HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
This report presents an independent landscape analysis by Health Management Associates (HMA) examining Medicaid coverage of breastfeeding services and supplies in six states: Arkansas, Colorado, Kansas, North Carolina, Oregon, and Vermont. The analysis explores the availability and implementation of lactation consultation services and breast pump benefits within these state Medicaid programs, based on policy reviews and interviews with key stakeholders. Participants included state Medicaid officials, WIC representatives, lactation providers, managed care organizations, community-based organizations, and breastfeeding experts.
Findings reveal persistent barriers to access, inconsistencies in policy execution, and implementation gaps. The report highlights effective practices currently in use and offers targeted policy recommendations to enhance service delivery, promote equitable access, and improve maternal and infant health outcomes. This analysis serves as a strategic resource for stakeholders seeking to strengthen Medicaid’s role in supporting breastfeeding families.
Earlier this month colleagues from Health Management Associates (HMA) attended the 2025 Ohio Rural Health Association Conference. The gathering brought together providers, policymakers, and advocates from across the state to discuss one of the most pressing issues of our time: the future of rural health care in an uncertain policy and financial environment.
At a moment when federal funding and regulatory debates dominate the headlines, what stood out most was the energy and commitment among local leaders to work together on practical solutions. The challenges facing rural communities are profound—hospitals and clinics strained by reimbursement shortfalls, workforce shortages threatening access, and shifting payer dynamics creating new administrative burdens. Yet the conversations throughout the conference were grounded in resilience and collaboration, demonstrating that sustainable solutions begin at the community level.
Spotlight on Collaboration
HMA was honored to contribute to this dialogue through three sessions focused on core issues shaping rural care.
Kenneth Cochran, DSc, RN, FACHE, drew on his deep leadership experience as a former Ohio hospital CEO to highlight the urgency of workforce development. With projections of a 187,000-physician shortfall by 2037, Ken outlined integrated workforce strategies—apprenticeships, housing partnerships, and a culture of continuous learning—that can help stabilize rural hospitals and strengthen community health infrastructure.
Courtney Smith, RHIT, CCS, shared two critical perspectives. First, she unpacked the growing strain of Medicare Advantage in rural communities, where reimbursement often falls short and administrative requirements delay patient care. Second, she explored the complexities of Medicaid revenue cycle management, offering actionable steps rural providers can take—from leveraging technology and analytics to streamlining wrap-around payment reconciliation—to maintain stability in an unpredictable environment.
Jennifer Shaw, Senior Consultant, co-presented on best practices for navigating payer relationships with Courtney. She underscored how rural providers can use data to strengthen negotiations and how collaboration across hospitals, clinics, and associations creates the leverage necessary to ensure fair treatment in contracting and payment.
These discussions demonstrated the value of having clinical, operational, and policy perspectives at the table. Each HMA colleague brought not only technical expertise but also a deep appreciation for the lived realities of rural providers, ensuring our sessions were rooted in practicality.
A Landscape in Flux
The national policy context reinforces the importance of this work. Recent debates in Washington over rural health funding underscore just how fragile the financial footing of many hospitals and clinics can be. While the outcome of federal policy is uncertain, what is clear is that communities cannot afford to wait.
As HMA has noted in our broader work on rural health, effective solutions hinge on collaboration across sectors and levels of government. Whether it’s building workforce pipelines, ensuring fair payment, or streamlining operations, progress requires alignment among providers, payers, policymakers, and communities themselves.
Moving Forward
The Ohio Rural Health Association conference was a reminder that even in uncertain times, there is a powerful foundation for innovation and problem-solving when rural providers work together. HMA is proud to support these efforts, bringing decades of experience in Medicaid policy, health system transformation, and rural health strategy to bear for our partners.
As we look ahead, one lesson stands out: the path forward for rural health will not be written in Washington alone. It will be forged in places like Ohio, where providers, leaders, and communities are building practical, collaborative solutions every day.
Ohio Health Policy Snapshots
Sign up for Ohio Health Policy Snapshots delivered right to your inbox
President Trump signed an executive order (EO), Ending Crime and Disorder on America’s Streets, on July 24, 2025, signaling a significant shift in federal homelessness policy and the requirements for organizations that use federal dollars to address homelessness in their communities. The order emphasizes public safety and prioritizes institutionalization and mandatory treatment over housing first approaches.
The administration asserts that “the overwhelming majority of these individuals are addicted to drugs, have a mental health condition, or both” and calls for transitioning homeless individuals into long-term institutional settings through civil commitment for “humane treatment.” Below, Health Management Associates (HMA) outlines key elements of the EO, including provisions, key stakeholder considerations, and potential strategies to maintain care continuity amid federal changes.
Key Elements of the Executive Order
End of Housing First: The EO discontinues support for the Housing First model, directing federal agencies to prioritize mandatory treatment. The Department of Housing and Urban Development (HUD) Secretary is directed to take steps requiring treatment participation as a condition of HUD program participation.
Support for Civil Commitment Infrastructure: The federal government will assist state and local governments with technical guidance, grants, and other resources to implement civil commitment, institutional treatment, and step-down treatment standards. The Attorney General and US Department of Health and Human Services (HHS) Secretary are instructed to pursue reversal of legal precedents that restrict civil commitments for individuals with mental illness who pose risks or are unable to care for themselves.
Restructuring Federal Programs: The EO directs HHS, HUD, and the Departments of Justice (DOJ) and Transportation (DOT) to review discretionary grants and restructure programs to ensure compliance with the new guidelines, as outlined below.
HHS Substance Abuse and Mental Health Services Administration (SAMHSA) grants will no longer support harm reduction or safe consumption efforts and has issued a “Dear Colleague” letter clarifying which services will be funded; for example, naloxone distribution can be funded, but clean syringe distribution cannot.
HUD will exclusively, where permissible, fund programs for women and children and revise regulations to exclude registered sex offenders.
Some emergency law enforcement funds may be allocated for encampment removals.
Expanded Roles: The EO directs HHS to leverage the use of federally qualified health centers (FQHCs) and Certified Community Behavioral Health Clinics (CCBHCs) to reduce homelessness and ensure federal funds support crisis intervention and comprehensive behavioral health services. In addition, the Attorney General is directed to prioritize funding for the expansion of drug and mental health courts.
Notably, federal grants will prioritize jurisdictions and states that enforce laws against open drug use, urban camping, urban loitering, and urban squatting. Grant recipients must also share certain health-related data with law enforcement, as permitted by law.
Considerations for Stakeholders
States, local governments, and county jurisdictions must assess housing and homeless programs that use federal funding streams. They must consider the implications of their current program activities and, where possible, realign programs with new requirements. They may gain access to new funding for treatment beds, drug and mental health courts, crisis response, and law enforcement support but risk losing funding for those programs that use harm reduction or housing first models. Local governments could face increased jail overcrowding and legal challenges related to civil commitments and data sharing. Early examination of current programs, particularly HUD and crisis programs, as well as early planning, will be essential.
Providers may need to restructure services to comply with the new mandates, including collaboration with crisis/removal entities and law enforcement and expanded reporting. Emergency department and inpatient facilities may see increased demand, especially from uninsured individuals.
State behavioral health authorities and other stakeholders can benefit from forming advisory councils to develop ethical frameworks for civil commitments, as well as consider providing training for providers and law enforcement and propose revisions to state statutes and regulations
Homeless individuals are likely to experience increased policing, institutionalization, and loss of access to non-mandated services and housing.
What Happens Next
Federal agencies are now responsible for implementing the EO, revising grant programs, issuing guidance, and shifting funding priorities toward enforcement and institutional treatment. These changes will redefine compliance for local governments and service providers.
Health and housing organizations must quickly assess the implications of this policy shift. Strategic collaboration across sectors, including behavioral health, housing, law enforcement and judicial systems, will be essential to maintain care continuity and protect individual rights.
Connect with Us
HMA’s housing and homelessness and behavioral health experts are closely monitoring the evolving federal policy landscape and legal developments. We are tracking federal funding shifts, priorities, and opportunities across HHS, HUD, DOJ, and DOT, helping stakeholders align their programs with new priorities to enhance eligibility and impact.
For details about federal agency implementation of the EO and downstream effects, contact our featured experts below.
Imagine a 77-year-old man named Don who lives alone in his small apartment after his wife, Marcia, suddenly died a year ago. She had been his constant companion and long-time caregiver, making sure he took his medications for diabetes and bipolar disorder. Now he is socially isolated, lonely, and depressed. When he neglects to eat, his blood sugar levels tend to drop, and he becomes light-headed. He won’t call his doctors then; he doesn’t want to bother them. Besides, it was his wife who used to communicate with his doctors and psychiatric team about any concerns. Without her, he doesn’t have much motivation to do anything.
Don illustrates several U.S. demographic and epidemiologic trends:
He is a “Baby Boomer” driving the ongoing aging of this country. Within the next 20 years, the number of Americans aged 65 and over will exceed the number of those under 18. The population of working age, including those available to care for older adults, will decline by 5 percent. As a result, the emerging care gap between the numbers of Americans who need care and those who can provide it will greatly increase.
Like greater numbers of older Americans, he has at least two chronic illnesses, adversely affecting his overall functioning and quality of life. According to a 2025 Centers for Disease Control research summary, chronic conditions put him at risk for higher healthcare costs[1]. The combination of chronic physical and mental health conditions will likely mean very high health care costs.
Like increasing numbers of older Americans, he has a behavioral health disorder. About 25% of older adults have a diagnosable mental, substance use, and/or cognitive disorder. These conditions are often exacerbated by social isolation and loneliness, which is associated with increased rates of both mental and physical health problems.
Unfortunately, about half of older adults with mental or substance use disorders do not get treatment or are treated by primary health care providers who have limited training in addressing geriatric psychiatric concerns. As a result, only about a third of people who get treatment receive what is “minimally” adequate treatment. Only about half of those who get treatment from mental health professionals receive adequate care.
The low utilization by older Americans of behavioral health services reflects several access challenges including:
Access to providers who are clinically, culturally, linguistically, and generationally competent are in short supply. The shortages are most acute for rural residents. There is also a shortage of geriatric mental health professionals participating in the Medicare program.
Service access is also problematic. Many treatment programs are in hard-to-reach locations. There is also a tremendous shortage of services in home and community settings, due to workforce shortages.
Discrimination including stigma and ageism, plus the lack of awareness about mental illness and the effectiveness of treatment result in reluctance to seek or accept behavioral health services.
Unlike many of his contemporaries suffering from a behavioral health condition, Don does have long-standing behavioral health treatment which has been effective for most of his lifetime for managing his bipolar disorder. But without his wife’s support, his attendance and adherence have faltered. He now needs other sources of support and guidance, as well as more intensive treatment, or he faces several major risks:
He may wind up being taken by ambulance to hospital emergency rooms for falls. *
He may be admitted to the hospital for broken bones, diabetic complications, or even a stroke or heart attack.
He may deteriorate further and become unable to care for himself, eventually transferring from a hospital to a long-term care facility.
He may suffer premature death.
Older Americans, like Don, need not suffer injury and decline in addition to grievous loss. With the right systems of behavioral health, supported by care coordination and person-centered care plans, they can recover, adapt, and remain in their homes, as most Americans prefer.
HMA has the expertise to create and strengthen those systems of care. To learn more about How HMA Can Help.
[1] Watson KB, Wiltz JL, Nhim K, Kaufmann RB, Thomas CW, Greenlund KJ. Trends in Multiple Chronic Conditions Among US Adults, By Life Stage, Behavioral Risk Factor Surveillance System, 2013–2023. Prev Chronic Dis 2025;22:240539. DOI: http://dx.doi.org/10.5888/pcd22.240539
Addressing Behavioral Health Needs in an Aging Population
America’s healthcare and behavioral health systems are not adequately supporting the mental health and substance use needs of older adults. Unless improved with targeted and innovative policies and operational changes, those systems will do an even poorer job in the immediate future as our country rapidly ages. The result will be an increased number of older adults with untreated mental health disorders, cognitive disorders, and/or substance use disorders, increased rates of hospitalization and institutionalization, and vastly increased care costs.
Available statistics make clear the challenges:
The number of older adults in this country is expected to grow from approximately 56 million in 2020 to 85 million in 2050. Without substantial breakthroughs in treatment and prevention, the number of older adults with diagnosable mental disorders will increase from about 11 to 17 million and those who misuse alcohol and other drugs will increase from 2 to 3.5 million.
During those three decades, the number of Americans with dementia will also nearly double from 7 to 13 million. Many of these elders will have co-occurring behavioral health conditions, such as depression, anxiety, psychosis, and behavioral disturbances which will greatly strain family resources and coping.
If present performance is any predictor of the future, our systems of care now in place will not be able to handle the coming needs. Today fewer than half of older adults with mental or substance use disorders get any treatment at all because of limited-service capacity and access. Much of the care that is provided comes from medical and behavioral health providers without specific training or experience in older adult mental health and substance use disorders. The so-called digital divide—in which many older Americans are uncomfortable with telehealth or lack the equipment or bandwidth to use it—disproportionately impacts those with behavioral health disorders who live in rural communities and/or have limited economic means.
To adequately care for these vulnerable older adults, our approach and systems must change. That will require increased attention, investment, and thoughtful planning. Fortunately, there is clinical, operational, and policy expertise available to guide what will necessarily be a decades-long effort.
How HMA can help
HMA works with a range of clients. We work with federal, state and local governments, trade associations, provider organizations and community-based provider organizations (CBOs), delivery systems, managed care organization (MCO) plans, and philanthropic funders, to design, implement, and sustain effective models and systems of care for older adults with mental health and substance use needs.
We bring together a cross-sector, multidisciplinary team of experts in older adults’ needs and mental health and substance use focused on strategy, policy, clinical, operations, and finance systems. Our team members have rich backgrounds across government, payers and provider systems. We understand our clients’ needs because we’ve been in your shoes.
Develop mental health/substance use and aging coalitions
Policy, Planning & System Redesign
Plan state and local policy and system redesign
Incorporate mental health and substance use in multi-sector plans on aging and age-friendly communities
Build age friendly systems of health and mental health/substance use care
Integrated & Specialized Care Models
Establish integration models within and between systems
Implement care coordination/care transition models, including post-acute care
Develop housing models that integrate mental health and substance use care
Establish specialized models of care for older adults with serious mental illness and/or substance use disorders
Evidence-Based & Preventive Interventions
Embed evidence-based practices for older adult mental health and substance use needs
Design suicide prevention and crisis systems that supports older adults
Integrate psychoeducation for older adults and their families
Financing & Technology Infrastructure
Design financing and optimization of revenue models
Embed tech-enabled care solutions
Provider Access
Conduct workforce planning, including age-friendly training
Identify and implement caregiver support models
Design financing and optimization of revenue models
Discrimination and Awareness
Provide psychoeducation for older adults and their families
Service Access
Plan state and local policy and system redesign
Establish integration models within and between systems
Implement care coordination/care transition models, including post-acute care
Incorporate mental health and substance use in multi-sector plans on aging and age-friendly communities
Build age friendly systems of health and mental health/substance use care
Embed tech-enabled care solutions
Recent Project Examples
Strategic planning
An Area Agency on Aging (AAA) hired HMA to assess the needs of its client population and develop strategies to enhance behavioral health services and supports. The mental health and substance use needs of older adults, and especially those with both Medicaid and Medicare are among the highest. Through this project, the AAA focused on finding ways to expand service access to older adults. HMA prepared several recommendations to contract with health plans to help older adults access behavioral health services.
Multi-sector plans on aging development
A county hired HMA to help develop a multi-sector plan on aging. Multi-sector plans on aging provide an opportunity to address the unmet mental health and substance use needs of older adults. HMA analyzed relevant assessments and plans and facilitated broad community engagement to help shape the development of the plan.
Skilled nursing facilities practice improvement
A state health department hired HMA to enhance the quality of care of skilled nursing facility residents with substance use disorders. Many residents, including older residents, of nursing homes have unidentified and untreated substance use conditions. HMA delivered on-site technical assistance, in-person staff training, policy and procedure development, community partnership building, and regional forums to foster shared learning.
Affordable housing with integrated services sustainability
A long-term care trade association hired HMA to develop a braided financial and partnership service model to integrate health, mental health and social services to support aging in place. Integrated service and financial models can better support the often co-occurring physical, mental, and social needs of older adults. HMA conducted stakeholder engagement, service gap analysis, and strategic alignment to support the development of a sustainable service model.
Post-acute care guide
A state-level hospital association hired HMA to support its hospitals and their staff on post-acute care transitions. Post-acute care transitions are critical to ensuring that older adults have a successful recovery. These transitions are important for preventing complications after leaving an acute care setting like a hospital. The association hired HMA to create first-of-its-kind post-acute care (PAC) guides to support clinicians and family members to find post-acute care resources to address behavioral health needs.
Rural access to services for older adults
A foundation hired HMA to improve access to integrated care for older adults who were dually eligible for both Medicaid and Medicare. Older adults residing in rural communities have poorer access and outcomes than their urban peers. HMA created a toolkit of actionable solutions for state policymakers to address older adults’ mental health needs and social isolation conditions in rural communities.
Kim Williams is an experienced executive, policy leader and social worker with a record of transformational growth, accomplishment, and innovation … Read more
This week, our In Focus section highlights findings from Health Management Associates Information Services’ (HMAIS’s) review of 2024 statutory filings submitted to the National Association of Insurance Commissioners (NAIC). These filings provide a nationwide view of Medicaid managed care plan profitability and medical loss ratios (MLRs) across 221 plans operating in 39 states, the District of Columbia, and Puerto Rico.
These data build upon and offer additional context to a previous analysis conducted by HMA and Wakely, an HMA Company, of increasing post-pandemic financial pressures driven by acuity increases resulting from the continuous eligibility unwinding and increases in behavioral health and home and community-based services access and utilization.
Medicaid Managed Care Underwriting Gains and Losses
As state Medicaid programs have increasingly moved from fee-for-service to managed care, a foundational assumption has been that efficient managed care organizations (MCOs) reduce waste and deliver high quality, cost-effective healthcare services. This transition has made Medicaid plan performance and sustainability a central focus for policymakers and actuaries alike.
Medicaid capitation rates must be actuarially sound, which means they must be projected to cover all “reasonable, appropriate, and attainable costs,” including medical administrative costs, plus a margin for insurance risk, even for nonprofit plans. According to the Society of Actuaries 2024 research, average underwriting margins in Medicaid rates ranged from 0.35 percent to 3.15 percent, with a consistent average between 1.2 percent and 1.3 percent.
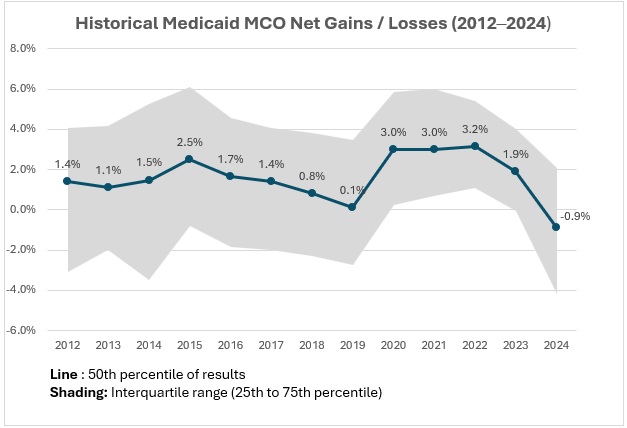
However, actual results often deviate from projections for reasons that may be challenging to predict. Rate setting is an inherently forward-looking process, and even with conservative assumptions, unexpected shifts in enrollment, acuity, or service utilization can lead to significant deviations from projected results. Retrospective reviews show variability in margins over time (see Figure 1).
Based on HMAIS’s analysis, Medicaid MCOs sustained modest but steady gains from 2012 through 2017. After a decline between 2016 and 2019, margins rebounded to approximately 3 percent until 2022, narrowed in 2023 to 1.9 percent, and turned negative in 2024 at -0.9 percent.
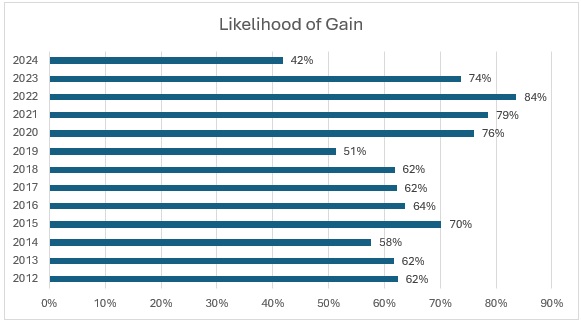
For the first time in over a decade, more plans experienced losses than gains in 2024 (see Figure 2), with only 42 percent reporting positive margins, down from the decade high of 84 percent in 2022. This shift raises critical questions about sustainability and participation in Medicaid managed care.
Figure 2. Medicaid Managed Plans Likelihood of Gain, 2012‒2024 (39 States, DC)
The “Likelihood of Gain” chart tracks the percentage of Medicaid managed care plans reporting an underwriting gain each year from 2012 to 2024. For most years, the likelihood that a plan posted a gain was relatively high, typically between 60 percent and 80 percent. The probability reached a recent peak in 2022, with 84 percent of plans reporting gains, and remained elevated in 2023 (74 percent). In 2024, however, the likelihood of gain dropped sharply to just 42 percent, the lowest level in the 12-year period.
Risk Corridors, Medical Loss Ratios, and Structural Policy Shifts
MLRs show the portion of plan revenue spent on medical care as compared with the costs to operate the plan and the underwriting gain or loss described previously. When MLRs rise or fall, it can be an indication that medical cost trends experienced by health plans differ from the assumptions used by state rate setting actuaries. High MLRs are the key driver of underwriting gains, and low MLRs are associated with higher profitability. All states report MLRs to the Centers for Medicare & Medicaid Services (CMS), and some enforce minimum MLRs with a remittance provision, requiring plans to return funds if their MLR goes below a certain level.
Risk corridors are another tool that states use to manage financial volatility. These mechanisms share gains or losses between plans and states when results deviate significantly from pricing assumptions, offering protection to MCOs and the state alike, in contrast to minimum MLR provisions with a remittance provision, which only protects the state. During the COVID-19 pandemic, many states implemented or expanded risk corridors to recoup overpayments because of lower utilization. Some risk corridors were set retroactively—a practice CMS now prohibits.
In 2024, MLRs reached a decade high of 90.8 percent, as indicated by HMAIS’s analysis. Driving this increase were heightened utilization rates, increased enrollee acuity, and the end of continuous Medicaid coverage protections in 2023. As healthier, lower-cost members left Medicaid, plans were left serving a more complex population with higher per-member costs. Inflation in medical costs—especially for behavioral health and home and community-based services—added more pressure. Delayed or avoided care during the COVID-19 pandemic may also have played a role, as members sought more services in 2022‒2024, resulting in a surge in utilization greater than what was priced into rates.
Many states put risk corridors in place to stabilize margins from 2020 to 2022, which may have contributed to the tight band of outcomes around the high underwriting gains in that period. However, many states have been removing them for 2024, 2025, and 2026. Without these protections, plans may face greater exposure to underpayment in 2025 and 2026 if cost trends continue to outpace rate assumptions.
What to Watch
Rate setting conversations between states and plans for 2026 are happening now, and in many cases they are quite challenging. In addition to meeting actuarial soundness requirements, states also must balance their budgets, and some may be facing limitations on their traditionally used tools.
Looking ahead, it will be increasingly important that states and plans partner to find cost savings that can ensure the program’s long-term sustainability.
A subscription to HMAIS provides access to comprehensive financial intelligence on Medicaid managed care. Far beyond surface-level snapshots, HMAIS delivers health plan-level financial performance metrics, enrollment trends, and state policy developments that directly shape rate setting and operational strategy. Whether you’re a state official, health plan executive, or policy strategist, HMAIS provides the financial clarity and policy context needed to anticipate regulatory shifts, benchmark performance, and make confident, data-driven decisions.
For questions about the analysis discussed in this article, contact our experts below.
The Trump Administration’s new Health Tech Ecosystem initiative is reshaping how patients and providers access health data, with the bold Kill the Clipboard road map offering a federal blueprint for modernization. At its National Conference being held October 14–16 in New Orleans, Health Management Associates (HMA) is bringing together healthcare leaders to explore how federal policy and industry innovation are driving smarter, more connected care.
About the Sessions
Driving Digital Health Forward: Federal and Industry Enablers of Smarter, Connected Care
The Digital Health “State of the Art”: Success Stories, Trends and Opportunities
Seizing Disruption to Make a Lasting Impact in Healthcare
These and other sessions reflect the federal government’s evolving priorities around digital transformation, interoperability, and patient empowerment. The Health Tech Ecosystem initiative and CMS’s Interoperability Framework are setting new expectations for how healthcare organizations manage data, engage patients, and collaborate across sectors
Featured Digital Healthcare and Innovation Leaders Speaking at the HMA Conference
Our speakers will unpack the far-reaching impact of these advancements, spotlighting opportunities for smarter data exchange and care coordination in a connected ecosystem. In addition, experts from across the healthcare industry will share practical strategies for advancing digital maturity and overcoming operational challenges, with a focus on improving patient care and organizational efficiency.
Chris Walker, Associate Vice President of Enterprise Transformation-Interoperability, Humana
Healthcare organizations need to prepare for a future regulatory environment that is significantly more digital, interoperable, and chronic disease–focused. From health plan executives and state Medicaid directors and policy teams, to provider organizations and health IT and digital health innovators, our speakers will discuss what changes are coming in the digital health space and how you can get your organization ready. Register for the conference today with the code HOTTOPIC25 to receive 20% off the standard conference rate through August.
This week, our In Focus section covers the 2025 CMS Quality Conference. The event convened healthcare leaders, clinicians, researchers, and patient advocates to explore strategies for improving outcomes and modernizing service delivery. Centers for Medicare & Medicaid Services (CMS) Administrator Dr. Mehmet Oz and senior CMS officials emphasized the agency’s evolving priorities under the Trump Administration, with a strong focus on digital transformation, patient empowerment, and fraud prevention.
In this article, Health Management Associates (HMA) experts highlight key themes from the conference. We note where these themes align with the agency’s recent proposed rules and requests for information (RFIs), including several RFIs included in the 2026 Medicare Physician Fee Schedule (PFS) proposed rule, with comments due September 12, 2025. Finally, they advise healthcare organizations of the immediate need to evaluate their risks and opportunities in this digital health ecosystem.
Key Themes of the Conference
Empower Patients with Data
CMS leaders shared a vision for enabling Medicare beneficiaries to experience healthcare technology in the same way that they use in banking and streaming services. Within a year, CMS committed to enabling real-time digital communication with beneficiaries, becoming the nation’s “best payer.” Notably, a patient safety advocate challenged CMS to think about bi-directional data exchange where patients should be able to share data with CMS.
Subsequent to the conference, Administration officials announced elements of the Health Technology Ecosystem infrastructure, including conversational AI tools, diabetes and obesity management platforms, and efforts to “kill the clipboard” by simplifying data access for patients and providers.
Reducing Waste and Tackling Fraud
The conference coincided with the federal government’s multi-billion dollar healthcare fraud takedown, underscoring CMS’ commitment to curbing waste. CMS officials highlighted several aspects of CMS’ work, including application of predictive algorithms dubbed “the Netflix model” to identify suspicious billing patterns. They also talked about the new CMS Innovation Center model—the Wasteful and Inappropriate Service Reduction (WISeR) Model—to engage technology companies to improve prior authorization processes in traditional Medicare, particularly for high-risk items like skin and tissue substitutes.
Focusing on Prevention
CMS tied the Make American Healthy Again (MAHA) agenda to quality measurement reform. CMS officials encouraged moving to two distinct sets of quality measures: one for treating illness and another for maintaining health. These measures could focus on preventing or delaying onset of disease and on measuring outcomes.
Moving to Digital Quality
CMS also emphasized its commitments to digital quality measurement and interoperability through the adoption of Fast Healthcare Interoperability Resources (FHIR®) application programming interface (API) technology. For example, CMS’ Center for Clinical Quality and Standards is testing a FHIR-based assessment tool for inpatient psychiatric hospitals. Separately, the Centers for Disease Control and Prevention (CDC) is transitioning National Healthcare Safety Network’s measures to FHIR.
Policy Connections: From Conference Themes to Federal Action
The conference themes reflect and preview broader federal policy changes including:
The 2026 Medicare Physician Fee Schedule (PFS) proposed rule includes multiple requests for input on streamlining quality measures, enhancing chronic disease management, and expanding digital infrastructure.
On July 30, CMS announced an updated voluntary blueprint for modern health data exchange, which encourages healthcare organizations to become CMS-aligned networks. The agency’s Interoperability Framework describes the voluntary criteria for CMS-aligned in areas of Patient Access & Empowerment, Provider Access & Delegation, Data Availability & Standards Compliance, Network Connectivity & Transparency, and Identity, Security & Trust.
The Road Ahead for Healthcare Organizations
Healthcare organizations need to prepare for a future regulatory environment that is significantly more digital, interoperable, and chronic disease–focused. CMS is building the highway that will enable healthcare organizations to build and maintain the technology necessary for these new initiatives.
This will require state and local government, healthcare organizations, and other partners to retool their infrastructure and workflows to optimize needed operational transformations. All entities should have a strategic roadmap for obtaining and using interoperable clinical data for care management, population health and quality, among other use cases.
Payers will benefit from initiatives such as:
Exploring strategic partnerships to help accelerate technology advancement, such as digital identity providers and specialists in digital quality measurement
Exploring ways to increase focus on prevention, such as increasing uptake of the Medicare Annual Wellness Visit or considering new payment approaches for services like medically tailored meals
Staying current on AI tools and predictive analytics that identify individuals at risk for preventable conditions and working with their provider networks to intervene early
States can take steps to prepare, including:
Exploring strategic partnerships to help accelerate technology advancement, such as digital identity providers and specialists in digital quality measurement
Assessing the reach and impact of existing primary prevention programs to understand how they can use their levers to incentivize healthy lifestyles, encourage culturally responsive health education, and address root causes of preventable illness and disease
Identifying opportunities for aligned efforts and referral pathways, including with community organizations, to address upstream health factors
Health systems and providers will need to reimagine the care experience by:
Exploring early adoption of AI tools for medical documentation to improve both patient experience of care interactions and coding accuracy to support digital quality measurement
Developing age-tailored checklists to ensure face-to-face time with patients to identify and support top primary prevention goals
Evaluating and working with their patients to use digital tools that support chronic disease prevention, such as diabetes and obesity management platforms
Connect with Us
The CMS Quality Conference signaled a substantial shift toward streamlined regulatory approaches and expanded standard data exchange, digital quality reporting and measurement, and AI deployment in care settings and by payers. Stakeholders should anticipate additional federal guidance updates, including in the Medicare Physician Fee Schedule final rule in the fall.
HMA works with state agencies, payers, health systems, and providers to assess and implement digital health, quality systems, and information technology. We can help stakeholders develop cross-sector alliances, and organizations plan for and implement changes needed to react to these new initiatives. To discuss the implications of the Administration’s efforts in prevention, healthcare quality, and interoperability, contact our featured experts below.