
January 8, 2025
CMS Announces 15 States Participating in the Transforming Maternal Health Model
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
CMS Announces 15 States Participating in the Transforming Maternal Health Model

Through a new collaboration with Stanford University’s Emergence Program, HMA’s Strategy & Transformation practice aims to foster innovation in Medicaid and public healthcare. This collaboration seeks to support a new generation of public health innovators, focusing on transformative approaches to healthcare payment, policy, and delivery.

Kyle Murphy and R.J. Briscione presenting.
Kyle Murphy and R.J. Briscione of HMA’s Strategy & Transformation Practice will mentor early-stage companies, deliver guest lectures on the U.S. public healthcare system, and co-develop thought leadership pieces with Stanford faculty and students at Stanford Emergence Program.
This multi-faceted collaboration is designed to provide real-world insights to aspiring healthcare entrepreneurs aiming to improve public health outcomes and equity.
Prof. Narges Baniasadi, who is the founder and executive director of Emergence program says: “We are excited about our growing collaboration with HMA team to catalyze the translation of academic research to impactful innovations for public health and to educate budding entrepreneurs on ways they can scale their impact through working with the public sector.”
Dr. Narges Baniasadi oversees this new initiative that strives to 1) catalyze impact entrepreneurship to address systemic challenges in the health of our society and planet and 2) shift the culture of the innovation ecosystem to be more mission-driven and inclusive. At the core of Emergence is its mission to inspire, educate, and support the next generation of innovators to improve societal and planetary health through impact entrepreneurship.
Early in January, HMA’s Strategy & Transformation Practice will also participate in the Stanford Mussallem Center for Biodesign’s implementation bootcamp for its 2024-25 cohort of Innovation Fellows. Murphy and Briscione will focus on expanding the Innovation Fellows’ understanding of Medicaid and assessing its viability as a go-to-market strategy for innovative solutions. Since 2001, Stanford Biodesign has educated and empowered aspiring and experienced innovators interested in improving healthcare with technology innovation through fellowships, graduate and undergraduate courses, faculty training, and executive education.
To date, the center has trained 219 Innovation Fellows through a 10-month program where they learn to identify and screen important unmet health needs, invent technology-based solutions to address the most promising ones (including medical devices, diagnostics, digital health, drug delivery, and biotechnology solutions), and prepare to implement them into patient care. The Strategy & Transformation Practice brings valuable experience to this collaboration, having previously worked with companies that have emerged from Biodesign trainee projects.
This collaboration elevates HMA’s position within the innovation ecosystem and prepares founders to build and scale products designed for Medicaid populations. By bridging the gap between evidence-based research and practical implementation, this effort has the potential to drive changes in public healthcare policy and delivery, generate the development of cost-effective healthcare solutions, and improve healthcare access for vulnerable populations. As HMA continues to lead in healthcare consulting,supporting the Emergence Program and Stanford Biodesign reinforces its commitment to fostering innovation and improving public health outcomes across the country.

This webinar was held on January 28, 2025.
The information presented in this webinar is based on market knowledge and guidance prior to the new Trump administration; due to the rapidly evolving healthcare and policy landscape, these issues are likely to change moving forward.
Maternal health is at a critical turning point, and healthcare professionals are seeking innovative solutions to improve outcomes, reduce disparities, and ensure equitable access to care. This webinar highlighted the latest CMS policies and guidance designed to address maternal mortality, expand access to high-quality care, and advance health equity for diverse populations. This session is ideal for hospital and critical access administrators, healthcare professionals, and policymakers dedicated to advancing maternal health and achieving better outcomes.
Learning Objectives:
This week, our In Focus section also reviews the significant efforts under way in Ohio to transform how the state provides healthcare services to its Medicare and Medicaid dual-eligible population. Effective January 1, 2026, MyCare Ohio will transition to the Next Generation of its program for people who are dually eligible for both programs.
Overview of Ohio’s Transition to Next Generation MyCare Ohio
This evolution moves Ohio to a fully integrated dual-eligible special needs plan (FIDE-SNP) model that seeks to achieve several key goals through a population-based health approach designed to address inequities and disparities in care for dual-eligible individuals. Examples include:
The MyCare program currently is offered in 29 counties across Ohio but will transition to a statewide program as a part of the Next Generation changes. In addition, coordination only dual-eligible special needs plans (CO-DSNP) will no longer be permitted.
After the Ohio Department of Medicaid (ODM) publicly released the request for applications and evaluated submitted proposals, the agency selected four managed care organizations (MCOs), which will become the Next Generation MyCare plans. The ODM awarded contracts to the following MCOs that will serve MyCare members beginning in January 2026: Anthem Blue Cross and Blue Shield, Buckeye Health Plan, CareSource, and Molina HealthCare of Ohio.
Considerations for the Market
The shift to the FIDE-SNP model and selection of four participating health plans will have a considerable impact on the competitive landscape for Medicare and Medicaid managed care in Ohio. The resulting changes may affect both selected and non-selected participants in different ways, including:
Connect with Us
Ohio is one of many states transitioning to a FIDE model beginning January 2026. Health Management Associates, Inc. (HMA), has successfully supported participating and nonparticipating carriers throughout the transition process and continues to be a dedicated partner to organizations navigating Medicare and Medicaid changes across the country.
Contact our featured experts below, to learn more about the Ohio FIDE-SNP initiative and HMA’s capabilities and expertise to support states, carriers, and other key partners with these transitions.
The Centers for Medicare & Medicaid Services (CMS) announced on December 16, 2024, that it will be terminating the Medicare Advantage Value-Based Insurance Design (VBID) model at the end of 2025 because of the model’s “substantial and unmitigable costs to the Medicare Trust Funds.” This In Focus article delves into the factors driving CMS’s decision and considerations for policymakers, Medicare Advantage Organizations and other interested stakeholders.
VBID Outcomes
VBID, run by the CMS Innovation Center, is not a permanent part of the Medicare Advantage (MA) program. Innovation Center models are required to be modified or terminated if they are a cost to the program.
CMS found that costs for the VBID model totaled $2.3 billion in calendar year (CY) 2021 and $2.2 billion in CY 2022, an unprecedent amount for an Innovation Center model. CMS concluded that these substantial expenses—driven by increased risk score growth and Part D expenditures—were unmitigable through policy modifications. Therefore, consistent with statutory requirements, CMS took action to terminate the model by the end of 2025. Earlier this year, CMS announced it would discontinue the part of VBID that allowed MA plans to offer hospice services.
Next year, the VBID model will have 62 participating MA plans and is projected to offer 7 million Medicare beneficiaries additional benefits and/or rewards, including those designed to address social determinants of health and reduce cost-sharing for prescription drugs used to treat and manage chronic conditions. As part of the announcement, CMS pledged to support a stable transition for all enrollees in MA plans participating in the MA-VBID model and emphasized that key benefits available under the model will continue to be widely available, including supplemental benefits that address the whole-person healthcare needs of beneficiaries. In addition, CMS noted beneficiary cost-sharing for prescription drugs will be reduced as the result of the expansion of the low-income subsidy program under the Inflation Reduction Act and the CMS Innovation Center’s Medicare $2 Drug List Model, which is slated to begin in 2027.
As part of the announcement, CMS released an executive summary of a forthcoming evaluation report, with the full report expected to be released in early 2025.
Key Considerations
Since the MA-VBID model’s launch in 2017, the program has experienced significant growth through a series of legislative and model changes, including requirements in the Bipartisan Budget Act of 2018 that expanded eligibility to MA plans in all 50 states and allowing all types of MA special needs plans to participate in MA-VBID. Previous CMS evaluations found that the MA-VBID model led to improvements in the quality of care for beneficiaries and promoted greater adherence to prescription drugs used to treat and manage chronic conditions. Though CMS has concluded that excess costs require the termination of MA-VBID by the end of 2025, the incoming Trump Administration can be expected to closely examine this decision and look at the entire Innovation Center portfolio.
Connect with Us
Health Management Associates, Inc. (HMA), Medicare experts will continue to assess and analyze the response to CMS’s announcement, including the incoming administration’s views on the decision and potential alternatives. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist MA organizations and interested stakeholders in analyzing and adapting to the marketplace as the MA-VBID program ends.
For further analysis of the MA-VBID decision and its impact on the market, contact our experts below.
This week, our In Focus section reviews the year-end legislative package congressional leaders announced as part of the stopgap funding to prevent a government shutdown. The package, which was unveiled December 18, 2024, would extend expiring Medicaid and Medicare policies, reauthorize health and human services programs, and extend federal funding for discretionary programs through March 14, 2025. The existing temporary funding measure expires December 20, 2024.
Following is a summary of several major healthcare policies that, if approved, will inform the shifting federal policy landscape and state and local programs in 2025.
Pharmacy Benefit Managers
The healthcare package includes policies that reflect several years of increased scrutiny on pharmacy benefit managers (PBMs), including:
Medicaid Policies and Programs
The legislative text includes 13 separate sections that address Medicaid policies, including extensions on expiring policies, establishment of new programs, and plans to codify certain other policies related to Medicaid eligibility and renewals. These policy changes include:
Medicare Payments
The compromise package also increases the Medicare Physician Fee Schedule conversion factor by 2.5 percent in 2025 to partially offset a 2.83 percent cut that the Centers for Medicare & Medicaid Services (CMS) finalized in November. Providers consider this a short-term fix, however, and Congress, provider advocates, and other interested parties are engaged in discussions about making broader changes to Medicare physician pay in 2025.
Notably, the agreement includes a payment policy consistent with a bill that the House of Representatives passed earlier this year—the Lower Cost More Transparency Act—to provide enhanced information about payment differentials between off‐campus outpatient departments and other outpatient facilities. The provision requires each off-campus outpatient department to obtain and bill for services under a unique national provider identifier.
Other notable Medicare policies include:
Other Notable Provisions
What’s Next
Funding for the federal government expires December 20, 2024. Congress will need to approve another temporary measure to avert a government shutdown. The length and scope of such an extension remains under discussion, though the current continuing resolution would push the funding deadline into the first few months of the incoming Trump Administration and new Congress. Healthcare stakeholders, including payers, state and local governments, providers, and community organizations, should continue to monitor the congressional negotiations and be prepared to analyze the impact of legislation that Congress ultimately approves.
Connect with Us
Health Management Associates, Inc. (HMA) experts will continue analyzing the implications of the funding and policy updates in the December 18 package and ongoing congressional discussions to reach an agreement. HMA’s experts have the depth of knowledge, experience, and subject matter expertise to assist organizations with navigating these changes and the impact for health and health adjacent sectors. Please contact Laura Pence and Andrea Maresca to connect with our experts.
Congress Continues Negotiations on 2025 Spending and End-of-Year Package

Tom Cochran, partner at 720 Strategies, is a renowned expert in digital communication and healthcare public relations. Tom reflects on the broader impact of digital tools, acknowledging both their potential to connect us and their unintended consequences, such as cognitive overload and societal fragmentation. The conversation highlights practical strategies for navigating transitions in leadership—whether in politics or healthcare—and emphasizes the importance of understanding, listening, and adapting communication strategies to fit the moment. Tom leaves us with a reminder of the irreplaceable value of face-to-face interaction in an increasingly digital world.
This week’s In Focus section summarizes states’ Medicaid Section 1115 demonstration priorities over the last four years and highlights predicted changes coming with a new presidential administration. In the waning days of any presidency, regardless of party, reviewing and approving pending Section 1115 applications that reflect the current administration’s key policy initiatives is a priority for officials at the Centers for Medicare & Medicaid Services (CMS).
Each administration has discretion over which Section 1115 demonstrations to encourage and approve. Though specific Medicaid priorities under the upcoming Trump Administration are still nascent, Health Management Associates, Inc. (HMA), federal, and state experts are monitoring these developments. This article describes a subset of the signature initiatives the Biden Administration permitted states to pursue in their Medicaid Section 1115 demonstrations and how the new administration could focus on different priorities, rescind existing guidance, or potentially withdraw already approved waivers.
Overview of Biden-Era Section 1115 Demonstration Initiatives
CMS-approved Section 1115 demonstrations permit alternative methods to improve the accessibility, coverage, financing, and delivery of healthcare services under joint federal-state funded programs, specifically Medicaid and the Children’s Health Insurance Program (CHIP).
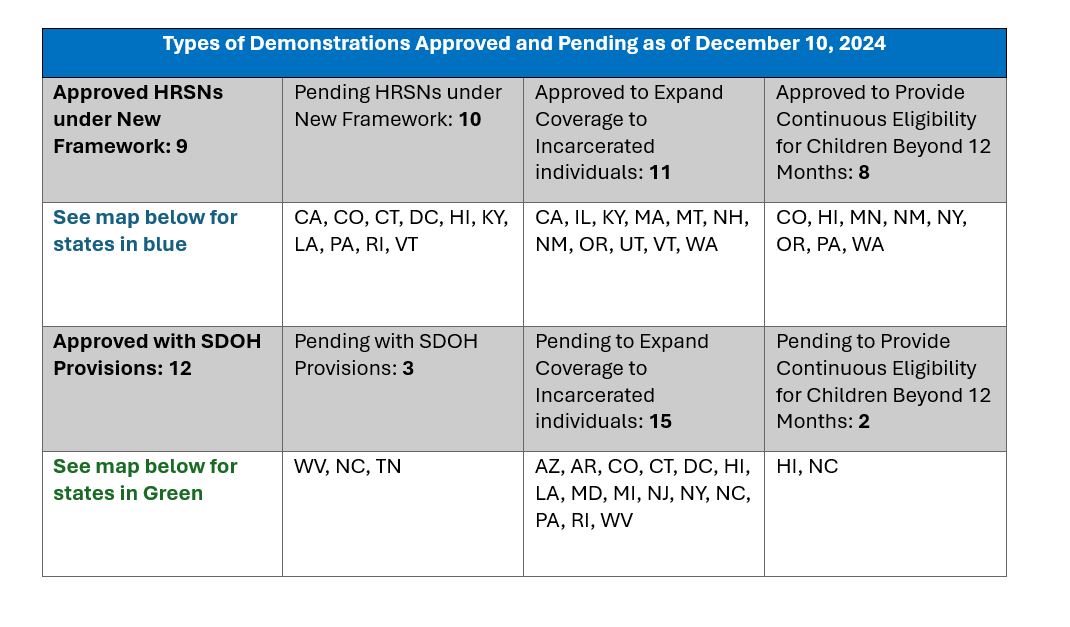
Addressing health disparities and promoting integrated care in Medicaid became a primary focus of the Biden Administration. In November 2023, CMS introduced a Medicaid and CHIP Health-Related Social Needs (HRSN) Framework, giving state Medicaid agencies the opportunity to address the broader social determinants of health (SDOH) that affect their enrollees, leading to better health outcomes. The new initiatives were not intended to replace other federal, state, and local social service programs, but rather to coordinate with those efforts. HRSN demonstration approvals to date include coverage of rent/temporary housing and utilities for up to six months and nutrition support (up to three meals per day), departing from longstanding prohibitions on payment of room and board in Medicaid.
During the present administration, CMS also has provided novel opportunities for states to adopt strategies that promote continuity of Medicaid coverage, mainly through bolstering Section 1115 demonstrations to provide multiyear continuous eligibility for children. In addition, CMS released guidance in April 2023 so states could apply for a new Section 1115 demonstration opportunity to test transition-related strategies that support community reentry for incarcerated people who would otherwise be eligible for Medicaid or CHIP.
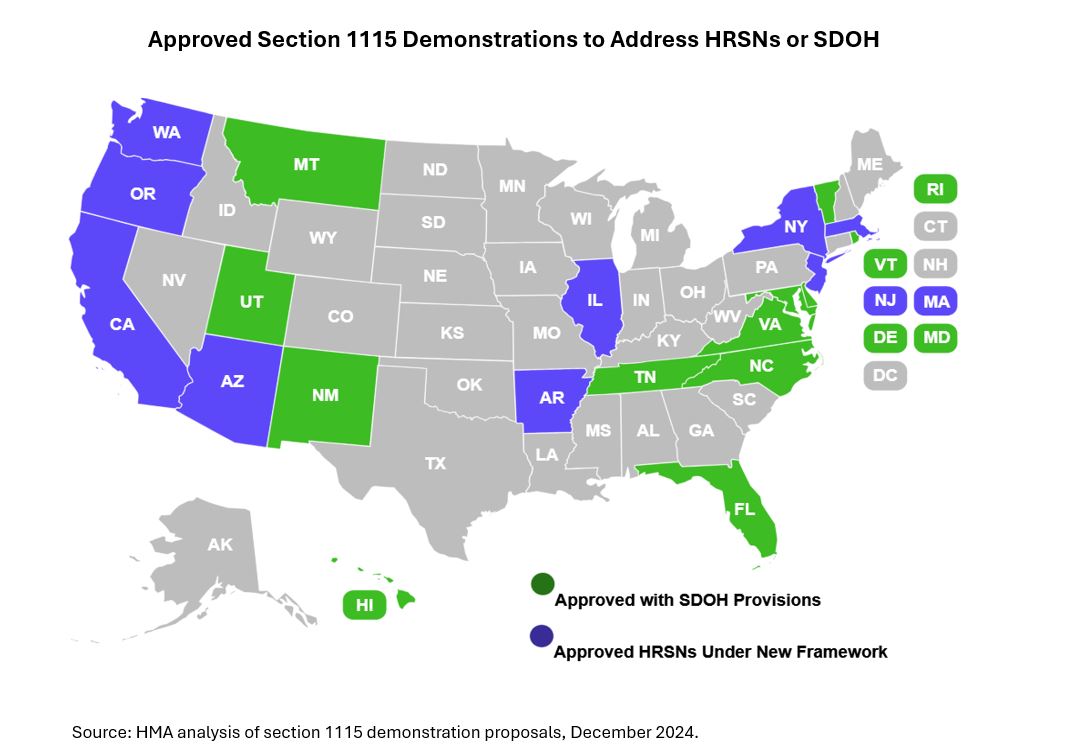
The table and map below show the types of demonstrations approved and pending to date. We anticipate that incoming administration officials will closely examine the four demonstration initiatives outlined as they determine their own Medicaid policy agenda and priorities. Under President Biden’s Administration, nine states received federal approval for HRSN demonstrations under the new framework. Another 10 states have applications pending.
Rescissions and renewals. Incoming Trump Administration officials technically could attempt to rescind some of the Section 1115 demonstrations approved during the Biden Administration. The Biden Administration unsuccessfully pursued with, a similar strategy for certain 1115 demonstration components approved during President-Elect Trump’s first term. Like the Biden Administration, the incoming Trump officials may choose not to renew demonstrations, even if the courts prevent them from rescinding approvals.
Any signature Section 1115 policy is unlikely to emerge until the new administration’s policy officials are in place. There are, however, important insights to consider based on the first Trump Administration’s priorities and areas of common ground across the Biden and first Trump administrations.
Signature 1115 initiatives. During President Trump’s first term, one signature Medicaid Section 1115 initiative allowed states to apply work requirements to some eligibility groups. CMS officials at that time also approved capped allotments for certain components of a state’s Medicaid program. Some states might consider revisiting these options with incoming administration officials. Two other key policy areas to watch following the transition include:
Implementation Considerations
Federal approval of Medicaid Section 1115 demonstration proposals is a critical milestone for states. Demonstration implementation also requires significant and ongoing leadership, resources, and collaboration between states and CMS and states and their partners.
The type of state demonstration activity is expected to shift dramatically over the course of the new administration. For example, proposals may shift from expansions in coverage and benefits to reflect the new administration’s other priorities. States, too, may consider alternative approaches to Section 1115 demonstrations, such as state plan authorities like in lieu of services (ILOS), to pursue certain innovative approaches that they might otherwise have implemented with demonstration authority.
Connect with Us
HMA empowers states, providers, and other stakeholders to thrive in an ever-changing healthcare landscape. With deep expertise at every level, HMA teams support state Medicaid programs and stakeholder partners nationally to address a range of operational challenges, including designing innovative healthcare approaches to address urgent healthcare challenges, expanding coverage opportunities, and optimizing integration to address program efficiencies and improved “whole person” care.
We have expertise in all of the components critical to developing Section 1115 programs—from the policy knowledge, to actuarial/budgeting talent, to communications and project management skills, as well as the necessary IT infrastructure.
Contact our featured experts below to learn more about HMA’s capabilities and expertise.

In this season of gratitude and joy, we reflect on a year filled with purpose and partnership. At HMA, we’re honored to support our clients and partners working to improve the health of individuals, families, and communities nationwide.
Watch our video to find out what fuels our passion to create a positive impact in all the work we do, from addressing health equity and improving maternal outcomes to advancing healthcare policy and helping organizations deliver the highest quality care.
All of us at HMA are wishing you a joyous holiday season and new year filled with continued success.
The transition of MyCare Ohio to the Next Generation of its program on January 1, 2026, marks a significant evolution in the way Ohio provides healthcare services to its dual-eligible population – those who qualify for both Medicaid and Medicare services. This evolution moves Ohio to a Fully Integrated Dual Eligible Special Needs Plan model (FIDE SNP) that aims to achieve several key goals through a population health approach, designed to address inequities and disparities in care for dual-eligible individuals. These goals include:
The current MyCare program is offered in 29 counties across Ohio but will transition to a statewide program as a part of the Next Generation changes. Additionally, Coordination Only Dual Eligible Special Needs Plans (CO DSNP) will no longer be permitted.
After the Ohio Department of Medicaid (ODM) publicly released the request for applications (RFA) and evaluated submitted proposals, they selected four Managed Care Organization (MCOs) that will become the Next Generation MyCare plans. The ODM awarded the following MCOs to serve MyCare members beginning in January 2026: Anthem Blue Cross and Blue Shield, Buckeye Health Plan, CareSource, and Molina HealthCare of Ohio.
The shift to the FIDE SNP model and selection of four participating health plans will have a considerable impact on the competitive landscape for Medicare and Medicaid managed care in Ohio. The resulting changes can affect both selected and non-selected participants in different ways, including:
Ohio is one of many states transitioning to a FIDE model beginning January 2026. Health Management Associates (HMA) has successfully supported participating and non-participating carriers throughout the transition process and continues to be a dedicated partner to organizations navigating Medicare and Medicaid changes across the country. Contact one of HMA’s many experts for more details on how to navigate this evolution in health care.