HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
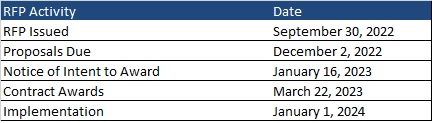
This week, our In Focus reviews the New Mexico Medicaid managed care request for proposals (RFP), released on September 30, 2022, by the New Mexico Human Services Department (HSD). The state will transition to a new program called Turquoise Care in 2024, which will build upon the current Centennial Care 2.0 program through a new Section 1115 waiver demonstration. Managed care organizations (MCOs) will provide physical health, behavioral health, and long-term care (LTC) services to approximately 800,000 Medicaid managed care members.
RFP
New Mexico plans to award Turquoise Care contracts to three MCOs. One of the selected MCOs will also be awarded a specialized foster care plan contract to provide services to Children in State Custody (CISC) on a statewide basis. CISC will be mandatorily enrolled and Native American CISC members will have the option to voluntarily enroll.
Turquoise Care will introduce new practices aimed at improving quality based on population health outcomes. The program will focus on three goals:
Goal 1: Build a New Mexico health care delivery system where every Medicaid member has a dedicated health care team that is accessible for both preventive and emergency care that supports the whole person – their physical, behavioral, and social drivers of health.
Goal 2: Strengthen the New Mexico health care delivery system through the expansion and implementation of innovative payment reforms and value-based initiatives.
Goal 3: Identify groups that have been historically and intentionally disenfranchised and address health disparities through strategic program changes to enable an equitable chance at living healthy lives. The target populations will be:
Prenatal, postpartum, and members parenting children, including children in state custody
Seniors and members with long-term services and supports (LTSS) needs
Members with behavioral health conditions
Native American members
Justice-involved individuals
Other changes for Turquoise Care include:
90 percent Medical Loss Ratio (MLR) aimed at improving quality of care
Expanded MCO reporting and monetary penalties for non-compliance
Minimum reimbursement rate for contract providers at or above the state plan approved fee schedule
More stringent provider network requirements
A single centralized vendor to process applications
Enhanced MCO staffing requirements, including qualifications, staffing levels, and training
Focus on social determinants of health
New Mexico will submit the Section 1115 demonstration waiver for Turquoise Health to the Centers for Medicare & Medicaid Services (CMS) for approval by December 2022. HSD will update the model contract to reflect the requirements related to the waiver renewal upon its approval.
During this procurement, the state will also be developing and implementing a new Medicaid Management Information System (MMIS).
Eligibility
Approximately 83 percent of the Medicaid population is in managed care.
Populations exempt from mandatory managed care enrollment are:
Native American members not in need of LTC
Individuals with Intellectual Disabilities (ICF-IID) in Intermediate Care Facilities
Individuals enrolled in Qualified Medicare Beneficiary (QMB), Specified Low-Income Medicare Beneficiary (SLIMB), or Qualified Individuals program
Individuals covered only under the Medicaid Family Planning program
Individuals enrolled in the Program of All-Inclusive Care for the Elderly (PACE)
Individuals covered pursuant to Emergency Medical Services for Non-Citizens (EMSNC)
Members in the Developmental Disabilities 1915(c) Waiver and in the Medically Fragile 1915(c) Waiver will continue to receive home and community-based services (HCBS) through that waiver but are required to enroll with an MCO for all non-HCBS.
Timeline
Proposals are due December 2, 2022. Contracts will run from January 1, 2024, through December 31, 2026, with optional one-year renewals, not to exceed eight years total.
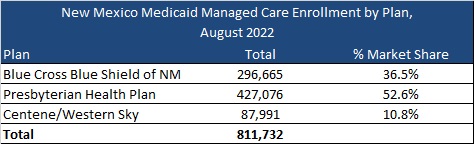
Current Market
New Mexico had 811,732 Medicaid managed care as of August 2022, served by Blue Cross Blue Shield of New Mexico, Presbyterian Health Plan, and Centene/Western Sky. The state also had an additional 163,361 fee-for-service members.
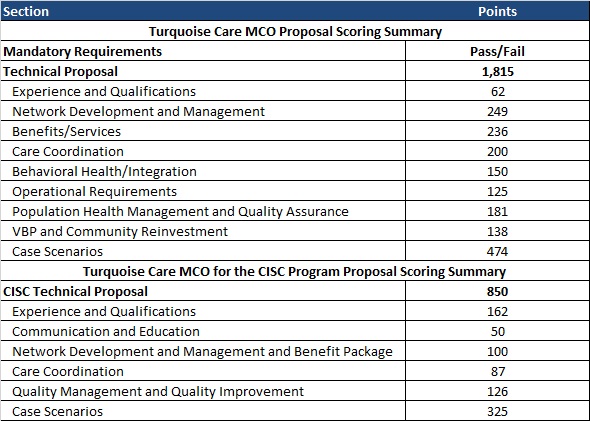
Evaluation
The evaluation process will consist of three phases: review of mandatory requirements, review and scoring of the technical proposals, and review and scoring of the CISC technical proposals.
Communities across the country are seeing elevated numbers of adolescents in the Emergency Department due to suicide attempts, self-harm, anxiety, depression, substance use disorder (SUD), and overdose. While this youth mental health crisis predates COVID, it has been greatly exacerbated by the pandemic. According to the Centers for Disease Control and Prevention (CDC), in 2019, 13% of adolescents reported having a major depressive episode, a 60% increase from 2007, and suicide rates rose nearly 60% for youth ages 10 to 24 by 2018[1]. Then it got worse. Last December, the U.S. surgeon general issued a public health advisory about the adolescent mental health crisis as emergency room visits due to suicide attempts rose 51% for adolescent girls in early 2021, compared to the same period in 2019. For boys, the increase was 4%[2].
The surgeon general recommends a “whole-of-society effort,” including a focus on mental health education and prevention, early identification, and access to high-quality mental healthcare.[3] School-based intervention is ideal because only 20% of students in need of more intensive services typically receive needed care when referred to external providers.[4]
The Bipartisan Safer Communities Act has committed $1.7 billion for mental health support in schools and communities via an array of methods including grant programs. The following programs are currently available for a wide array of eligible entities, including states, cities/counties, Local Education Agencies (LEAs), Indian tribes or tribal organizations, health facilities, and nonprofit entities:
Project AWARE (Advancing Wellness and Resiliency in Education). This grant program provides up to $1.8 million per year for up to 4 years to develop a sustainable infrastructure for school-based mental health programs and services. Grant recipients are expected to build collaborative partnerships with the State Education Agency (SEA), LEA), Tribal Education Agency (TEA), the State Mental Health Agency (SMHA), community-based providers of behavioral health care services, school personnel, community organizations, families, and school-aged youth. Grant recipients will leverage their partnerships to implement mental health-related promotion, awareness, prevention, intervention, and resilience activities to ensure that students have access to and are connected to appropriate and effective behavioral health services. Applications are due October 13th.
Resiliency in Communities After Stress and Trauma (ReCAST). This program provides up to $1,000,000 a year for up to 4 years to promote resilience, trauma-informed approaches, and equity in communities that have recently faced civil unrest, community violence, and/or collective trauma within the past 24 months; and to assist high-risk youth and families through the implementation of evidence-based violence prevention, and community youth engagement programs. SAMHSA expects ReCAST to be guided by a community-based coalition of residents, non-profit organizations, and other entities (e.g., health and human service providers, schools, institutions of higher education, faith-based organizations, businesses, state and local government, law enforcement, and employment, housing, and transportation services agencies). Applications are due October 17th.
In addition to these two grants, there will be an expansion of the Certified Community Behavioral Health Center (CCBHC) Demonstration for States that is expected to be released later this month. The Excellence in Mental Health Act[5] established a federal definition and criteria for CCBHCs. These centers are a provider type that delivers a comprehensive range of mental health and SUD services to vulnerable individuals. They meet people where they are, which can include school-based services, and act as a critical partner in ensuring people have access to quality, affordable, and accessible mental health care.
School-based Mental Health Services
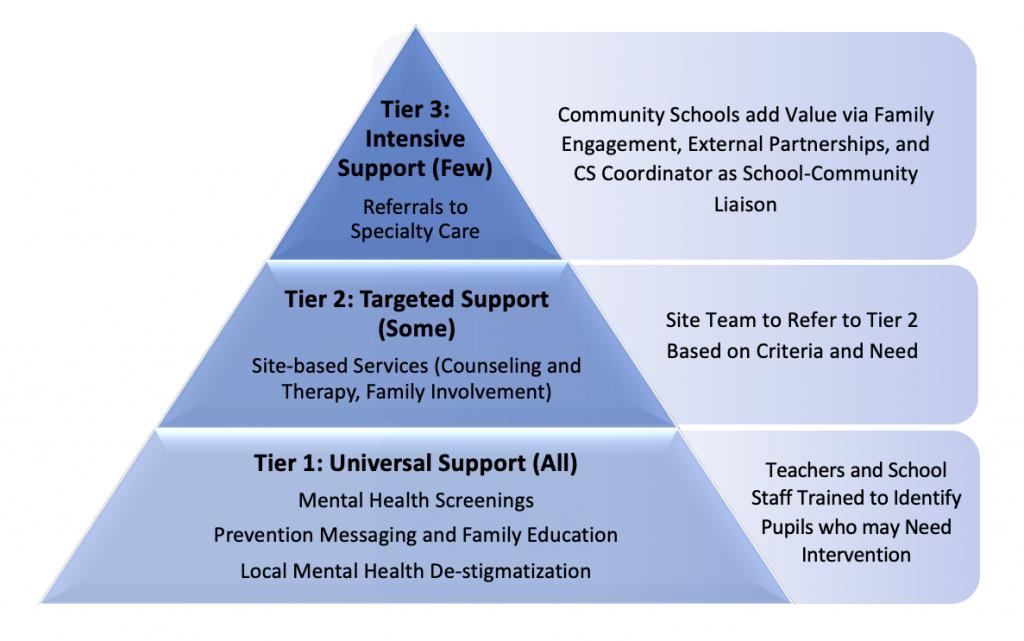
School-based mental health services, delivered within a Multi-Tiered System of Supports (MTSS) framework, can be supported by the aforementioned funding opportunities. The MTSS framework is currently used in public schools to target services and supports to students. As shown below, MTSS addresses universal prevention and progressively targeted support for students and families. It also aligns well with partnerships with community providers to establish an authentic community response that addresses the continuum of mental health needs.
Multi-Tiered System of Supports (MTSS) framework
The key to a successfully implemented MTSS framework is a strong partnership between the school staff, parents/guardians, children, and community partners. This partnership works well when anchored to an evidence-based socio-emotional curriculum that is reinforced across all Tiers and familiar to all parties.
Suicide and Self Harm Prevention
Dialectical Behavioral Therapy (DBT) was recently identified by the New York Times as “the Best Tool We Have’ for Self-Harming and Suicidal Teens,” because it is one of the only interventions found to reduce self-harm and suicidal ideation, its effects are maintained at one-year follow-up[6], and it successfully engages young people[7].
Curriculum developers Drs. Lizz Dexter-Mazza and James Mazza worked with Marsha Linehan, the DBT treatment developer, to adapt DBT Skills into a universal school-based social emotional learning curriculum, called DBT-STEPS-A. This approach is designed to help schools intervene and support well-being and resiliency before kids are suicidal or self-harming. It trains existing school personnel to integrate skill-building into the school program, universally or as a stand-alone option for youth in 6-12th grade (an elementary version is in development). As such, it is a viable approach, despite the current shortage of mental health care professionals in school-based settings.
In addition, DBT provides a shared language and strategies across all three MTSS tiers so that everyone (students, school staff, teachers, providers, and parents/guardians) can benefit. Because DBT is also commonly provided in inpatient, outpatient, and residential behavioral health programs, the value of extending this approach into school settings is further magnified for youth who transition from the highest levels of care.
A DBT STEPS-A program taught at the universal level provides the broadest application within school-based settings, supports uptake that leads to peer-to-peer coaching and support, along with shifting the school environment and culture to promote mental wellbeing and reinforce the skills via a shared language and common strategies. In Tier 2, students are supported to practice skills and decision-making strategies in smaller group or individual psychotherapy sessions as needed. The third tier is more intensive support for students experiencing ongoing emotional and behavioral difficulties for whom Tier 2–level support is not sufficient. It is designed to supplement individual psychotherapy for those in need of a higher level of care. Parent/guardian skills-training seminars are recommended, so they can learn about the skills their child is acquiring and how best to support them while they are practicing. Engaging parents/guardians proactively helps to increase adaption of the skills across both home and school contexts.
A matched sample of adolescents who received the DBT STEPS-A curriculum demonstrated lower scores on the BASC-2 Emotion Symptom Index and on the BASC-2 Internalizing Problems, indicating fewer mental health difficulties, compared to peers who did not receive the curriculum (Cohen’s F squared equal to 0.65 and 0.83, respectively[8].
The DBT curriculum is accessible via a $50 manual. All handouts for kids are available in English and Spanish and can be printed from a web-based link for free. An array of trainings are available to support rapid school-based service delivery.
To learn more about current and upcoming funding for enhanced school and community-based mental health care or DBT-STEPS-A, contact:
You can also contact DBT in Schools, LLC for information about DBT-STEPS-A [email protected].
[1] National Vital Statistics reports – Centers for Disease Control and … (n.d.). Retrieved from https://www.cdc.gov/nchs/data/nvsr/nvsr69/nvsr-69-11-508.pdf
[2] Richtel, M. (2021, December 7). Surgeon general warns of Youth Mental Health Crisis. The New York Times. Retrieved from https://www.nytimes.com/2021/12/07/science/pandemic-adolescents-depression-anxiety.html
[3] Protecting youth mental health – hhs.gov. (n.d.). Retrieved from https://www.hhs.gov/sites/default/files/surgeon-general-youth-mental-health-advisory.pdf
[4] Sheryl H. Kataoka, M.D., M.S.H.S., Lily Zhang, M.S., and Kenneth B. Wells, M.D., M.P.H. (2002). Unmet Need for Mental Health Care Among U.S. Children: Variation by Ethnicity and Insurance Status. The American Journal of Psychiatry: https://doi.org/10.1176/appi.ajp.159.9.1548
[5] Excellence in Mental Health Act. (2013, February 7). http://www.congress.gov/
[7] Rathus, Jill H. ( 2014). DBT skills manual for adolescents. New York :The Guilford Press,
[8] Elizabeth T. Dexter-Mazza, James J. Mazza, Alec L. Miller, Kelly Graling, Elizabeth Courtney-Seidler, and Dawn Cattuchi (2022). Application of DBT in a School-Based Setting. Pending publication
Today, Jay Rosen, founder, president, and co-chairman of Health Management Associates (HMA), and David Kulick, co-founder of Adaptation Health, announced that Adaptation Health is joining HMA. It will continue to operate as Adaptation Health, an HMA Company.
Founded in 2017, Adaptation Health is an innovation consultancy and incubator based in New Orleans that works with state Medicaid programs and managed care organizations (MCOs) to drive adoption of new delivery and engagement solutions. Adaptation brings together leaders from these sectors to solve systemic problems in publicly funded healthcare.
“Like HMA, Adaptation Health has innovation in its DNA,” Rosen said. “I’m excited to pair HMA’s unmatched Medicaid expertise with Adaptation Health’s creative approach and laser focus for tackling the complex challenges related to Medicaid to benefit those the program serves.”
Adaptation Health has worked across dozens of states and MCOs to build private market innovation through expert vendor sourcing, diligence, and deployment driving improvements in member care, acceleration of equity, and supporting positive evolution in public market delivery. They have directly worked with over 500 startups and early Medicaid-focused companies to enable best-in-class solutions for the public good.
“We are very excited to join HMA as they are pre-eminent Medicaid experts. We believe that through this partnership Adaptation Health can continue to support states and MCOs across the country in accelerating Medicaid performance, value, and innovation.” Kulick said.
Kulick will continue to lead Adaptation Health, an HMA Company. Terms of the transaction were not disclosed.
Founded in 1985, HMA is an independent, national research and consulting firm specializing in publicly funded healthcare and human services policy, programs, financing, and evaluation. Clients include government, public and private providers, health systems, health plans, community-based organizations, institutional investors, foundations, and associations. With offices in more than 20 locations across the country and over 500 multidisciplinary consultants coast to coast, HMA’s expertise, services, and team are always within client reach.
Today, Jay Rosen, founder, president, and co-chairman of Health Management Associates (HMA), and David Kulick, founder and managing director of The Focus Group, announced the merger of the two firms. The Focus Group will continue to operate as The Focus Group, an HMA Company.
Founded in 2014, The Focus Group, based in New Orleans, helps healthcare clients navigate the intersection of healthcare policy, payment, and delivery by devising and implementing strategies that create change and fuel growth. Led by public market and business transformation experts, Kulick and Alex Rich have partnered with hundreds of company executives to solve complex challenges and deliver high-value projects. The Focus Group services include market intelligence, strategy development, business transformation, and go-to market execution for providers, payers, life sciences, health foundations, and private equity investors.
“The Focus Group brings extensive expertise across the healthcare spectrum, driving growth for a wide array of clients,” Rosen said. “We’re excited to add their unique approach to managing change and commitment to innovation to our impressive lineup of experts as we continue to expand the ways we can serve our clients and partners.”
“We are thrilled to merge with HMA and drive greater value to our clients. This is a strategic opportunity to link HMA’s vast depth in healthcare policy and payment with our focus on commercial growth to lead the charge together for positive evolution in healthcare delivery,” Kulick said.
Kulick and Rich will continue to lead The Focus Group, an HMA Company, as managing directors. Terms of the transaction were not disclosed.
Founded in 1985, HMA is an independent, national research and consulting firm specializing in publicly funded healthcare and human services policy, programs, financing, and evaluation. Clients include government, public and private providers, health systems, health plans, community-based organizations, institutional investors, foundations, and associations. With offices in more than 20 locations across the country and over 500 multidisciplinary consultants coast to coast, HMA’s expertise, services, and team are always within client reach.
Community Response Teams are vital cross-sector, data driven, community-based collective action initiatives that address the local opioid crisis through harm reduction education, Naloxone distribution, and data. During this webinar, HMA speakers addressed the rationale, framework, funding, and implementation of successful initiatives that serve as models for other states, including case studies from California and Delaware.
Learning Objectives
Create local community collaborations focused on opioid education, Naloxone distribution, and reducing stigma.
Understand the four critical concepts of the Community Response Team framework: prepare, use data, prevent, and co-design with community.
Understand how counties in California and Delaware implemented the framework.
This week, our In Focus section looks at the current federal policy landscape and trends and the legislative outlook for the remainder of 2022 and beyond. Experts from HMA continue to monitor developments in this area and provide additional updates as more information becomes available.
Legislative Branch
To date in 2022, Congress passed multiple comprehensive bills, including the Inflation Reduction Act (IRA), which was signed by President Biden on August 16, 2022. The IRA extends Exchange plan premium tax subsidies through 2025, institutes an out-of-pocket drug spending cap for Medicare beneficiaries, expands Medicare, Medicaid, and CHIP coverage protections for certain vaccines, allows Medicare to negotiate drug prices, and implements a penalty payment in the Medicare program for prescription drug prices that rise faster than the rate of inflation.
Going forward, stakeholders have an extensive list of immediate Medicare payment issues for Congress to tackle while lawmakers continue to consider fundamental reforms to the program. Priorities include mitigating Medicare payment reductions scheduled for 2023; providing relief to address inflationary cost pressures; extending the 5 percent bonus for physicians participating in Advanced Alternative Payment Models (APMs), which expires at the end of 2022 for Accountable Care Organizations (ACOs); and permanently expanding telehealth access and payment policies after the federal COVID-19 public health emergency (PHE) declaration expires. Many stakeholder groups are also urging the Senate to act on the House-approved legislation, Improving Seniors Timely Access to Care Act (H.R. 3173), to reform Medicare Advantage prior authorization policies.
Congress did not include major Medicaid proposals in the Inflation Reduction Act. Medicaid stakeholders want Congress to revisit certain Medicaid policies in one of the remaining legislative vehicles this year. Significant proposals of interest include closing the Medicaid coverage gap in non-expansion states, enhanced coverage for justice involved populations, and expanding support for home and community-based services (HCBS). States and some stakeholders have also sought more certainty in the timing and guardrails for ending the COVID-19 Public Health Emergency (PHE) policy that links enhanced federal Medicaid funding with the requirement for continuous Medicaid coverage.
Congressional leaders and key influencers are laying the groundwork for 2023 legislative efforts. Congress is likely to defer action on most major legislative issues until after the November mid-terms, including finalizing federal fiscal year 2023 funding for most departments. A change in control of either or both chambers of Congress will likely lead to greater scrutiny of the Biden Administration’s health care policies and actions, which have largely gone untested by this Congress.
Executive Branch
Executive orders have been a major source in driving federal workstreams in 2022. Following enactment of several major bills, implementation responsibilities have shifted to the Executive Branch and stakeholders will have multiple opportunities to further shape and support new programs, regulatory and policy updates, and funding opportunities. Executive orders passed include:
Advancing Racial Equity and Support for Underserved Communities, January 21, 2021
Promoting Competition in the American Economy, July 9, 2021
Improving the Customer Experience, December 13, 2021
Access to Affordable, Quality Health Coverage, April 5, 2022
Equality for LGBTQI Individuals, June 15, 2022
Protecting Access to Reproductive Healthcare Services, July 8, 2022
The Administration will continue to address COVID-19 emergency needs while stepping up efforts to support states, health plans, providers and other stakeholders as they prepare for the post-COVID environment. The current PHE declaration expires October 13, 2022, but since HHS has not signaled that it plans to end the PHE in October, another extension is likely until January 11, 2023. The next advance notification about the end of the PHE would be Nov. 12, 2022. Once the PHE declaration expires, numerous Medicare and Medicaid, TANF, and SNAP flexibilities will end, including Medicaid’s continuous coverage requirement and certain telehealth flexibilities, among others. Additional federal agency guidance is expected to support post-PHE transitions.
The Centers for Medicare & Medicaid Services (CMS) plans to advance new policy direction across several service and delivery areas, including strengthening long-term services and support and innovations via Section 1115 demonstration programs. CMS is expected to approve transformational 1115 proposals in additional states. Several state proposals focus, in part, on building capacity among local and regional entities and community-based organizations to address social drivers of health. Many state proposals are also strengthening behavioral health delivery systems and seek to meet enrollees’ urgent behavioral health needs. Additionally will want to monitor CMS’ regulatory efforts to align and strengthen managed care and fee-for-service (FFS) access and network adequacy policies as well as updates to the agency’s in lieu of services policy in managed care programs.
The Administration is also expected to accelerate work on its top policy priorities and regulatory agenda in advance of the next Presidential election, and this will require ongoing engagement among health care stakeholders.
For additional information on these and other policies, please contact Andrea Maresca, Amy Bassano, Zach Gaumer, Jon Kromm, or Kevin Kirby.
With the help of newly available federal funding, states like Minnesota are poised to dramatically advance crisis systems and services to address the needs of individuals who experience behavioral health crises. During this webinar, speakers provided an overview of key behavioral health crisis initiatives nationwide, including a look at specific community efforts that can inform the development of improved systems and services in Minnesota.
Learning Objectives
Understand the differences between crisis systems and crisis services.
Find out how communities are advancing crisis systems and services by leveraging national opportunities.
Assess the implications of SAMHSA’s focus on block grant funding for crisis services.
Learn how the new national 988 call number and allocations for 988 infrastructure support can drive improved crisis response.
The Bipartisan Safer Communities Act offers states new funding for expansion of the Certified Community Behavioral Health Clinic (CCBHC) Demonstration. The next CCBHC Planning Grant RFP for states is anticipated to be released in the fall of 2022. In this webinar, the first of a two-part series, experts from HMA and the National Council for Mental Wellbeing discussed:
The CCBHC Demonstration opportunity and what the evidence for the model demonstrates
How states have used the CCBHC model as a transformational opportunity that can help behavioral health care systems achieve broader health quality and access goals
Lessons New York and Michigan have learned from their CCBHC efforts, including key takeaways from the application and implementation processes
Speakers
Kristan McIntosh, Principal, HMA Heidi Arthur, Principal, HMA Dave Schneider, Managing Principal Rebecca Farley-David, Senior Advisor, Public Policy and Special Initiatives, National Council for Mental Wellbeing
Check Out Part 2 of our CCBHC Planning Grant Webinar Series
In our follow-up webinar, HMA and National Council for Mental Wellbeing reviewed the specific requirements of the Substance Abuse Mental Health Services Administration (SAMHSA) Notice of Funding Availabilities (NOFA) and shared recommended activities for states to have a successful application. The recording and slide deck can be found here.
This week, our In Focus section highlights an issue brief from Wakely, an HMA Company, The Basics of Evaluating PBM Contracts, published September 2022. The brief provides an overview of the basic financial elements of a pharmacy benefit manager (PBM) contract. Evaluation of a traditional request for proposals (RFP) or PBM contract should begin with financial analysis of the following four key elements: discount guarantees (typically understood as point-of-sale ingredient costs), dispensing fees, rebate guarantees, and PBM administrative fees. This paper addresses various points of consideration when attempting a financial analysis of these contract elements.
Payors today face unprecedented degrees of complexity when conducting a PBM RFP or evaluating PBM contracts. To stay competitive, payors must navigate an ambiguous and changing pricing environment. That requires a solid understanding of PBM contracting. In a proposal, some PBMs may offer better AWP discounts while other PBMs offer better rebate guarantees. Alternatively, a payor may find a PBM that offers the best discounts and rebates but charges significantly higher administrative fees. Such analysis will consider the impacts of these key components together with historical and projected drug mix. While any PBM analysis must start with the elements discussed in this paper, a complete analysis must dive below the surface and into the fine print underlying these items.