1314 Results found.

Driving change in healthcare delivery: HMA Spring Workshop shapes policy and strategy frameworks for value-based care implementation
Federal policy frameworks establishing alternative payment models in Medicare and Medicaid have been the kick-starter of value-based care (VBC) innovation in healthcare delivery. However, employers provide health insurance to most Americans, and very few employers – with the exception of jumbo, self-insured employers – have leaned heavily into VBC. Small- and medium-sized firms rely on brokers to find an affordable health insurance plan, and often lack the resources required to negotiate more. Though the tide has been changing, our fragmented payment system has yielded only a subset voluntarily taking substantial risk for patient outcomes.
It has been said that to truly transform our American healthcare system to pay for value – improved outcomes for lower cost – it would require better alignment across public and commercial payers to support care providers in shifting their business models to take risk.
Quality and cost information are critical to implement VBC payment and delivery systems. Federal initiatives in Medicare and Medicaid have opened the door for providers, payers, and innovators to use health information to improve outcomes, with patients more engaged and more in control; the “Universal Foundation” announced by the Centers for Medicare and Medicaid Services (CMS) in 2023 seeks to align quality measures across the more than 20 CMS quality initiatives; and policies included in the 21st Century Cures Act and CMS Interoperability and Patient Access rule are creating more transparency on price and quality.
By enabling an infrastructure to measure, digitize, and share cost and quality information, federal and state governments have set the stage for greater collaboration among all purchasers – including employers – and the healthcare delivery system to redesign care that addresses health related social needs and behavioral health, ensuring that healthcare is provided equitably and sustainably. As the care delivery system is better able to deliver high value care, more employers will demand this for their workforce to provide a better benefit to their workers.
These issues, and more, will be a part of the expert-led conversation on VBC at HMA’s 2024 Spring Workshop March 5-6, in Chicago. This workshop offers a unique opportunity for payers, government officials, community organizations, vendors, and providers to have an unvarnished conversation about the challenges, lessons, and opportunities in implementing VBC. The meeting is designed to share insights, change-oriented strategies and actions that advance VBC from top industry experts, health plan executives, state and federal leaders, and policy experts.
Our working sessions will feature solutions-focused conversations among peers:
- Care delivery measures that drive outcomes, equity, population health
- Payment & risk management models for payment, pricing, attribution
- Data that is interoperable, consumer focused, deploying technology that is aligned to deliver on strategic objectives
- Policy & Strategy Frameworks at federal, state, and local levels that incentivize VBC
The closing panel will look at ways to take action through policy and collaboration to move our industry toward more sustainable approaches to healthcare payment and delivery.
To learn more and register for this unique event, please visit HMA’s 2024 Spring Workshop page. Act fast – online registration ends Wednesday, February 28!

Expanding Access to High Quality Sexual Health Care and STI Prevention
In 2022, more than 2.5 million cases of syphilis, gonorrhea, and chlamydia were reported in the United States. There were alarming increases in syphilis cases in particular – there has been an 80% rise in syphilis cases since 2016 and in 2022, there were 3,755 cases of syphilis among newborns reported (163% increase since 2018). While sexually transmitted infections (STIs) occur in all populations, some groups are more affected, including young people, gay and bisexual men, transgender individuals, and pregnant people. There are deep inequities in the rates of STIs including disproportionate rates among racial and ethnic minorities which are the result of longstanding social and economic structural inequities.
Sexual health services are being threatened and have inequitable resources which further complicates care for those individuals with lived experience with STIs, HIV, and viral hepatitis. They often experience additional and intersecting sexual health, behavioral health, and social needs that must be addressed concurrently.

HMA brings together experts from a full spectrum of sexual health services including policy, clinical, operations, and research.
Our experts have significant experience with conducting needs assessments and gap analyses, supporting syndemic (HIV/STI/Hepatitis) planning, centering health equity, and leveraging policy and research findings to maximize impact and access. A syndemic is a situation in which two or more interrelated biological factors work together to make a disease or health crisis worse.
Illustration from the Centers for Disease Control and Prevention (CDC)
We work with clients to reach shared goals of supporting sexual health, expanding access to screening, vaccines and other preventative services, reducing high rates of STIs including HIV, and addressing deep and persistent racial disparities in STI rates and the inequities that drive them.
We can help organizations including:
State and municipal departments of health and public health
Health plans
Community-based organizations (CBOs)
Behavioral Health Service Organizations
Federally Qualified Health Centers
Title X Clinics
Planned Parenthood affiliates and other free-standing women’s health centers
Foundations
Associations and Coalitions
Our sexual health experts include:
Former senior officials from the Health Resources and Services Administration and the Center for Disease Control and Prevention.
Advocates and former senior leaders of community-based organizations, foundations, and other programs that support healthcare systems capacity to implement quality STI prevention, screening, diagnosis, surveillance, and treatment.
Clinicians with experience providing sexual health services and building programs at the intersection of sexual health, behavioral health, primary care and maternal and child health.
Social workers and behavioral health professionals working to integrate approaches that address social and behavioral health needs.
Program development, strategic planning, and technical assistance experts working to implement innovative solutions and evidence-based guidelines.
Researchers and evaluators with extensive experience examining the implementation and impact of policy and operational changes on sexual health services.
Our experts can support your work to expand equitable access to sexual health care.
With offices in more than 30 locations across the country and over 700 multidisciplinary consultants with a wide spectrum of industry experience, and longstanding expertise in all 50 states, HMA has experienced staff in syndemic needs assessments and planning, program evaluation, research and analysis, strategic/business planning, clinical services, stakeholder engagement, quality improvement, and workforce development. Our portfolio of companies also gives you access to actuarial, data analytics and communications expertise, and more.
OUR WORK
South Carolina Department of Health and Environmental Control (DHEC) contracted with HMA to conduct a statewide gap analysis to document the array of partner services and disease intervention STI inside and outside the department and identify gaps and duplication to improve services and strengthen the program. As part of this engagement, HMA conducted an analysis of South Carolina’s STI delivery system, staffing capacity and processes, and developed a service location map to highlight gaps and inequities. The final report summarized findings and included recommendations for closing gaps in service delivery, workforce development and improving the efficiency and effectiveness of service delivery.
HMA supported the Washington State Department of Health’s Office of Infectious Disease in taking a syndemic approach to ending the HIV, STI, and viral hepatitis epidemics. A key activity of this project included supporting the Office of Infectious Disease to establish a new planning body that reflects the populations served by transforming their Statewide HIV Planning Group and launching a new communicable disease (syndemic) planning group. This work included conducting research on other statewide planning group structures, collecting community and stakeholder input, developing and operating structure, charter, and bylaws; recruiting and onboarding a diverse membership; and creating organizational change management, all with a focus and commitment to advancing racial equity. Through this work, HMA also drafted the state’s integrated HIV Prevention and Care Plan and Requests for Applications to help distribute state funds to local intervention efforts that advance the goals of this plan.
As part of our extensive area of work in strategic planning with state and local agencies, providers of health and human services, community-based organizations and many more, HMA has worked with clients that provide sexual and reproductive health care services to assess potential opportunities and approaches for expansion, delivery, and financing of care to reach underserved communities.
HMA worked with the Wyoming State Department of Health to conduct their HIV needs assessment and developed their Integrated HIV Prevention and Care Plan. This work included collecting and analyzing data on HIV incidence and prevalence; developing HIV, STI, and viral hepatitis ecosystem maps; facilitating workgroup meetings; collecting additional community and stakeholder input through provider and community surveys and focus groups; and developing a written report of the assessment findings, all with a focus and commitment to advancing health equity.
HMA worked closely with the Boston Public Health Commission to conduct an extensive HIV needs assessment. Activities included key stakeholder interviews, focus groups, surveys and data collection and analysis. Emphasis was placed on the intersection of HIV and drug user health.
HMA team members developed and implemented professional development training series entitled “The Intersection of HIV and SUD” on behalf of the Minnesota Department of Health. The 12-hour curriculum was developed in partnership with several community organizations representing Tribal, African American, and LGBTQIA+ communities. The training is delivered virtually and includes topics such as: understanding HIV; HIV risk reduction; SUD harm reduction; chemsex; HIV and stigma, pregnancy and HIV; and cultural, racial and sexual identities.
Contact our experts:

Julie Rabinovitz
Principal

Charles Robbins
Principal

Webinar replay: Compassionate Overdose Response Summit and Naloxone Dosing Meeting
The Compassionate Overdose Response Summit and Naloxone Dosing Meeting, held on March 18-19, 2024, was a two-day summit where naloxone experts built consensus on the definition of a compassionate bystander overdose response.
Day 1 (March 18) was an invitation-only for a small group of researchers, people with lived experience of overdose, those who have reversed multiple overdoses, and medical providers tasked with drafting an issue brief that will be the basis for the remainder of the summit.
Day 2 (March 19) was an open virtual summit. On this day, we shared the issue brief with the audience for feedback and host multiple presentations that covered emerging research on this topic, including:
- The impact of different naloxone doses and formulations on people who receive them
- The role of oxygen in community overdose response
- Communication strategies for bystander overdose response steps
The event produced clear guidance on naloxone dosing and the role of oxygen in overdose response:
- There is no real-world evidence for high-dose or long-acting opioid antagonists; therefore, until there is community experience with those regimens, they should not be included in standing orders or made available for broad community use.
- Rescue breathing is standard overdose response protocol and should be included in educational materials and training.
- People who use drugs must be central to the design, development, purchasing and distribution of all overdose reversal products
Additional materials from this event are below:
- Compassionate Overdose Response Summit Agenda
- Missouri’s Overdose Field Report: Naloxone dosing remains stable despite concerns otherwise
- Understanding negative reactions following overdose reversal with naloxone
- Examination of Naloxone Dosing Patterns for Opioid Overdose by Emergency Medical Services in Kentucky during Increased Fentanyl Use from 2018 to 2021
- Two decades of data: Insights from syringe service participants and EMS
- Scope of international research and what are the next research questions
For justification for the above statements or for questions, please contact Erin Russell.
HMA keynote speakers preview themes and imperatives for March 5-6 value-based care workshop
HMA’s Spring Workshop on Value-Based Care, March 5-6 in Chicago, is just a few weeks away. Listen to why our speakers are so excited to engage with attendees on value-based care.
Elizabeth Mitchell, CEO, Purchaser Business Group on Health will deliver the keynote speech on “The Purchaser’s Dilemma: Why Employers Should Demand Value (and Why They Don’t).”
Our March 5 dinner headliner Katie Kaney, CEO of LovEvolve will discuss her “Whole Person Index” and how we can collaborate in new ways to transform the healthcare system to deliver better health at a lower cost for all.


Hurry – online registration ends February 28!
Interoperability and patient access final rule: the next phase in the data exchange journey
This week, our In Focus section reviews the Centers for Medicare & Medicaid Services (CMS) Interoperability and Prior Authorization Final Rule, published on January 17, 2024. This is CMS’s latest effort to flesh out regulations mandating payer interoperability and fully electronic prior authorization (PA) policies. The 2024 final rule also represents a new phase in the agency’s work to advance interoperability as it moves beyond policymaking focused on building interoperable systems to policies centered on the applications and usage of shared data.
The new requirements affect a large segment of the nation’s public health insurance programs, including Medicare Advantage (MA) organizations, state Medicaid fee-for-service (FFS) programs, state Children’s Health Insurance Program (CHIP) FFS programs, Medicaid managed care plans, CHIP managed care organizations, and qualified health plan (QHP) issuers on the federally facilitated exchanges (FFEs). These payers must implement and adhere to Health Level 7® (HL7®) Fast Healthcare Interoperability Resources® (FHIR®) application programming interfaces (APIs). These APIs were developed by the DaVinci project and the CARIN Alliance which are both HL7 FHIR accelerator programs. Leavitt Partners, an HMA company, leads the work of the CARIN Alliance.
The final rule demonstrates a commitment to information sharing across the industry landscape and confidence in the FHIR standard to support health data exchange across all required APIs. Ultimately, FHIR APIs are creating a more patient-centered data ecosystem that can provide a tangible return on investment.
Following are details about the requirements, opportunities, and next steps for stakeholders.
Prior Authorization API and Process
Payers must build and maintain PA APIs by January 1, 2027, allowing providers to ask payers whether PA is required for a patient’s procedure, what documents must be submitted to attain authorization, and to receive the final decision and reason for denied requests electronically within a specified timeframe (seven days for standard procedures and three days for expedited decisions).
The rule finalizes requirements for the PA process, regardless of whether the payer receives the PA request through the Prior Authorization API. Specifically, CMS is requiring that:
- Affected payers send notices to providers when they make a prior authorization decision, including a specific reason for denial when they deny a PA request
- Payers, other than QHP issuers on the FFEs, respond to prior authorization requests within specific timeframes
- Affected payers publicly report certain metrics about their PA processes
These prior authorization process requirements become effective January 1, 2026. The last 12 months of PA information also must be shared with patient, providers, and other payers when the member switches a plan through the respective APIs.
To promote adoption of electronic prior authorization processes, CMS is adding an Electronic Prior Authorization measure for Medicare clinicians who participate in the Merit-based Incentive Payment System (MIPS) and hospitals and critical access hospitals in the Medicare Promoting Interoperability Program as an attestation measure.
Payer to Payer FHIR API
To support continuity of care and value-based programs, payers must be able to send, receive, and incorporate enrolled member data from previous and concurrent payers if members are dually enrolled.
To comply with the new electronic data sharing, the final rule requires payers to build and use FHIR API by January 1, 2027. Payer-to-payer (P2P) data sharing will include the last five years of claims/encounters, clinical data, and the active and pending PA requests. The data collected through the P2P APIs will need to be available to the other APIs (i.e., provider, patient, and prior authorization). The rule requires payers to request data from previous payers within a week after the patient opts in to sharing data. For dually enrolled members, data sharing will incur at least quarterly.
Patients must opt in and agree to the P2P data sharing. To this end, health plans must adjust their enrollment administrative process to allow members to easily share previous and concurrent payer information and consent to data sharing. CMS allows Medicaid or CHIP agencies to contract with entities, such as Health Information Exchanges (HIEs), for the digital access and transfer of a patient’s medical records, which supports the Payer-to-Payer API.
Provider Access FHIR API
Payers also must build and maintain a Provider Access API to share patient data with in-network providers with whom the patient has a treatment relationship, enabling continuity and coordination of care, by January 1, 2027. Affected payers must maintain an attribution process to associate patients with the appropriate in-network providers responsible for the patient care. The data from the payer via the Provider Access API must be added to a provider’s electronic health record, practice management solution, or any other technology solution that a provider uses for treatment purposes.
The Provider Access API includes the same data covered in the Payer to Payer Access API (claims/encounters, clinical data, and prior authorizations). The payer has one business day to deliver the required information. Payers must offer a mechanism for members to opt out from making their data available to the attributed providers.
Patient Access FHIR API
The final rule further enhances patient access to data to improve their treatment and shopping experience. In addition to claims and clinical data, as of January 1, 2027, payers must make PA data available through the Patient Access API to inform patients on their plan’s PA process and the status of requests.
In addition, affected payers must report annual metrics about Patient Access API usage and data requests to CMS beginning January 1, 2026.
Key Considerations and Early Results
The rule presents a significant opportunity to improve patient experiences and outcomes and to address some of the administrative burden on clinicians. Though CMS made some adjustments to timeframes in the proposed rule, immediate attention is needed to evaluate technological solutions available to payers, assess gaps between current and future required state, and develop policies to comply with new requirements and measures reporting.
Commercial payers may also leverage the improved electronic data sharing but are not required to do so. CMS-funded payers must respond to any inquiries from commercial payers and must require commercial payers to provide the same information as affected payers. Commercial payers, state governments, and other stakeholders have an opportunity to collaborate around the electronic data exchange.
This rule may have positive downstream application to other areas beyond PA, including quality measurements, risk adjustment, and population health. Early adopters who have implemented the prior authorization APIs have, on average, recorded a 150% – 300% return on investment (ROI). The implementation of API-based prior authorization represents a demonstrable increase in efficiency and significantly reduced provider burden. Given the measurable ROI, state-based regional collaboratives being led by Leavitt Partners are forming between payers and providers to implement the core tenants of the CMS rule well in advance of the 2027 deadline.
Similar initiatives are taking place in the technology space, like the Digital Quality Implementers Community, which was recently convened by Leavitt Partners and National Committee for Quality Assurance (NCQA) to build industry readiness for transitioning to FHIR-based digital measurement that hinges on improved electronic data sharing
What to Watch
The HMA team will continue to analyze the CMS’s Interoperability and Patient Access rule in the context of other federal and state policy changes affecting MA organizations, Medicaid FFS programs, state CHIP FFS programs, Medicaid and CHIP managed care programs, and QHPs.
The work and opportunities afforded with the Interoperability and Patient Access final rule will be featured prominently at The HMA Spring Workshop: Getting Real About Transforming Healthcare Quality and Value, March 5-6. In addition to rich discussions, HMA and HMA companies, including Leavitt Partners and Wakely Consulting LLC, are available to support planning and implementation and related system redesign initiatives. If you have questions about these topics, contact our experts below.

February 14, 2024
Interoperability and Patient Access Final Rule: The Next Phase in the Data Exchange Journey
Webinar replay: Substance Use Disorder (SUD) Ecosystem of Care: Pivoting to Save Lives – Part 1
This webinar was held on March 14, 2024.
This was part 1 of our 3-part webinar series, “Substance Use Disorder Ecosystem of Care: Pivoting to Save Lives.” In this session, we provided an overview of the series and took a look at the services and support that comprise a system of care for people who are not yet in treatment. These services are often community-based and involve outreach, engagement, and meeting people where they are. As people enter treatment, experience relapse, or choose to move through different treatment modalities, health promotion and harm reduction can serve as a safety net to keep people continuously engaged.
Learning Objectives:
- Explain the differences between prevention, promotion, and harm reduction.
- Illustrate the primary goal of health promotion.
- Distinguish the continuum and role of health promotion related to stages of chronic disease: active, controlled, and relapse.
- Identify role of harm reduction as a health promotion activity in the public sector v. the harm reduction often carried out in CBO/non-profit sector.
Whether you are a healthcare professional, caregiver, or someone personally affected by substance use, this webinar offered a roadmap for navigating the complexities of the Substance Use Care Continuum, fostering hope and resilience in the pursuit of sustained well-being.
Watch previous webinars and register for upcoming webinars in the series.
CMS releases advance notice of changes to MA capitation rates and Part C/D payment policies
This week, our In Focus section reviews the Centers for Medicare & Medicaid Services (CMS) Calendar Year (CY) 2025 Advance Notice for the Medicare Advantage (Part C) and Part D Prescription Drug Programs published on January 31, 2024. Alongside the advance notice, CMS published draft CY 2025 Part D Redesign Program Instructions. This guidance includes CY 2025 payment updates as well as additional proposed technical and methodological changes to Medicare Advantage (MA) and Part D. CMS previously released a proposed rule in November 2023 that included proposed policy changes to MA and Part D for CY 2025.
The proposed payment policies signal CMS is working to ensure the stability of MA and Part D programs, while also addressing concerns about the appropriateness of payments to plans. Furthermore, CMS remains highly focused on the impact methodological changes could have on payment to plans that enroll beneficiaries who are dually eligible for Medicare and Medicaid services. Proposals to align quality measures across programs and strengthen the measures used to assess the quality of beneficiary experiences and services provide directional information on CMS’s plans for the forthcoming annual payment rules for 2025.
Following are highlights from the 2025 Advance Notice and Part D Redesign Program Instructions. The deadline for submitting comments is Friday, March 1, 2024. CMS will announce the MA capitation rates and final payment policies for 2025 no later than April 1, 2024.
Payment Impact on MA: CMS is projecting that federal payments to MA plans will increase on average 3.7 percent from 2024 to 2025. The increase reflects multiple factors, including growth rates in underlying costs, change in Star ratings, continued implementation of the new risk adjustment model and fee for service (FFS) normalization, and risk score trends. Actual impacts of the proposed payment policies will vary from plan to plan.
Risk Adjustment: CMS is proposing to continue its three-year phase in of the updated Part C risk adjustment model, first published in the CY 2024 Rate Announcement. In CY 2025, risk scores will be calculated by blending 67 percent of the risk score using the 2024 CMS hierarchical condition categories (HCC) risk adjustment model and 33 percent using the 2020 CMS-HCC risk adjustment model. In addition, the MA risk score trend is being calculated separately under each model, then blended by the respective percentage to determine a CY 2025 risk score trend of 3.86 percent.
CMS is proposing a new methodology for calculating the FFS normalization factor to accurately address the effects of the COVID-19 pandemic without excluding any years of FFS risk scores.
CMS also proposes to apply the statutory minimum MA coding pattern difference adjustment factor of 5.90 percent for CY 2025.
Frailty Adjustment for FIDE SNPs and PACE Organizations. For CY 2025, CMS is proposing to blend the frailty score calculated for fully integrated dual eligible (FIDE) special needs plans (SNPs) consistent with the phase-in of the 2024 CMS-HCC model. The FIDE SNP frailty score is the sum of:
- 33 percent of the score calculated with the 2020 CMS-HCC model frailty factors
- 67 percent of the score calculated with the 2024 CMS-HCC model frailty factors
CMS also intends to use only the full Medicaid frailty factors to calculate frailty scores for FIDE SNP enrollees in order to align with the requirement that FIDE SNPs must have exclusively aligned enrollment, meaning that enrollment in FIDE SNPs will be limited to full-benefit dually eligible individuals, beginning in CY 2025. CMS will use the frailty factors associated with the 2017 CMS-HCC model to calculate frailty scores for Program of All-Inclusive Care for the Elderly (PACE) organizations in CY 2025.
Star Ratings: CMS reiterates its plan to further implement the “universal foundation” of quality measures. CMS first announced this subset of metrics in 2023, with the goal of aligning a core set of metrics across the agency’s programs while continuing to allow for program specific measures. CMS reminds plans that beginning with the 2024 measurement year (2026 Star Ratings), the weight of patients’ experience, complaints, and access measures will be reduced from a weight of four to a weight of two.
CMS proposes several updates and refinements to the Star Ratings program, including:
- Retiring the Care for Older Adults – Pain Assessment (Part C) measure, starting as early as the 2025 measurement year
- Making changes to the Plan Makes Timely Decisions About Appeals and Reviewing Appeals Decisions (Part C) measures for cases submitted electronically to the independent review entity
- Adding Social Need Screening and Intervention (Part C) to the display page for the 2025 Star Ratings and giving notice that National Committee on Quality Assurance (NCQA) is evaluating the potential addition of a utilities insecurity screening and intervention rate for this measure in the future
- Adding Depression Screening and Follow-Up for Adolescents and Adults (Part C) and Adult Immunization Status (Part C) to the display page for the 2026 Star Ratings
- Updating the Members Choosing to Leave the Plan (Part C and D) measure for the 2026 Star Ratings
- Possibly adding the Initiation and Engagement of Substance Use Disorder Treatment (Part C) and Initial Opioid Prescribing for Long Duration (IOP-LD) (Part D) measures
- Revisions to the Care Coordination (Part C) measure, and other changes through future rulemaking
Part D Impact
The advance notice reviews the significant changes to the Part D benefit occurring in 2025 as required in the Inflation Reduction Act (IRA). The IRA’s Part D changes effective in CY 2025 include:
- Eliminating the coverage gap phase. A newly defined standard Part D benefit will consist of three phases: annual deductible, initial coverage, and catastrophic coverage. There is no initial coverage limit, and the initial coverage phase will extend to the maximum annual out-of-pocket threshold, after which the catastrophic phase begins.
- Setting the out-of-pocket threshold at $2,000.
- Sunsetting the Coverage Gap Discount Program and implementing of the Manufacturer Discount Program (Discount Program).
- Making changes to the liability of enrollees, plans, manufacturers, and CMS.
- Updating the definition of incurred costs to include, among other categories of costs, supplemental coverage and other health insurance, which was previously excluded. Manufacturer discounts provided under the Discount Program also will be excluded.
- Premium stabilization will continue to be in effect.
CMS is recalibrating the RxHCC risk adjustment model to account for IRA changes and is proposing to calculate separate normalization factors for risk scores used to pay MA-PD plans versus PDPs.
Key Considerations
The impact of the MA risk score trend on payment will vary across individual MA plans. Plans will want to analyze these effects to inform their comments to CMS.
In the advance notice, CMS emphasized the strong growth in the dual SNP market for 2024. This market continues to present growth opportunities. CMS has sought to ensure that changes to payment accuracy better reflect more recent cost and utilization patterns and the risk profile of the sickest and most complex enrollees. Plans will want to consider payment incentives in the context of major policy, reimbursement, and operational changes required to improve integrated care for dually eligible individuals. MA organizations considering becoming FIDE SNPs and wishing to obtain frailty payments in 2025 will need to understand the specific requirements to be eligible for such payments.
The HMA Medicare team will continue to analyze these proposed changes. We have the depth and breadth of expertise to assist with tailored analysis, to model policy impacts across the multiple rules, and to support the drafting of comment letters on this notice.
If you have questions about the contents of CMS’s MA Advance Notice and payment policies and how these would affect MA plans, including SNPs, providers, and Medicare beneficiaries, contact our experts below.
February 7, 2024
CMS Releases Advance Notice of Methodological Changes for MA Capitation Rates and Medicare Part C and Part D Payment Policies

HMA white paper examines expanding home care value through innovative client and caregiving supports
As the U.S. population ages, non-medical personal care services are increasingly important for supporting Americans to remain in homes, as the vast majority of them prefer. But in-home personal care services will remain in short supply throughout the country unless home care agencies have greater success recruiting and retaining caregivers. In this HMA white paper, we describe the programs developed by Help at Home, the nation’s largest personal care services providers with 53,000 in 11 states, to use technological solutions to increase ease of caregiver recruitment and to provide its caregivers with a greater sense of purpose and meaning in their work.
The latter accomplishment has been achieved through Help at Home’s innovative care management program, “Care Coordination at Help at Home,” in which its caregivers receive a weekly text asking them to complete a brief survey about their personal care client’s physical and behavioral health symptoms and any health-related social needs. This information is transmitted to the agency’s Clinical Support Team, composed of nurses, social workers, and community health workers, who review the caregivers’ observations and, if needed, conduct further evaluations of the clients and/or alert the appropriate primary care or specialty providers about their escalating health and social needs. The program’s outcomes: Decreased client utilization of Emergency Department visits and hospitalizations since brewing health concerns are addressed earlier on. Increased caregiver retention because caregivers feel like they are making a significant difference in the health and well-being of their clients.
Pennsylvania releases community HealthChoices (CHC) Medicaid managed care RFA
This In Focus section reviews the request for applications (RFA) that the Commonwealth of Pennsylvania Department of Human Services (DHS) released January 30, for the Community HealthChoices (CHC) Program. CHC is the mandatory managed long-term services and supports (MLTSS) program, which serves five CHC zones that cover all 67 counties in the commonwealth.
Notably, this procurement, as compared to the original CHC procurement in 2018, has increased emphasis on innovative approaches to address health equity and the Social Determinates of Health (SDOH). The health equity focus goes beyond traditional health-related social needs such as access to housing, transportation, food, and employment, and addresses some SDOHs that have a particular impact on the CHC population, such as environmental conditions and addressing hazardous or unsafe living conditions.
Behavioral health remains carved-out to separate behavioral health managed care organizations (BH-MCOs). Instead, CHC applicants will need to articulate how they will coordinate with the BH-MCOs to ensure access to appropriate BH services, which continues to be an area of significant interest for state Medicaid officials.
Background
The CHC Program serves individuals who are dually eligible for Medicare and Medicaid and people with physical disabilities who receive home and community-based waiver services or nursing facility care.
Participants may receive LTSS in the community or in a nursing facility.
CHC is the sole program option for fully dual eligible beneficiaries and most nursing facility clinically eligible (NFCE) individuals who reside in the five zones. The regional CHC zones are as follows:
- Southwest zone: Allegheny, Armstrong, Beaver, Bedford, Blair, Butler, Cambria, Fayette, Green, Indiana, Lawrence, Somerset, Washington, and Westmoreland counties.
- Southeast zone: Bucks, Chester, Delaware, Montgomery, and Philadelphia Counties.
- Remaining zones and respective counties, including
- Lehigh/Capital zone: Adams, Berks, Cumberland, Dauphin, Fulton, Franklin, Huntingdon, Lancaster, Lebanon, Lehigh, Northampton, Perry, York
- Northeast zone: Bradford, Carbon, Centre, Clinton, Columbia, Juniata, Lackawanna, Luzerne, Lycoming, Mifflin, Monroe, Montour, Northumberland, Pike, Schuylkill, Snyder, Sullivan, Susquehanna, Tioga, Union, Wayne, Wyoming.
- Northwest zone: Cameron, Clarion, Clearfield, Crawford, Elk, Erie, Forest, Jefferson, McKean, Mercer, Potter, Venango, Warren
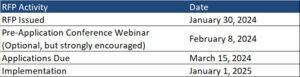
RFA
Medicaid managed care organizations (MCOs) may submit applications for one or more zones. Applications are due March 15, 2024. The department anticipates awarding agreements to three to five CHC-MCOs in each of the five CHC zones. Selected applicants must provide CHC services in all counties in the zone(s) for which they are selected to participate and improve the accessibility, continuity, and quality of services for participants in the CHC program. The contract will run for five years and will have three one-year renewal options.
DHS indicates that the awarded CHC-MCOs must have an aligned dual-eligible special needs plan (D-SNP) and a current Medicare Improvement for Patients and Providers Act (MIPPA) agreement with the department. The aligned D-SNP must be operational and the MIPPA agreement must be in place by the anticipated implementation date (January 1, 2025).
DHS indicates selected MCOs must be as flexible and adaptable as possible and demonstrate the ability to coordinate services for multiple populations and across multiple programs, including programs with a focus that is broader than the delivery of healthcare services and LTSS.
Other RFA highlights include the following:
- Does not require a cost submittal.
- Includes small diverse business (SDB) or veteran business enterprise (VBE) goals of 11 percent and 3 percent respectively. Applicants must include separate SDB and VBE submittals for each zone in its application.
- Includes a contractor partnership program (CPP) which requires entities that are awarded a contract or agreement with DHS to establish a hiring target to support Temporary Assistance for Needy Families (TANF) beneficiaries in obtaining employment with the contractor, grantee, or their subcontractors.
Notably, DHS has provided itself flexibility within the RFA to implement a pay-for-performance incentive to MCOs. Under this policy, DHS could make incentives available to MCOs that help participants successfully complete the financial eligibility redetermination process with their local County Assistance Offices (CAOs). The department may implement additional pay-for-performance incentives in later years.
Timeline
Evaluation
For an applicant to be considered responsible for this RFA and eligible for selection of best and final offers (BAFOs) and negotiations:
- The total score for the technical submittal of the application must be greater than or equal to 75 percent of the available raw technical points
- The applicant’s financial information must demonstrate that the organization possesses the financial capacity to fulfill the good faith performance of the agreement
The evaluation committee will evaluate technical submittals for each zone separately. For each zone, DHS must select for negotiations the applicants with the highest overall score. The weight for the technical criterion is 100 percent of the total available points. Technical evaluation will be based on soundness of approach, applicant qualifications, personnel qualifications, and understanding the project.
The final technical scores will be determined by giving the maximum number of technical points available to the application with the highest raw technical score. The remaining applications will be rated by applying the formula located at RFP Scoring Formula.
Financial information will not be scored as part of the technical submittal. It will be reviewed only to determine an applicant’s financial responsibility.
SDB and VBE participation submittals will not be scored, however, if an applicant fails to satisfy the SDB or VBE requirements described, and DHS will reject the application.
DHS will not score the CPP submittal. Once an applicant has been selected for negotiations, DHS will review the CPP submittal.
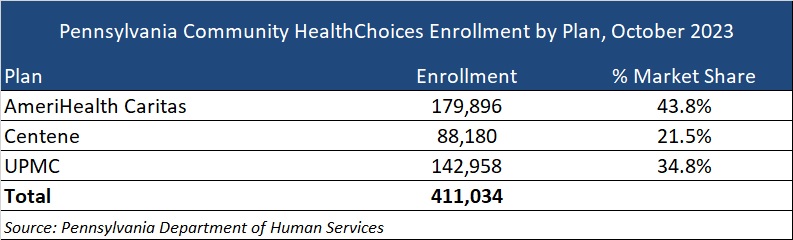
Current Market
The CHC incumbents are AmeriHealth Caritas, Centene, and University of Pittsburgh Medical Center (UPMC), serving 411,034 CHC members as of October 2023.
DHS has published a historical data summary for the CHC program along with other DHS reports at: Community HealthChoices Historical Data.
Link to solicitation: All files on PA eMarketplace
Want to know more about how the next phase of Community Health Choices will impact your organization?
HMA’s Pennsylvania-based teams can assist organizations seeking to understand the implications of this important procurement, key program changes and what the outcome may mean for providers, community base organizations, and other stakeholders. Please contact Dianne Bisacky with questions or if you are seeking more detailed analysis of this procurement or the Community Health Choices program generally.
Nine States to Participate in Children’s Behavioral Health Policy Lab
LANSING, MICH. – Health Management Associates (HMA), in partnership with the Annie E. Casey Foundation, Casey Family Programs, National Association of State Mental Health Program Directors (NASMHPD), the Child Welfare League of America (CWLA), the American Public Human Services Association (APHSA), National Association of Medicaid Directors (NAMD) and the Centene Foundation, will convene a Children’s Behavioral Health (CBH) State Policy Lab, Feb. 7-9 in Baltimore. HMA today announced that Georgia, Kansas, Kentucky, Maryland, Missouri, Pennsylvania, Texas, Utah, and Wisconsin will participate in the policy lab. MITRE, which previously hosted a related federal convening, will also take part in this state convening.
This pioneering effort, made possible by the partner organizations, aims to convene state interagency teams – including child welfare, juvenile justice, behavioral health, Medicaid, and K-12 public education – to collectively strategize, learn from innovators in the sector and promote cross-system alignment to drive outcomes for children, youth, and families.
COVID-19 has exacerbated long-standing system collaboration challenges across state child welfare, behavioral health, and Medicaid that lead to unsatisfactory outcomes for the most vulnerable children in our communities. Most worrisome is the worsening of behavioral and physical health challenges and trauma because of uncoordinated or fragmented care. This lack of coordinated strategy and policy leads to higher costs of treatment and also increasingly exposes states and local jurisdictions to threats or filings of class action lawsuits, and related settlements or those arising from Department of Justice investigations. Fortunately, federal and state efforts and investments to address the youth systems of care – including schools, community, delivery systems, and community-based child placing agencies – are in motion.
In November, a call for applications was released to U.S. states and territories for potential participation in the State Policy Lab. Applicants were required to identify demonstrated need, existing state agency governance structures focused on children and youth, technical assistance needs, and outcomes for attending the policy lab. The applications required demonstrated participation from Medicaid, child welfare and behavioral health agencies; a commitment to creating sustainable interagency solutions for children, youth, and their families and had to certify formal support from the Governor/Cabinet level.
An external independent panel reviewed applications for state agency participation using a standardized rubric that covered four domains:
- Gaps and opportunities analysis
- Intent of collaborative partnerships
- Approach to engagement of youth and adults with lived experience
- Imminent risks to public agency operations as a result of poor outcomes for children, youth, and their families
This convening is aimed at assisting child welfare, juvenile justice, behavioral health, Medicaid, and K-12 public education where possible to build upon existing efforts to improve outcomes for children, youth, and families, strategically layering on missing components and promoting alignment between them and with other agency priorities. Examples of what could be co-designed with state partners:
- Build a shared strategic vision for a comprehensive continuum of care that ensures access to the “right service, at the right time based on individual and family need.” This vision can strengthen prevention initiatives and ensure the full array of evidence-based community-based interventions including use of crisis response and stabilization models.
- Develop policies and strategies for improving the engagement of children, youth, and families with lived experiences to the “right part of the system for the right level of care,” agnostic of the door through which they enter any coordinated child serving system, while ensuring that all aspects of this system are anchored in equity.
Following the event, learnings and findings will be disseminated to help states and counties adopt innovative solutions to improve outcomes for children, youth, and their families.
For more information email: [email protected]