HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
This week, our In Focus section reviews the release of the 2025 Medicare Advantage (MA) Star Ratings and pivots to the actions that Medicare Advantage Organizations (MAOs) could take to improve performance in future rating cycles.
Background
Newly released MA Star Ratings information is based on the 2025 Star Ratings published on the Medicare Plan Finder on October 10, 2024. Star Ratings are largely based on the quality of care, member satisfaction, and retention.
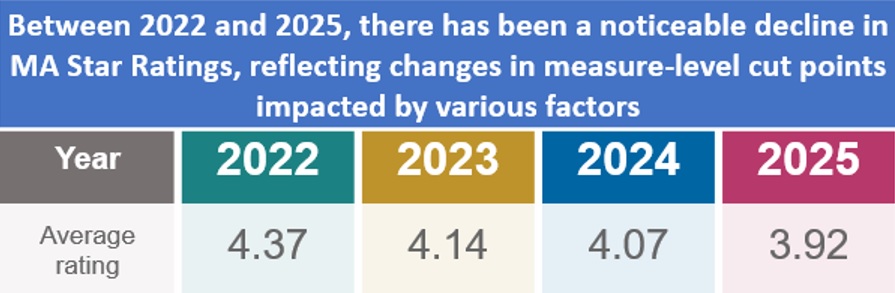
The Centers for Medicare & Medicaid Services (CMS) increased many measure-level cut points from the 2024 Star Ratings, requiring MAOs to achieve higher performance on these measures to receive a four or higher Star Rating. An earlier In Focus reviewed a white paper published by Wakely, an HMA Company, which provides an in-depth analysis of CMS’s latest policy and methodology changes that affect an MAO’s overall quality performance and Star Rating.
Topline Results
Significant attention is being given to the notable overall industry decline in Star Ratings. Specifically, only seven Medicare Advantage (MA) plans received an overall 5-Star Rating in 2025, compared with 38 in 2024. Only 40 percent of MA prescription drug plans achieved a score of four or five Stars versus 43 percent in 2024.
Key Considerations for Star Ratings, and What to Do About Them
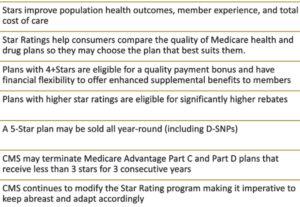
The ratings significantly influence the financial and operational effectiveness of each MAO, directly affecting plan reimbursement and ability to enhance benefits. The 2025 Star Ratings will impact 2026 MA quality bonus payments. Health plans that earn four or more Stars are eligible for quality bonus payments and greater rebate percentage the following year. Plans may reinvest payments to make plan products more attractive to beneficiaries and emphasize a higher rating in their marketing efforts.
In the wake of CMS’s release of Star Ratings, an intense focus has shifted to each MAO’s specific overall Star Rating. Given the clear implications for population health and health plan sustainability, companies will need to quickly pivot to address opportunities for performance improvement. Key steps to optimize Star Ratings include:
Grow Foundational Knowledge – MAOs need to build broad organizational understanding of the domains and measures, the weights, the levers that can affect individual measures and domains, and the rating cycle.
Assess the Current Landscape – Organizations will benefit from having executive sponsorship, a governance structure, and overall leadership for each domain and measure. They should develop the ability to report on measures, and set interim goals. Assessments also need to ensure the network and bonus structure are aligned with Stars.
Develop a Roadmap –A calendar of events is critical for supporting performance improvement. This should include a preoperational and operational strategy as well as a year-over-year workplan to track, assess, and identify systems, technology, processes and people with a process for evaluation. Formulate a hiring and investment plan, if needed.
Prepare for Reporting and Oversight – Develop a reporting and oversight structure, including a cadence of reporting and structure for review, process, and timing of reports by measure/domain leads. Ensure dashboards are updated annually to include new measures and weights and that a process is in place for managing display measures.
What to Watch
The MA landscape is highly dynamic, with some companies leading in market share, while others are leaders on quality ratings. As companies adapt to regulatory changes and strive for higher quality ratings, we can anticipate further shifts in the coming years. This will be exacerbated by shifts we are forecasting based upon the Health Equity Index and upcoming changes in Star weights. Strategies and actions MAOs implement in 2024 and 2025 will affect their 2026 Star Ratings.
Connect with Us
HMA experts have conducted in-depth analysis on all contracts, domains, and measures that roll into the Star Ratings. For further analysis of the 2025 trends and plan-specific impacts, contact our featured experts below.
Explore The HMA Stars Accelerator Solution for additional insights into programmatic strategies, best practices for design of meaningful solutions to implement, and approaches to measure the effectiveness of these solutions.
Laguna Honda Hospital and Rehabilitation Center (LHH) is the largest publicly owned and operated nursing facility in the United States and has cared for those most in need for more than 150 years. Licensed at 780 beds, LHH serves patients with complex medical needs who are low or very low income as part of the San Francisco Health Network. Health Management Associates (HMA) was engaged by the San Francisco Department of Public Health (SFDPH) to conduct a comprehensive, top-to-bottom assessment in support of its effort to attain Centers for Medicare & Medicaid Services (CMS) recertification.
BACKGROUND
For this engagement, HMA brought together a team of experts with decades of national experience leading public health systems and organizations, including skilled nursing facilities. HMA’s subject matter experts included a long-term care physician specialist, a quality expert, long-term and acute care administrative and nursing leaders, a former California county public health official, and behavioral health specialists.
APPROACH
The assessment produced by HMA included:
An in-depth analysis of operations, leadership, governance, staffing, and the model of care to drive strategy planning, execution and attained favorable clinical results.
An in-depth review of nursing unit staffing, including clinical staffing mix, support staffing, leadership’s span of control.
Evaluation of the medical staff leadership, staffing and clinical affiliation models.
Identified key root causes of operational and regulatory challenges.
Developed and delivered a comprehensive month-long training curriculum for all 1,200 staff to address knowledge and skill gaps.
Evaluation and recommendations to drive the effectiveness of the quality management and performance improvement functions.
Reviewed policies and procedures and recommended restructuring based on evidence-based data, best practices, and stakeholder interviews, which are currently being implemented by the facility.
A full facility mock survey to serve as a baseline for identifying gaps and development of a compliance workplan.
TESTIMONIAL
“HMA is a trusted partner and has been vital in helping Laguna Honda Hospital’s CMS recertification efforts. Their guidance, expertise, and hands-on work contributed to our sustained improvements.”
Roland Pickens, MHA, FACHE, CEO, San Francisco Health Network
RESULTS
The team spent extensive time at the facility and on nursing units observing resident care delivery. They also conducted in-depth interviews with internal and external stakeholders, including clinicians, community leaders, union representatives, political leaders, advocates, and others.
The resulting efforts provided improvements for restructuring, governance and leadership development, quality management improvements, and organizational transformation necessary to enable successful and sustained CMS recertification of the facility in compliance with skilled nursing regulations. The facility was recently recertified by both Medi-CAL and CMS as a result of the improvements made through this project.
This week’s In Focus section previews key public policy issues affecting Medicare Advantage (MA) and Medicare Part D that could potentially be addressed under regulations issued by the Centers for Medicare & Medicaid Services (CMS) later this fall. CMS’s highly anticipated regulations—which include annual programmatic, policy, and technical updates to the MA and Part D programs for the coming plan year—are under review at the Office of Management and Budget and are expected to be released in the coming weeks ahead.
In addition to the proposed rule, healthcare organizations are closely tracking CMS regulations that are expected to be released later this year, which would impact MA plan payment rates as well as proposed regulations intended to streamline the prior authorization process for prescription drug coverage under Medicare. This annual regulatory policymaking process is getting under way as the Medicare Open Enrollment period begins October 15, 2024, during which Medicare beneficiaries will compare Medicare health plan and drug coverage options and select the coverage that best meets their health care needs. (See Table 1 for key 2024 MA dates.)
As the last major Medicare policy regulations from the Biden Administration, healthcare entities can expect a continued focus on regulatory policies and requirements that strengthen program oversight and enhance beneficiary protections, while also seeking to maintain stability in Medicare benefits offerings and plan choices.
Following are some of the key issues to watch for as CMS’s annual regulatory process begins this fall.
Health Equity
Ensuring health equity is a foundational element of CMS’s strategic plan and the agency seeks to advance health equity goals and improvements across all of its programs, including Medicare Advantage. Beginning next year, MA plans will be required to conduct an annual review and analysis of utilization management (UM) policies and procedures from a health equity perspective. By requiring public reporting and identifying any impacts on underserved populations, this requirement is designed to ensure MA plans’ UM policies and procedures ensure access to medically necessary care, especially for vulnerable, low-income populations, such as beneficiaries who receive the Part D low-income subsidy and those who are dually eligible for Medicare and Medicaid.
In addition, CMS has finalized rules to collect health equity data, including race and ethnicity data, and adopted changes to the MA quality measurement program that will provide incentives for MA plans to improve care for underserved and vulnerable populations, including beneficiaries with high social risk factors.
Stakeholders should expect CMS to continue building and strengthening policies to advance health equity goals while exploring new initiatives to reduce disparities and close gaps in care for vulnerable populations.
Consumer Protection and Oversight
Earlier this year, CMS launched a high-profile effort to increase transparency in Medicare Advantage, including the release of a request for information (RFI) to solicit public input on ways to improve data collection and enhance oversight over all aspects of the MA program. More details are available in the press release. In addition to seeking comments on improving overall MA data collection and public reporting, the CMS RFI on MA data collection solicited specific recommendations to improve data collection and accountability for MA plans’ provider networks and prior authorization process.
While the formal comment period closed in May 2024, responses to the CMS RFI on MA data collection can inform and shape future regulatory policy direction, as CMS continues to examine ways to improve transparency and oversight over MA plans.
Quality and Star Ratings
CMS will soon release the Medicare Advantage Star Ratings, which measure the quality of MA plans based on a range of quality and performance metrics. The Star Rating system provides beneficiaries with crucial information to compare plans and select the coverage option that best meets their needs. High-performing plans receive bonuses—which provides incentives for plans to continue to improve quality of care for beneficiaries and patient outcomes. Last year, MA plans received $11.8 billion in bonus payments, and 74 percent of MA beneficiaries were enrolled in plans that achieved a rating of four or more stars. For more information, read the issue brief.
On the regulatory front, CMS recently adopted significant changes to Star Ratings that continue to have far-reaching impacts on MA plans’ quality performance, which, in turn, will continue to shape and inform their quality improvement strategies. Among the notable regulatory changes CMS has adopted is the new Health Equity Index, which rewards MA plans that provide high quality care to beneficiaries with social risk factors, including low-income beneficiaries and those dually eligible for Medicare and Medicaid. Though this policy change takes effect in 2027, MA plans can take steps now to prepare and enhance their capabilities to improve quality of care for beneficiaries with social risk factors, including using targeted care coordination programs.
As policymakers and stakeholders continue to monitor the impact of recently finalized changes to MA Star Ratings, CMS will continue exploring improvements to the MA Star Ratings system that further raise the bar on quality and ensure the program aligns with CMS’s broader goals and objectives.
Prior Authorization
As MA plans have increased the use of prior authorization and drawn scrutiny among patient advocates and providers, CMS has taken important steps to streamline and improve the prior authorization process to ensure timely access to care for Medicare beneficiaries. These regulatory policy changes—which include continuity of care requirements beneficiaries, increased oversight over UM practices, and ensuing evidence-based clinical decisions within MA are consistent with traditional fee-for-service (FFS) Medicare—are intended to ensure prior authorization and other UM tools do not create barriers to medically necessary care for Medicare beneficiaries.
Policymakers continue to look for ways to further improve the prior authorization process, and CMS has signaled additional interest in further regulatory standards to strengthen oversight and improve beneficiary protections. Potential policy options CMS could pursue include requiring more detailed reporting by MA plans (including number of prior authorization requests, denials, and appeals by type of service), extending prior authorization standards and consumer protections to prescription drugs covered by Medicare, and improving the timeliness of prior authorization decisions to avoid delays in necessary care.
Risk Adjustment Payment Policy and Coding
CMS has adopted significant changes to the MA risk-adjustment model, which continue to be phased in over a three-year period (2024−2026). These changes include important technical changes to improve the model’s payment accuracy, including a focus on conditions that are subject to more coding variation. Because CMS risk-adjustment changes will be fully implemented by calendar year 2026, policymakers and stakeholders are closely monitoring whether CMS will pursue additional regulatory policies to improve the accuracy of the risk adjustment program and address coding issues.
Since 2018, CMS—as required by statute—has applied a coding intensity adjustment that reduces MA risk scores by 5.9 percent annually to ensure consistency with Medicare FFS coding. However, MedPAC and others have continued to raise concerns that MA risk scores are higher than those for similar Medicare FFS beneficiaries, even after accounting for the 5.9 reduction in MA risk scores, which results in increased payments to MA plans. As policymakers continue to evaluate changes to ensure the long-term sustainability of the Medicare program, CMS could consider further changes in this area to equalize payments between MA and FFS Medicare through risk adjustment or coding changes.
Table 1. Key 2024 Medicare Advantage Dates
Date
Event
September 2024
CMS announces average premiums, benefits, and plan choices for MA and Medicare Part D for 2025.
Early-to-mid October 2024
CMS releases MA and Part D plan Star Ratings 2025.
October 15, 2024
Medicare Annual Election Period begins. Medicare beneficiaries can enroll in MA or Part D plans for CY 2025.
October or November 2024
CMS CY 2026 Policy and Technical Changes to MA and Medicare Part D (CMS-4208).
November 2024
CMS Interoperability Standards and Prior Authorization for Drugs (CMS-0062).
December 7, 2024
End of Annual Election Period.
Next Steps
The imminent release of CMS regulations come at a critical time for the Medicare Advantage program, which continues to experience enrollment growth amid a challenging and ever-changing regulatory environment. MA plans and other stakeholders need to be prepared to engage in the formal notice and comment process as well as offer policy solutions and best practices to strengthen and enhance the program for the 33 million beneficiaries it serves.
The Health Management Associates, Inc. (HMA), team will continue to closely monitor the timing of the release of CMS regulations and will analyze the impact of the key provisions once these rules are released. We have the depth, experience, and subject matter expertise to assist organizations engaging in the rulemaking process and assessing their impact. HMA can also assist with tailored analysis and modeling capabilities to assess the policy impacts across the multiple rules and guidance.
If you have any questions about the forthcoming CMS regulations and potential impact on MA plans, providers, and beneficiaries, contact our featured experts below.
This week’s In Focus highlights a white paper that Wakely, a Health Management Associates, Inc. (HMA), company published in September 2024, titled “A Cut Above the Rest: Summary of 2025 Star Rating Cut Point Changes.” The paper provides an in-depth analysis of the latest cut point changes from the Centers for Medicare & Medicaid Services (CMS) to demonstrate how policies like the Tukey Outer Fence Outlier removal logic (Tukey), guardrails, and changes in overall quality performance have led to the highest Medicare Advantage (MA) Star Rating cut points in the program’s history.
Why Cut Points Matter
MA Star Ratings are a critical measure of the quality and performance of MA plans. The MA Star Ratings cut points are the thresholds CMS has set to evaluate the performance of MA plans. These ratings, ranging from 1 to 5 stars, are based on various quality measures, including clinical outcomes, patient experience, and plan administration. CMS applies methodologies such as Tukey to set the cut points and guardrails to stabilize them over time. MA plans are evaluated and earn a rating that is based on their performance against the cut points. Higher Star Ratings can lead to increased enrollment and higher payments from CMS, making them a key focus for MA organizations.
Key Findings
Wakely used the 2025 Star Rating Technical Notes to analyze measure-level cut point changes. The data summarize how Medicare Advantage organizations (MAOs) performed on various quality measures during the 2023 measurement year. Notably, the Tukey methodology was applied for the first time within the 2024 Star Ratings cut points. Initially, the full impact of this methodology was evident in the initial 2024 Star Ratings, but the updated 2024 Star Ratings restricted use of guardrails and spread the impact of Tukey over a few years.
The analysis reinforces expectations for changes in MA spending in 2026, in part because of changes in Medicare Advantage Prescription Drug Overall Star Ratings.
The Star Ratings have been on a steady decline over the last two years while CMS continues to refine and evolve its Star Ratings methodology and areas of focus. Key issues to consider in this climate include:
MAOs are experiencing significant reductions in quality bonus and rebate payments, which potentially affects opportunities to improve member health outcomes.
Strategies to enhance Star Ratings and elevate program quality are crucial for performance and meeting the unique needs of MA enrollees.
MA plans and other stakeholders also should consider that as plans optimize performance on certain traditional quality measures, CMS is placing increased emphasis on member experience with their health plan and providers during care.
The Star Ratings is an important tool CMS uses to redirect plan focus and resources.
CMS is scheduled to release the final scores and Star Ratings for Star Year 2025 in early October 2024. These ratings will be based on the performance data from the 2023 dates of service. This release will provide MAOs with updated quality and performance metrics, which are used to determine CMS Star Ratings and subsequent quality-based payments.
Connect with Us
For further insights into the Star Ratings and more information on the report, contact our featured experts below.
Strategies and actions MAOs implement in 2024 and 2025 will affect their 2026 Star Ratings. For further insights into programmatic strategies, best practices for design of meaningful solutions to implement, and approaches to measure the effectiveness of these solutions, explore The HMA Stars Accelerator Solution.
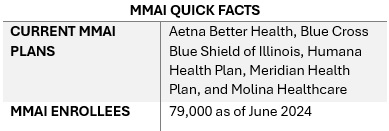
This week, our In Focus section from the HMA Weekly Roundup highlights the Illinois Department of Healthcare and Family Services request for proposals (RFP) for a dual-eligible special needs plan (D-SNP) to replace its current Medicare-Medicaid Alignment Initiative (MMAI) demonstration.
Overview
Illinois is one of the states affected by the Centers for Medicare & Medicaid Services (CMS) decision to end the capitated model in the federal Financial Alignment Initiative (FAI) demonstration. Illinois is among the last states to issue an RFP that will support the transition from the demonstration program. Two states, Texas and South Carolina, have yet to issue RFPs. On September 10, 2024, CMS issued a memo discussing end-of-demonstration enrollment and operational considerations and deadlines by which states should make operational decisions.
The Health Management Associates, Inc., (HMA) In Focus article June 26, 2024, discussed related changes that CMS finalized to the federal policy framework for D-SNPs to enhance care coordination, improve health outcomes, and ensure that dual-eligible beneficiaries receive accurate information about their healthcare while integrating successful features of the FAI demonstration and the Medicare-Medicaid Plan (MMP) program. These decisions are prompting more states to develop new models for integrating Medicare and Medicaid services.
Illinois D-SNP RFP Highlights
This Illinois procurement will transition the state to a fully integrated dual-eligible special needs plan (FIDE-SNP) model, which will include a requirement that plans provide managed long-term services and supports (MLTSS) for both people who are dually eligible and Medicaid-only beneficiaries beginning in 2027.
The RFP is largely focused on quality care provisions and improved care coordination across all services lines, including overall expectations to achieve the following:
Improved access and quality of community-based behavioral health services
Better quality of care in facilities
Fewer program opt-outs
A strategy for increasing the use of alternative payment models (APMs) in Medicaid managed care in Illinois, particularly for behavioral health providers
Emerging National Trends
Overall, the Illinois D-SNP procurement reflects broader national trends toward more coordinated, equitable, and outcome-focused healthcare.
Focus on Health Equity. The procurement emphasizes health equity and reducing disparities, including information on innovations that are responsive to health-related social needs (HRSNs) and social determinants of health (SDOH). The state is weighing payers’ experience partnering with non-traditional providers to meet Medicaid customers’ needs, their innovative programs to address customers who are difficult to locate, and their strategies for improving care for adults with complex needs in facility or community-based settings.
In addition, the state will require plans to report outcomes by race, ethnicity, and geography. Given the demographic and health equity reporting requirements, payers should be prepared to speak to their data collection, member engagement strategies, and relationships with community-based organizations. This capability will be an essential component of addressing both population health and health equity activities.
Alternative Payment Models. The RFP also requests detailed information on the payer’s strategy for increasing the use of APMs in Illinois Medicaid managed care, including the models the payer intends to implement. Experience supported by data-driven outcomes and explanations of work with providers or clinics to adopt, manage, and support reporting and analytics for APMs is a key area of interest for the state. Notably, the state seeks information on plans to include behavioral health providers in APMs.
Long-Term Services Related Transitions. The RFP questions also reflect the long-term services and supports that dually eligible beneficiaries need, as well as those of Medicaid-only beneficiaries who are eligible for these services. More specifically, the RFP raises questions to determine how payers will effectively implement nursing home diversion plans, incentivize hospitals to discharge patients to community settings, and approaches to transition members from institutional settings to the home and community, including by connecting members with supports for HRSNs. Payers will be expected to provide specific examples of their experience and outcomes in other states.
Emerging National Trends
The emphasis on health equity in the Illinois RFP reflects a broader national trend. States are increasingly interested in—and in some situations required—addressing SDOH and reduce disparities, especially for the Medicare and Medicaid dual-eligible population. As a result, payers and other healthcare organizations must develop capacity internally and through external collaborations to build their expertise and evidence base for advancing improvements.
The push for APMs in the Illinois procurement aligns with national efforts to move away from fee-for-service models. Illinois’s inclusion of behavioral health providers in APMs and requiring integrated care models highlights the growing recognition of the importance of mental health in overall health outcomes.
Illinois’s RFP also reflects heightened interest in improving care transitions and coordination. The potential for incentive programs related to community placement and increased focus on nursing home diversion will require innovative plans and a long-term commitment to working with all stakeholders to build on the federal FAI experiences.
What We’re Watching
Responses to the Illinois RFP are due October 18, 2024, and awards are expected to be announced in December. The state anticipates making awards to the top four bidders. Contract execution is estimated July 2025, with implementation January 1, 2026.
As the FAI demonstration ends and CMS’s integration requirements take effect over the next several years, there will be a steep learning curve for states, payers, and other key stakeholders adapting to this evolving environment. Compliance with new CMS rules will be crucial, and experiences in Illinois and other FAI demonstration states can provide valuable insights for other states and stakeholders.
Additional growth and program refinements in the federal Medicare Advantage (MA) landscape are expected in the coming years, especially among MA D-SNPs. Those MA D-SNPs that have yet to participate in Medicaid will need to continue make significant business decisions on participation and actively compete to secure state Medicaid contracts, which will have downstream implications for their state and local partners.
Connect with Us
Health Management Associates (HMA) experts continue to review the evolving landscape and federal changes that will affect D-SNPs in 2025 and beyond. Contact our featured experts below for details about the nationwide D-SNP rules and landscape.
The upcoming HMA event, Unlocking Solutions in Medicaid, Medicare, and Marketplace, offers extensive opportunities to engage with leaders from various sectors who are designing and implementing Medicare-Medicaid integration initiatives. Join us for main stage panel discussions with distinguished health plan executives from national and local plans and Medicaid directors from Iowa, New Mexico, New York, and Rhode Island.
HMA Principal Holly Michaels Fisher will lead a deeper dive into integration issues during the breakout session, Innovations to Improve Outcomes for Medicare-Medicaid Dually Eligible Individuals, with speakers Michael Carson, President and CEO of WellCare; Dr. Steven R. Counsell, Medical Director for the Division of Aging at Indiana Family and Social Services Administration; Dr. Linda Kurian, Executive Medical Director for the Center of Excellence of Medicare Duals/D-SNP at Aetna; and Juliet Marsala, Deputy Secretary for the Office of Long-term Living in the Pennsylvania Department of Human Services.
During the breakout, Meeting New Expectations for Health Equity and Improved Beneficiary Outcomes in Medicare Advantage, HMA Principal Greg Gierer will facilitate a conversation on the evolving landscape of MA rates and supplemental benefits, with experts Melinda Buntin, Health Economist and Bloomberg Distinguished Professor at the Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins Carey Business School; Mark Fendrick, Director of the University of Michigan’s Center for Value-Based Insurance Design, and Matt Kazan, Vice President of Policy and Government Affairs at the SCAN Group.
Caprice Knapp, a seasoned health economist with over 20 years of experience in Medicaid and healthcare policy, shares her journey through various roles in government, academia, and private insurance. In this episode, Caprice offers a unique perspective on the challenges of measuring quality in healthcare, the importance of data-driven decision-making, and how global healthcare models can inspire innovation in Medicaid. From pediatric palliative care to cost-effective policy solutions, Caprice sheds light on how improving quality of care can transform healthcare outcomes for vulnerable populations.