HMA Insights: Your source for healthcare news, ideas and analysis.
HMA Insights—including briefs, webinars, and our podcast—gives you easy access to HMA’s deep expertise, helping you stay current on the latest healthcare trends and topics. Search for a topic of interest or browse the latest insights below.
This webinar explored the current state of maternal health in the U.S., with a focus on persistent disparities, recent policy and funding shifts, and the practical realities facing programs on the ground. Kimberly Seals highlighted how external support, and strategic partnerships can help organizations navigate constraints, sharpen their approach, and strengthen impact in a rapidly changing environment.
Learning Objectives:
Understand key policy and funding shifts impacting maternal health.
Learn strategies to align mission and operations during resource constraints.
Explore the value of external partners in advancing maternal health goals.
Gain practical tools to sustain and strengthen maternal health programs.
As states and stakeholders seek greater transparency and accountability in Medicaid, a new analysis from Health Management Associates (HMA), offers a fresh perspective on how dollars flow through the system. Drawing on publicly available data from the Transformed Medicaid Statistical Information System (T-MSIS), HMA disaggregated funding dispersed to Medicaid managed care organizations to discern spending for specific categorically eligible populations. The findings significantly enhance policy discussions and can facilitate development of pragmatic and specific care management interventions that support quality patient care.
For policymakers, regulators, and other stakeholders, this level of disaggregation provides a clearer view of how public dollars are used—and where there may be opportunities to improve performance or reinvest savings. It also supports more informed rate development and contract negotiations, particularly as states pursue value-based purchasing and other reforms. As Medicaid continues to evolve, especially in the context of budget pressures and changes in enrollment and risk profiles of enrollees, understanding the financial picture of managed care programs is essential to ensuring sustainability.
HMA’s team of experts—including actuaries, former Medicaid directors, and data analysts—has deep experience working with T-MSIS data and advising states, plans, and providers on Medicaid program analysis, evaluation, and strategy. For more information about working with T-MSIS data and the insights it can provide, contact our experts below.
As the US Senate debates H.R. 1—a sweeping legislative package that the House passed on May 22, 2025, which would impose nationwide Medicaid work and community engagement requirements by the end of 2026— Health Management Associates’ (HMA’s) latest analysis offers insights into the potential impact of these changes. Drawing on Transformed Medicaid Statistical Information System (T-MSIS) data, HMA experts examine the health and demographic profiles of the approximately 16 million individuals who comprise the Medicaid expansion population.
This 10-slide presentation of findings underscores the high prevalence of chronic and behavioral health conditions among these individuals, raising important questions about how new eligibility requirements could affect access to care and health outcomes. Notably, the presentation contextualizes health needs with Medicaid spending patterns, comparing the Medicaid expansion group with other eligibility categories, such as dual eligibles and children. We explore how the proposals of the nine state 1115 demonstration applications could affect the work requirements policy and implementation landscape. It also breaks down pharmacy spending by therapeutic class, spotlighting common conditions like opioid use disorder.
These insights are especially valuable for Medicaid managed care organizations, providers, and other stakeholders that will play a key role in designing work requirement initiatives and operationalizing any new requirements. Our May 22, 2025, article—Building State Capacities for Medicaid Work and Community Engagement Requirements—delves into the issues that are central to such discussions.
With deep expertise in Medicaid policy, demonstration design, and advanced analytics, HMA is uniquely positioned to help states, plans, and providers navigate the evolving federal landscape. For more information about HMA’s T-MSIS capabilities, contact featured experts below.
On March 4, 2025, the Centers for Medicare & Medicaid Services (CMS) rescinded the 2023 and 2024 guidance on Health-Related Social Needs (HRSN) Section 1115 demonstrations. This policy shift signals a significant pivot in federal Medicaid priorities under the current administration. While states with approved HRSN demonstrations may continue operating under existing terms, the path forward for pending proposals and future renewals is less certain.
This article explores key considerations Health Management Associates (HMA), experts identified for states that need to realign HRSN activities with other activities to align with the Trump Administration’s federal policy objectives and priorities for Section 1115 Medicaid and CHIP demonstrations.
Background on HRSN Initiatives in Section 1115 Demonstrations
In November 2023 and December 2024, CMS published guidance on a new Section 1115 demonstration that gave state Medicaid and CHIP agencies the opportunity to address the broad environmental conditions, or social determinants of health (SDOH), that affect people’s health. This initiative permitted states to address the individual-level adverse social conditions of enrollees that contribute to negative health outcomes. To assist states in their efforts, CMS approved Section 1115 demonstrations that piloted the provision of housing, food, non-medical transportation, and other environmental supports that meet enrollees’ HRSNs.
What does CMS’s rescission of the HRSN demonstration policy initiative mean for states planning their next steps and priorities for Medicaid and CHIP?
First, CMS’s March 4 rescission has no impact on states with a current, active Section 1115 demonstration that includes HRSN. States with HRSN demonstrations can maintain their approved programs until the scheduled expiration date; however, requests to amend any aspect of the program before it expires could subject the state to renegotiation of HRSN components that align with the new federal direction.
Second, states with pending HRSN Section 1115 demonstration proposals should proactively consider new coverage approaches to authorize services that address an individual’s SDOH. Pending proposals developed using the now rescinded guidance may require substantial changes to gain approval. States should also prepare for additional public comment periods if revisions significantly alter the original design.
Looking ahead, CMS is not expected to renew demonstration components that no longer align with current federal objectives. This projection pertains to any demonstration component, not just the rescinded HRSN guidance. States should start planning now for how they will sustain successful HRSN-related outcomes through alternative coverage pathways.
Strategic HRSN Pivot Considerations
While the HRSN guidance has been rescinded, CMS has not withdrawn the 2021 State Health Official Letter RE: Opportunities in Medicaid and CHIP to Address Social Determinants of Health (SDOH) (SHO# 21-001), published during the first Trump Administration. This leaves room for states to pivot HRSN initiatives into other federal authorities, such as:
State Plan Amendments and Waivers. These approaches include state plan options, 1915 waiver options, CHIP Health Services Initiatives, as well as certain special program authorities like Program of All-Inclusive Care for the Elderly or Money Follows the Person.
Childhood Chronic Disease Prevention: States could consider aligning SDOH activities with the Make America Healthy Again initiative of the current administration by focusing on environmental factors that adversely affect an enrollee’s health, such as poor nutrition, chronic stress, overexposure to synthetic chemicals, and mental health challenges.
Justice-Involved Populations: States could explore reentry services and SDOH supports for individuals transitioning from carceral settings to the community, including compliance with new Medicaid requirements for incarcerated youth under the Consolidated Appropriations Act of 2023.
School-Based Health Services. States could explore SDOH activities as part of new approaches to address gaps in the provision of school-based health services to Medicaid and CHIP eligible children. CMS and the US Department of Education launched a joint effort to expand school-based health services by establishing the Medicaid School-Based Services (SBS) Technical Assistance Center to help states increase healthcare access to children enrolled in Medicaid and CHIP. States could explore SDOH initiatives that expand the capacity of school-based entities that provide assistance under Medicaid or CHIP.
Looking Ahead
As states recalibrate their Medicaid and CHIP strategies, understanding how they can align with evolving federal priorities is critical for all stakeholders. Notably, Medicaid stakeholders, including managed care organizations, hospitals and health systems, and providers, also have several opportunities, including:
Inform State Strategy: Plans and providers can share data and outcomes from HRSN interventions to help states assess the value of these services and whether they should continue under alternative authorities.
Shape New Demonstration Designs: As states pivot to align with new federal priorities, plans and providers can offer practical insights into how SDOH interventions could be integrated into behavioral health, reentry, school-based services, and chronic disease prevention efforts.
Strengthen Community Partnerships: Continued collaboration with community-based organizations will be essential to maintain service delivery and demonstrate impact in new policy contexts.
Connect With Us
HMA’s team—including former CMS Section 1115 leaders and other colleagues steeped in Medicaid and CHIP policies and operations—offers unique expertise in designing demonstrations that reflect current federal policy priorities and maximize state outcomes in alignment with program objectives that CMS will support.
For questions about these developments and your organization’s plan to adapt to new federal Medicaid policy priorities, contact our featured experts below. Connect with our experts and other leaders experienced in new pathways for covering effective services at the HMA National Conference, October 14-16, 2025, in New Orleans, LA.
Non-Emergency Medical Transportation (NEMT) is a vital Medicaid benefit designed to ensure that individuals without access to reliable transportation receive critical healthcare services, especially for those with chronic conditions. This session explored the foundational purpose of NEMT and its role in ensuring members access the care they need, improving care outcomes, and advancing health equity by addressing transportation barriers. We examined how services are currently delivered—ranging from traditional ride scheduling to managed transportation brokers—and discussed the growing role of technology and innovation in streamlining operations, enhancing member experience, and curbing fraud, waste, and abuse. Attendees also gained insight into how the NEMT landscape is evolving in response to Medicaid reforms, value-based care initiatives, and the integration of social determinants of health (SDOH).
Learning Objectives:
Understand the role of NEMT in expanding healthcare access
Learn what NEMT is, who it serves, and how it helps reduce access barriers for Medicaid and vulnerable populations
Explore current delivery models and ways to innovate for better results and lower costs
Discuss how technology — such as GPS tracking, app-based scheduling, real-time data sharing, and AI— can improve service delivery and reduce fraud, waste, and abuse
Gain a view into the future trends in the NEMT industry
Understand how policy shifts, integration with social services, and market trends are shaping the future of NEMT
Featured Speakers:
Sufian Chowdhury, Founder and CEO Kinetik
Peter J. Hicks, Executive Director Non-Emergency Medical Transportation Accreditation Commission
Tammy Mihm, Director of Compliance Oversight NEMT TennCare
This 10-slide presentation, Medicaid Expansion: Data-Driven Insights into Healthcare Needs, offers a focused analysis of the Medicaid Expansion population—non-disabled adults ages 19–64 with incomes up to 138% of the Federal Poverty Level—across more than 40 states. Using recent T-MSIS data, the deck highlights the high prevalence of chronic and behavioral health conditions within this group, while also detailing demographic trends among the approximately 16 million enrollees.
Developed by Matt Powers, Shreyas Ramani, Loren Anthes, and Lora Saunders, the presentation contextualizes health needs with Medicaid spending patterns, comparing the Expansion group to other eligibility categories, such as dual eligibles and children. It also breaks down pharmacy spending by therapeutic class, spotlighting common conditions like opioid use disorder. In light of recent federal legislative proposals such as H.R. 1, the deck explores how states are beginning to navigate policy changes through 1115 waiver activity—particularly around medically frail and good cause exemptions—offering early insight into likely implementation strategies.
Watch our Medicaid Town Hall hosted by Health Management Associates. Our experts answered your questions live on a wide range of timely and critical topics, including:
Key policies and insights about the ongoing 2025 federal budget reconciliation negotiations, including changes to Medicaid eligibility policies, financing, and cost-sharing rules.
New executive branch priorities to address program integrity and agency regulations and guidance reshaping provider tax rules and state-directed payment arrangements.
The evolving landscape of Medicaid Section 1115 demonstrations, including updated federal monitoring approaches and new state initiatives.
Medicaid managed care trends, payment innovation, and emerging strategies to address whole-person care focused on maternal health and behavioral health needs.
As Congress intensifies negotiations over budget reconciliation, including potential changes to Medicaid financing and Affordable Care Act (ACA) subsidies, new data from Wakely Consulting Group, an HMA (Health Management Associates) company, sheds light on how the effects of the Medicaid redetermination process continued to unfold well into 2024. Appendix A of the May 2025 white paper Medicaid Redetermination Impacts on the Individual Market, provides a full-year view of enrollment and morbidity trends, showing that the influx of former Medicaid enrollees had some negative effects on risk scores. In fact, relative risk increased across all market types—state-based exchanges (SBEs), in federally facilitated exchange (FFE) Medicaid expansion states, and FFEs in non-expansion states—despite substantial enrollment growth.
Data presented in Wakely’s white paper and their experts’ findings challenge the conventional assumption that higher enrollment dilutes risk and suggest that many new enrollees may have had unmet health needs or delayed care. The data also show that states with the highest enrollment growth did not necessarily experience the greatest morbidity shifts. This decoupling of enrollment and morbidity complicates forecasting for insurers and policymakers alike, especially as Congress debates Medicaid funding and ACA subsidy structures in the ongoing budget reconciliation process.
What to Watch
As federal lawmakers consider reforms that could alter Medicaid eligibility, subsidies, and risk adjustment mechanics, these findings underscore the importance of monitoring not just how many people enroll, but who they are and the type of care they need. The individual market’s evolving risk profile will have direct implications for premium setting, subsidy design, and the financial stability of plans that serve this population.
Connect with Us
Wakely is experienced in all facets of the healthcare industry—from carriers to providers to government agencies. Wakely’s actuarial experts and policy analysts continually monitor and analyze potential changes to inform clients’ strategies and propel their success.
For more questions about the analysis contact our experts below.
In this week’s In Focus section, Health Management Associates Information Services (HMAIS) draws on its database of monthly enrollment in Medicaid managed care programs to provide the latest quarterly analysis of Medicaid managed care enrollment, offering a snapshot of developments across 28 states.[1] The data and insights are particularly timely as stakeholders, including states, Medicaid managed care organizations (MCOs), hospitals and health systems, and providers, continue to plan for multiple possible federal policy changes and the operational realities that will follow.
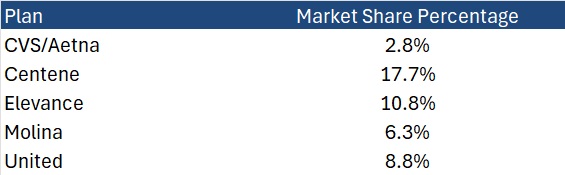
HMAIS also compiles a more detailed quarterly Medicaid managed care enrollment report representing nearly 300 health plans in 41 states. The report provides by plan enrollment plus corporate ownership, program inclusion, and for-profit versus not-for-profit status, with breakout tabs for publicly traded plans. Table 1 shows a sampling of plans and their national market share of Medicaid managed care beneficiaries based on a total of 66 million enrollees. These data should be viewed as a broader representation of enrollment trends rather than as a comprehensive comparison.
Key Insights from Q1 2025 Data
The 28 states included in our review have released monthly Medicaid managed care enrollment data via a public website or in response to a public records request from Health Management Associates (HMA). This report reflects the most recent data posted or obtained. HMA has made the following observations related to the enrollment data:
Year-over-year growth. As of March 2025, across the 28 states reviewed, Medicaid managed care enrollment declined by 2.5 million members year-over-year, a 3.9 percent drop as of March 2025 (see Figure 1). This marks a continuation of the downward trend reported in late 2024, though with notable variation across states.
Figure 1. Year-over-Year Growth in Medicaid Managed Care States, 2020−24, March 2025
Localized growth amid broader declines. While most states experienced enrollment reductions, Indiana and North Carolina bucked the trend with measurable gains, suggesting the influence of state-specific policy shifts or demographic factors. Oregon and Texas also saw modest growth.
Sharpest contractions. Illinois, Maryland, and South Carolina, reported double-digit percentage drops, underscoring the uneven impact of redeterminations and eligibility changes.
Difference among expansion and non-expansion states. Among the 21 states included in our analysis that expanded Medicaid, enrollment fell by 1.8 million (-3.6%) to 48.6 million. In contrast, the seven non-expansion states saw a steeper proportional decline (-5.4%), to a total of 12.2 million enrollees.
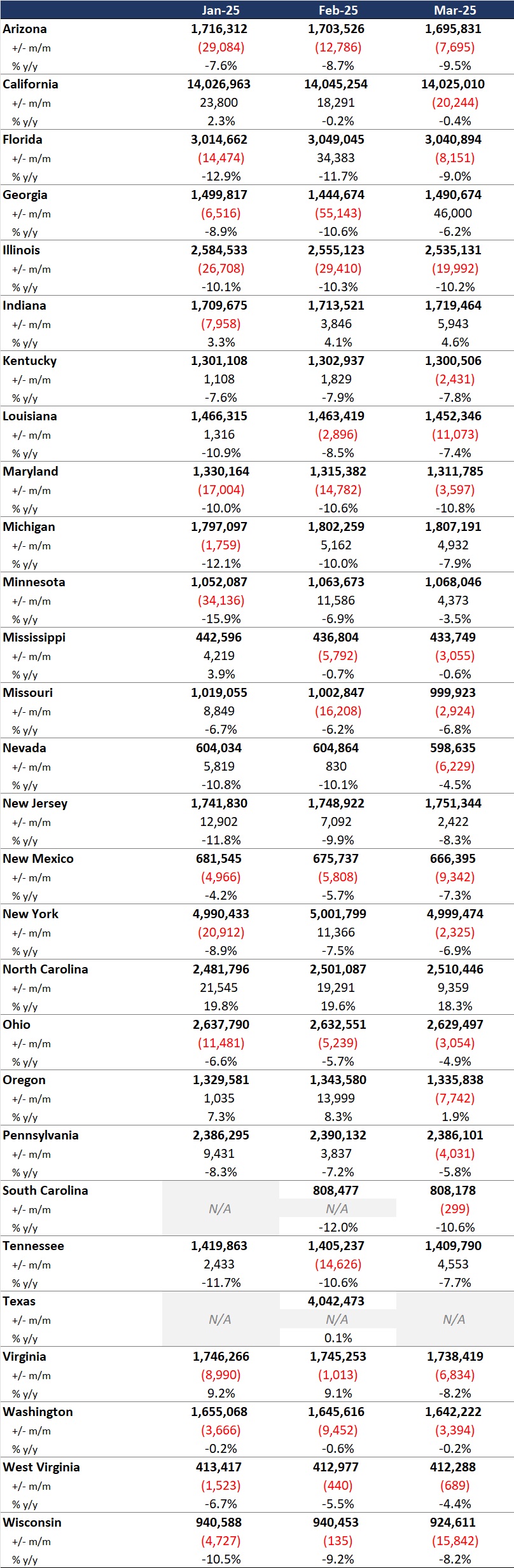
Table 1. Monthly MCO Enrollment by State, January 2025 through March 2025
Note: In Table 1 above and the state tables that follow, “+/- m/m” refers to the enrollment change from the previous month, and “% y/y” refers to the percentage change in enrollment from the same month in the previous year.
It is important to note the limitations of the data presented. First, states report the data at the varying times during the month. Some of these figures reflect beginning of the month totals, whereas others reflect an end of the month snapshot. Second, in some instances, the data are comprehensive in that they cover all state-sponsored health programs that offer managed care options; in other cases, the data reflect only a subset of the broader managed Medicaid population. This limitation complicates comparison of the data described above with figures reported by publicly traded Medicaid MCOs. Hence, the data in Table 1 should be viewed as a sampling of enrollment trends across these states rather than a comprehensive comparison, which cannot be established solely based on publicly available monthly enrollment data.
Market Share and Plan Dynamics
Using our data repository from 300 health plans across 41 states, HMAIS’s report addresses corporate ownership, program participation, and tax status. As of March 2025, Centene continues to lead with 17.7 percent of the national Medicaid managed care market, followed by Elevance (10.8%), United (8.8%), and Molina (6.3%), as Table 2 shows.
Table 2. National Medicaid Managed Care Market Share by Number of Beneficiaries for a Sample of Publicly Traded Plans, March 2025
What to Watch
The policy backdrop remains fluid. The US House of Representatives’ passage of the One Big Beautiful Bill Act introduces sweeping changes to Medicaid financing, including proposed cuts of up to $715 billion. Additional federal proposals, such as mandatory work requirements, could further reshape enrollment patterns.
Stakeholders should prepare for:
Implementation of work/community engagement mandates for certain adult populations
Potential redesign of Affordable Care Act expansion programs
Retraction of federal regulations focused on streamlining of eligibility and redetermination processes to improve accuracy and efficiency
Connect with Us
HMA is home to experts who know the Medicaid managed care landscape at the federal and state levels. As the Medicaid landscape continues to evolve, HMAIS equips stakeholders with timely, actionable intelligence. Our subscription service includes enrollment data, financials, waiver tracking, and a robust library of public documents.
For more information about the HMAIS subscription, contact our experts below.
[1] Arizona, California, Florida, Georgia, Illinois, Indiana, Kentucky, Louisiana, Maryland, Michigan, Minnesota, Mississippi, Missouri, Nevada, New Jersey, New Mexico, New York, North Carolina, Ohio, Oregon, Pennsylvania, South Carolina, Tennessee, Texas, Virginia, Washington, West Virginia, Wisconsin.