollars passed along to states are including new rules and objectives to improve quality in an equitable manner. Therefore, those applying for federal contracts and grants must include a strategy to improve quality, equity, affordability, and access.
From the Experts: Interventions need to be robustly evaluated to address equity and social determinants of health (SDOH).
The HMA Point of View: Governments, care providers, and payers have been experimenting with approaches to SDOH, but the bar is now higher and results have to be measurable. New investments that address SDOH and aim to improve equity must include a strategy to measure and analyze results of interventions, including evaluation of critical subpopulations to address disparities. Although experiments will continue, we have reached the point where a robust analysis of outcomes is an expectation.
From the Experts: Quality is playing a central role in operationalizing equity.
The HMA Point of View: While there are many reasons for disparities in health, quality metrics and programs must be designed to improve quality for all patients. Identifying inequities is only the first step; successful programs will advance equity by reducing barriers to care. Measurable quality programs should be designed for population health, but personalized for individuals with clear provider incentives to not only identify disparities but also minimize them. Quality is the tool by which we achieve health equity.
From the Experts: We are on the precipice of doing great things in quality.
The HMA Point of View: Our ability to integrate data from multiple sources is finally getting to a place where patients can get the quality care they need, and providers can give the right care at the right time to improve outcomes. Policymakers have broken down barriers to data sharing, enabling a new economy of information sharing that promises to empower patients and reduce costs. It is no longer enough to have a separate IT or data strategy; anyone working to improve healthcare quality needs to have data strategies within and across every operational function across their organization.
From the Experts: Being rewarded for doing what’s right for the patient is central to continuous quality improvement.
The HMA Point of View: Quality care for the patient means creating the right incentives for payment and care delivery that focus on outcomes and experience. Every point of care in the patient’s health journey needs to be evaluated and designed from the point of view of providing a quality experience. Not every patient has the same journey, and our healthcare system must meet them where they are, delivering for their unique needs. Convenience, personalization, accuracy, simplification, and affordability are nearly as important as clinical outcomes in the mind of most patients and addressing barriers to health can have clinical benefits.
HMA has a long history of working with clients to achieve their quality improvement goals including securing accreditation for both payer and provider organizations, driving clinical practice transformation, and improving the overall value of care. We strongly believe that there is no quality without equity, access, and measurement, and are investing in people and resources to support these needs. Together we are working with clients to advance value-based care, develop programs demonstrating quality, value, and equity in behavioral health, and implement new quality and accreditation programs to better serve their communities.
Learn more about HMA’s continuing work in quality and accreditation and join the conversation on LinkedIn and Twitter using #HMAtalksQuality.
This week’s In Focus is the second in a two-part look at the Centers for Medicare & Medicaid Services’ (CMS’s) recently proposed changes to the Medicaid program. Last week we covered CMS’s proposed changes to the federal Medicaid managed care regulations (CMS-2439-P). This week we review the Medicaid Access to Care proposed rule (CMS-2442-P).
As we discussed last week, the managed care and access to care rules include significant changes to core structural and financing aspects of the Medicaid program. Though state agencies, providers, health plans, consumer groups, and other stakeholders will want to understand the distinct requirements and expectations in each rule that apply to them, the proposed changes cannot be viewed in isolation.
The Access to Care rule addresses a range of challenges that shape the experience of Medicaid enrollees, regardless of whether they are in managed care programs or traditional fee-for-service (FFS). The proposed policy changes also are designed to create an updated federal framework for Medicaid’s home and community-based services (HCBS) programs. These proposals come at a pivotal time, as states are facing workforce shortages, particularly among HCBS direct care workers (DCWs).
The remainder of this In Focus delves into notable components of the proposed changes and includes analysis of the implications of these policies for stakeholders. CMS will benefit from stakeholder input; the deadline for submitting comments is July 3, 2023.
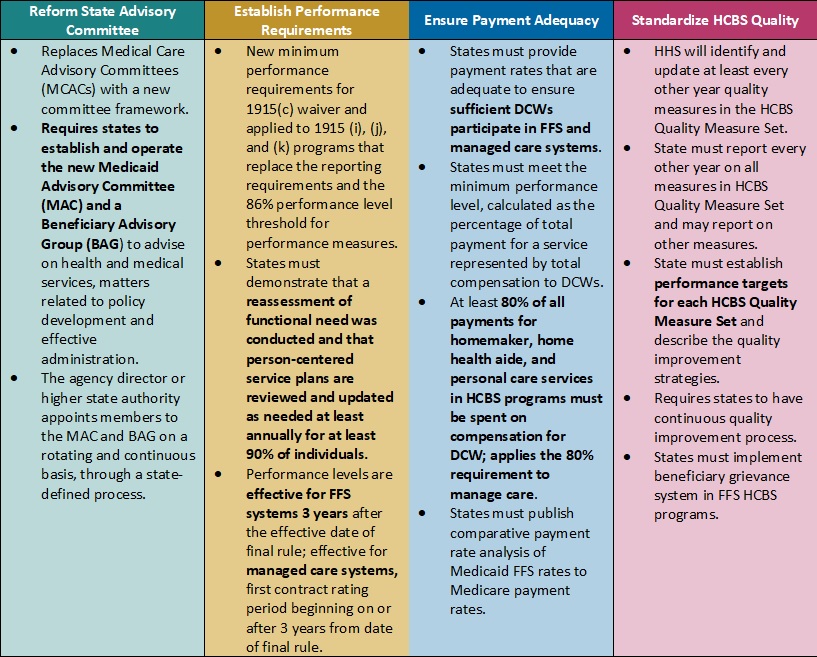
Table 1. Access to Care Regulations: Overview of Proposed Changes
Key Themes and Considerations
Ensuring Payment Adequacy for Key HCBS Services Experiencing Workforce Shortages. One of the most notable proposed changes that would directly impact DCWs is a requirement that at least 80 percent of Medicaid payments be spent on compensation. The proposed rule would apply to homemaker, home health aide, and personal care services, as they represent a large portion of HCBS services that DCWs provide. The proposal is based on feedback from states that have implemented similar provisions, which have ranged from 75 to 90 percent compensation requirements.
CMS specifically seeks stakeholder feedback on the percentage that should be adopted. This policy provision also is important from an equity perspective, given that 90 percent of DCWs are women and 60 percent are members of racial or ethnic minority populations. However, increased or mandated DCW rates may make it difficult for HCBS providers to sustain their businesses as they manage the increased administrative pressures of electronic visit verification, the complexity of filing claims for managed long-term services and supports (MLTSS), and the additional work that HCBS quality measurement may create. Smaller HCBS providers, some of which may have deep cultural expertise, may struggle to sustain themselves and meet these requirements.
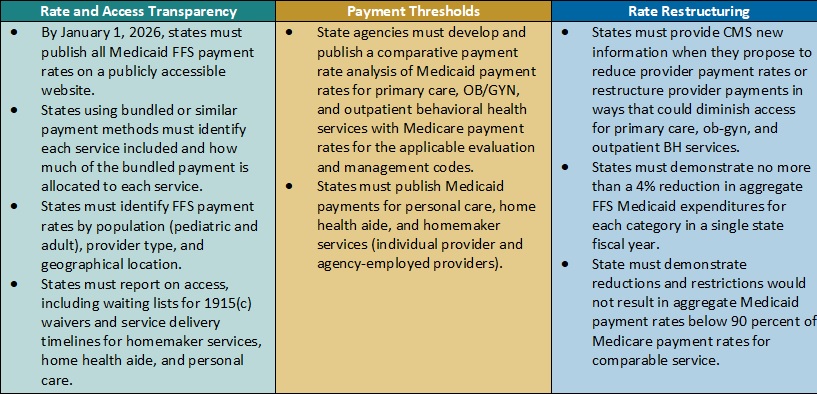
Table 2. Access to Care Regulations: Snapshot of Proposed Rate, Access, and Payment Changes
Payment Alignment. CMS is seeking to align access to care strategies and payment rate transparency more closely across the FFS and managed care delivery systems. The proposed rule includes several changes that CMS has developed achieve this goal. For example:
CMS plans to require that states publish more detailed rate information in a consistent format. States, health plans, providers, and other interested stakeholders will want to consider the implications by delivery system. Additional transparency requirements could create a new opportunity to understand rates across payers and states and use this information in addressing access challenges for services.
The proposed rule also would require extensive comparative analysis of Medicaid FFS rates and Medicare rates. CMS proposes to use Medicare non-facility payment rates as a benchmark to determine if states are meeting federal Medicaid access State analyses will be vital to CMS oversight as well as advocacy efforts within states to monitor and update FFS rates as needed.
Strengthening the Focus on Quality in State HCBS Programs. Over the last several decades, states and Medicaid stakeholders have made significant progress toward increasing participation in HCBS programs and community integration initiatives to counter Medicaid’s institutional bias. CMS is proposing more consistency in the expectations and reporting for HCBS quality measures to further the impact and create a consistent foundation for the recently mandated HCBS quality initiatives starting to take root.
In the short-term, the proposed changes will require states, and likely downstream providers and Medicaid agencies, to immediately change their quality reporting policies and systems. States and their stakeholders will want to map out processes for cyclical updates to HCBS quality measures, including cross-walking the future measures with existing ones, making systems changes, and updating dashboards. Targeted attention and focus will be needed to identify realistic HCBS performance targets that yield successful improvement strategies in the midst of a workforce crisis. Longer term, it will be necessary to map out when updates and reporting will be required to strengthen the rigor and accountability for state performance in the HCBS quality measure set, as well as reinforce the information available to make policy, clinical, and operational improvements to Medicaid programs.
HCBS Access Measurement. CMS is proposing new FFS HCBS payment and access transparency requirements to ensure compliance with Medicaid provider payment rules that require payments to be adequate to enlist at least the same number of providers that the overall geographic population can access. Because the targeted HCBS services do not have a comparable Medicare rate, CMS proposes implementation of a payment rate disclosure approach that would standardize data and monitoring across service delivery systems, with the goal of improving access. In addition to proposed payment transparency changes, CMS proposed new reporting on HCBS waiver waiting lists and timelines for the start of related services once authorized.
These new reporting requirements will provide stakeholders with more information to benchmark their state’s experience with other providers across the nation. This information could be influential to policymakers and legislators and help uncover some of the core contributors to our nation’s HCBS workforce shortage.
Improving Health Equity with Medicaid Beneficiary Input. CMS proposes overhauling the scope and membership of the state Medical Care Advisory Committee. The new Medicaid Advisory Committee (MAC) would continue to advise the state on health and medical matters and play an expanded advisory role on matters of policy development and effective administration of the program. CMS also plans to require that states establish a Beneficiary Advisory Group (BAG) composed of current or past Medicaid beneficiaries. A subset of BAG members would serve on the MAC to ensure their perspectives are integrated into the committee’s recommendations to states.
Under the new federal requirements, MAC representatives could have greater relative input and influence on policies and actions each state Medicaid agency advances. Medicaid stakeholders will want to ensure the MAC’s minimum federal requirements support effective structures and processes in states.
What’s Next
CMS plans to reframe Medicaid access as one of three parts of the continuum of care, along with enrollment and maintenance of coverage. The proposals in the Access to Care rule would have a meaningful impact on the volume and type of data available to evaluate the relationship between Medicaid payment rates and access across all delivery systems.
States, managed care organizations, providers, Medicaid enrollee advocacy organizations, and other interested stakeholders should analyze the proposals and consider submitting comments to CMS on the feasibility, potential impact, and, where applicable, alternatives to the proposed changes. They also can use this time to begin planning and determine which resources and tools they may need to prepare for implementation of changes across delivery systems in the Medicaid program.
HMA’s experts are taking a wholistic approach to reviewing the Access to Care and Managed Care proposed rules in tandem and identifying key points of intersection.
For more information on the access to care proposed rule, contact HMA’s team of experts, Susan McGeehan and Andrea Maresca.