
March 20, 2024
State Teams Convene to Strengthen Collaboration across Child Welfare, Behavioral Health, and Medicaid
HMA Insights – including our new podcast – puts the vast depth of HMA’s expertise at your fingertips, helping you stay informed about the latest healthcare trends and topics. Below, you can easily search based on your topic of interest to find useful information from our podcast, blogs, webinars, case studies, reports and more.
State Teams Convene to Strengthen Collaboration across Child Welfare, Behavioral Health, and Medicaid

A new report by Leavitt Partners, an HMA Company, outlines the concept of site-neutral payment reforms being considered as a potential program improvement, and proposes a compromise approach to implementing site-neutral payments that benefits beneficiaries, hospitals, and the Medicare program. Site-neutral payments, which would equalize payment for the same services across all settings of care, are most commonly considered in connection with outpatient or ambulatory settings. Because out-of-pocket costs for Medicare beneficiaries are based on a percentage of the total reimbursement costs, any policy that reduces reimbursement for some services would result in savings to Medicare beneficiaries.
The approach proposed in the report lowers out-of-pocket costs to Medicare beneficiaries, improves the financing of the Medicare program by addressing a payment distortion, and reinvests in hospitals through new targeted funding and inclusion of policy priorities.
If you have any questions, contact our expert below.
This week, our In Focus section covers Congress’s and the Administration’s parallel efforts to finalize fiscal year (FY) 2024 spending bills and begin the budget process for FY 2025.
Congress approved a bipartisan package for some of the FY 2024 spending bills, and on March 9, 2024, President Biden signed the Consolidated Appropriations Act of 2024 into law (PL 118-42). Programs funded through this measure include the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and other federal nutrition supports, rental assistance for safe and affordable housing, and veterans medical care and benefits.
Several mandatory funding extensions of public health programs and health-related policies also found their way into the 2024 consolidated appropriations package, including extending the Community Health Center Fund, delaying reductions in the disproportionate share hospital allotments, defining Certified Community Behavioral Health Centers (CCBHCs) as a Medicaid service, extending incentive payments for certain Medicare providers, and mitigating the impact of cuts to the Medicare physician fee schedule.
These policies, however, addressed a narrower set of issues than the expansive and bipartisan legislation that has been moving through both chambers of Congress. For example, House and Senate members have worked on respective bipartisan policies affecting price transparency, pharmacy benefit managers, and Medicare site-neutral policies, among others.
Meanwhile, President Biden released the FY 2025 Budget proposal March 11, 2024, kicking off the annual budget process. Like the administration’s FY 2024 budget proposal, the FY 2025 plan emphasizes deficit reduction and continues to make equity and Medicare solvency cornerstones of the budget. Health-related priorities include expanding access to affordable healthcare services, lowering drug costs, improving maternal health, addressing the mental health and substance use disorder crises, and enhancing biodefense and preparedness activities.
Check out the FY 2025 budget analysis from Leavitt Partners, a Health Management Associates, Inc. (HMA), company, and a deeper dive into the Consolidated Appropriations Act of 2024.
What We’re Watching
Congress is continuing negotiations on the outstanding spending bills, including the one that funds the Departments of Health and Human Services, Labor, and Education through September 2024. Lawmakers are working to reach an agreement before the next funding deadline of March 22.
The administration’s FY 2025 budget proposals are generally being characterized as a blueprint for President Biden’s re-election campaign and, if successful, a policy agenda for his second term. Though Congress has already begun holding hearings on the budget request, members on both sides of the aisle will likely focus on issues that resonate in an election year.
Regardless of the outcome of the November elections, Congress has an opportunity to address unfinished business during the lame duck session later this year.
HMA and Leavitt Partners collaborate to monitor legislative and regulatory developments in healthcare and adjacent spaces and to assess the impact of policy changes on the healthcare industry.
Federal Policymakers Consider Current and Future Spending Measures on Simultaneous Tracks
This week, our In Focus section analyzes preliminary 2023 Medicaid spending data collected in the annual CMS-64 Medicaid expenditure report. After submitting a Freedom of Information Act request to the Centers for Medicare & Medicaid Services (CMS), HMA received a draft version of the CMS-64 report that is based on preliminary estimates of Medicaid spending by state for federal fiscal year (FFY) 2023. Based on the preliminary estimates, Medicaid expenditures on medical services across all 50 states and six territories in FFY 2023 totaled nearly $852.9 billion, with 59.6 percent of that amount now flowing through Medicaid managed care programs. In addition, total Medicaid spending on administrative services was $33.8 billion, bringing total program expenditures to $886.7 billion.
Total Medicaid managed care spending (including the federal and state share) in FFY 2023 across all 50 states and six territories was $508.1 billion, up from $468.3 billion in FFY 2022. This figure includes spending on comprehensive risk-based managed care programs as well as prepaid inpatient health plans (PIHPs) and prepaid ambulatory health plans (PAHPs). PIHPs and PAHPs refer to prepaid health plans that provide only certain services, such as dental or behavioral health care. Fee-based programs such as primary care case management (PCCM) models are not included in this total. Following are some key observations.
Table 1. Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures, FFY 2007−2023 ($M)

As the table below indicates, 68.9 percent of FFY 2023 spending came from federal sources, which is 11.5 percentage points higher than the pre-Medicaid expansion share in FFY 2013 and 1.3 percentage points higher than FFY 2020.
Table 2. Federal versus State Share of Medicaid Expenditures, FFY 2013−2023 ($M)

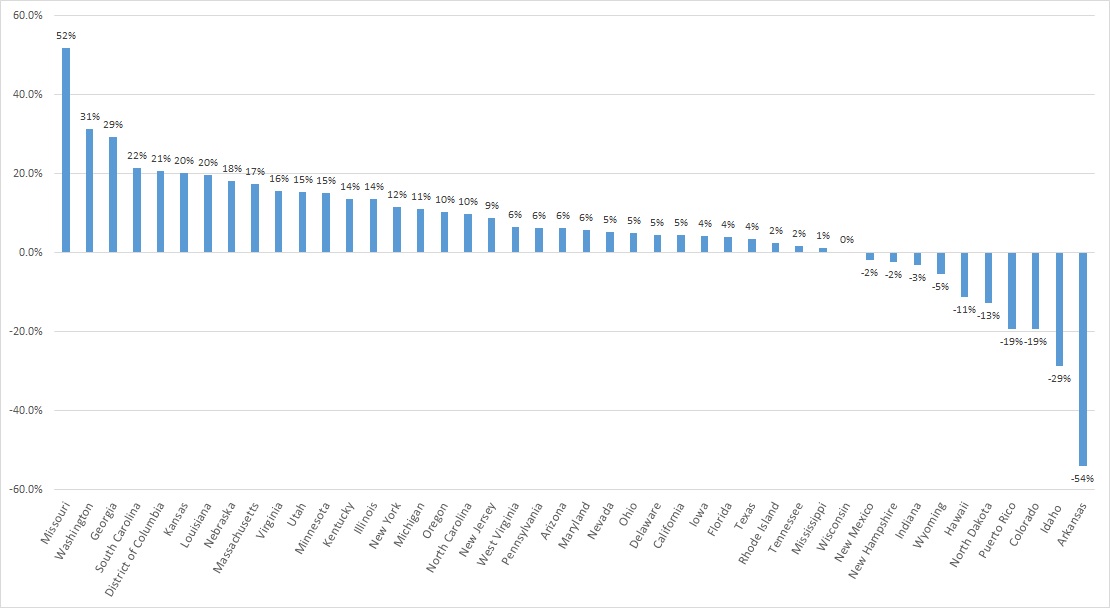
A total of 44 states and territories report managed care organization (MCO) spending in the CMS-64 report. Average MCO spending during FFY 2023 increased 8.5 percent. On a percentage basis, Missouri experienced the highest year-over-year growth in Medicaid managed care spending at 51.7 percent, followed by Washington at 31.4 percent and Georgia at 29.3 percent.
The chart below provides additional detail on Medicaid managed care spending growth in states with risk-based managed care programs in FFY 2023.
Figure 1. Medicaid Managed Care Spending Growth on a Percentage Basis by State, FFY 2022-2023
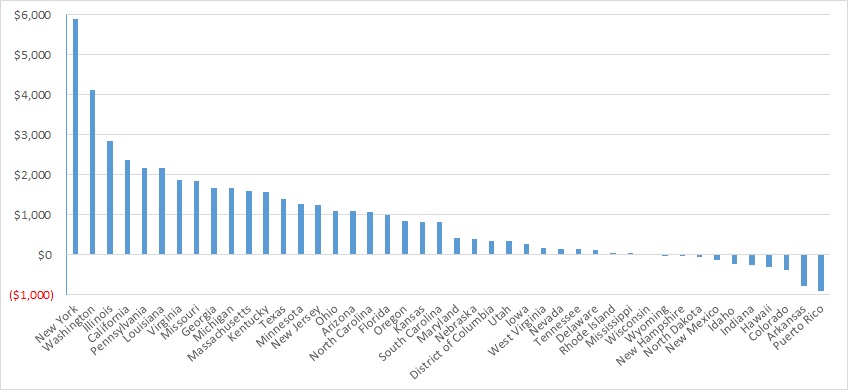
Looking at year-over-year spending growth in terms of dollars, New York experienced the largest increase in Medicaid managed care spending at $5.9 billion. Other states with significant year-over-year spending increases included Washington ($4.1 billion), Illinois ($2.8 billion), and California ($2.4 billion). The chart below illustrates the year-over-year change in spending across the states.
Figure 2. Medicaid Managed Care Spending Growth on a Dollar Basis by State, FFY 2022−2023 ($M)
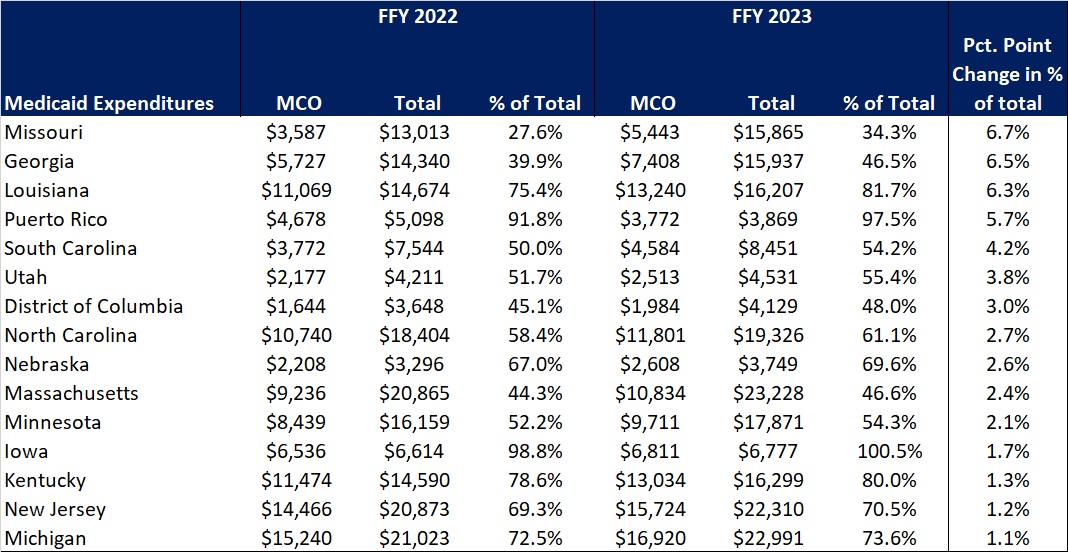
The percentage of Medicaid expenditures directed through risk-based Medicaid MCOs increased by more than one percentage point in 15 states from FFY 2022 to FFY 2023. The managed care spending penetration rate rose 6.7 percentage points in Missouri, 6.5 percentage points in Georgia, 6.3 percentage points in Louisiana, and 5.7 percentage points in Puerto Rico. In all, 22 states saw a decrease in managed care penetration from FFY 2022 to FFY 2023.
Table 3. Medicaid MCO Expenditures as a Percentage of Total Medicaid Expenditures in States with a One percent or Greater Increase from FFY 2022 to FFY 2023 ($M)
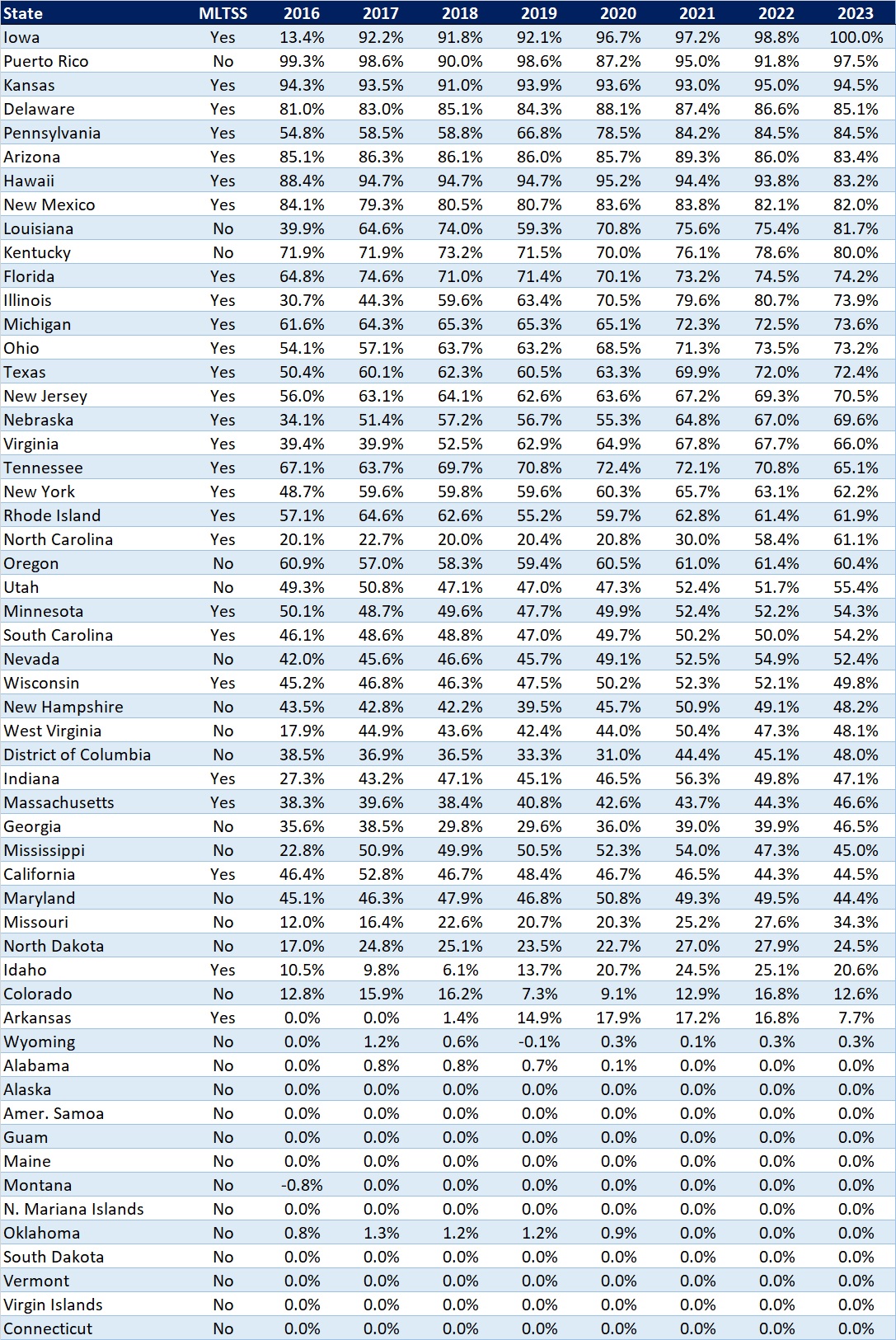
The table below ranks the states and territories by the percentage of total Medicaid spending through Medicaid MCOs. Iowa reported the highest percentage at 100 percent, followed by Puerto Rico at 97.5 percent and Kansas at 94.5 percent.
In many states, certain payment mechanisms may never be directed through managed care, such as supplemental funding sources for institutional providers and spending on retroactively eligible beneficiaries. As a result, the maximum achievable penetration rate in each state will vary and may be below the amount achieved in other states. The Medicaid managed care spending penetration rate is greatly influenced by the degree to which states have implemented managed long-term services and supports (MLTSS) programs.
Table 4. Medicaid MCO Expenditures as a Percent of Total Medicaid Expenditures, FFY 2016-2023
If you’re interested in becoming an HMAIS subscriber and for access to the CMS-64 data, contact our expert below.


Reviewing existing policies and procedures to identify gaps and needed updates to ensure compliance with regulations and adherence to best practices and industry standards.
Recommending revisions based on the assessment review and helping prioritize changes based on risk analysis.
Updating policies and procedures based on the approved recommendations.
Developing a training program for staff regarding the updated privacy and security policies and procedures via in person training, virtual training, and/or creating training videos.
HMA’s privacy and security assessment and support services capabilities include the following qualifications and expertise:
Holding leadership roles at state health data organizations and on the National Association of Health Data Organizations Board
Coordinating health information technology (HIT) for state Medicaid agencies
Leading state value-based purchasing agencies
Founding HIT strategic consulting firms
Experience with the National Association of County and City Health Officials
Project management and strategic planning support for multiple state agencies and data organizations
Privacy and security legal expertise
Contact our experts:


On February 15, 2024, HMA Principals Teresa Garate, PhD and Anika Alvanzo, MD, MS presented at the 2024 Opioid & Fentanyl Abuse Management Forum sponsored by the World Conference Forum. Their presentation focused on enhancing outreach strategies for reaching and engaging people suffering from opioid use disorder in their communities. Participants were able to learn about public health approaches, harm reduction and low-barrier treatment, as well as an understanding of the considerations needed when building community driven strategies that are person-centered.
Dr. Garate also served as chairperson for the two-day event, providing opening remarks on the first day, engaged panelists in provocative conversations, and closed out the gathering with a summary of the presentations. With a deep understanding that addiction is a disease of the brain, the presentations focused on biopsychosocial approaches and highlighted the use of multiple and diverse interventions. The compilation of the event’s presentations resulted in robust discussions on research, model programs, model strategies, and the critical role of policy, funding, innovation, and data sharing. The overarching message was that as a collective group of advocates, we must continue to use every resource we have at our disposal to push the envelope and challenge the status quo so that we can stop the increase in overdoses and overdose deaths.
At HMA, consultants on our opioid team have unique expertise and more than 30 years of experience tackling every part of the substance use disorder system. They have led the development of comprehensive prevention, evidence-based treatment, and recovery solutions at the state, county and community level. We have experience working with states and community organizations to develop impactful, sustainable responses to opioid crisis issues. Our team is ready to help clients create actionable and sustainable programs to address the opioid epidemic and addiction treatment.
Contact us to learn more about how we can help your organization develop programs to help combat the opioid crisis.
Driving Change in Healthcare Delivery: HMA Spring Workshop Builds Towards Policy and Strategy Frameworks Necessary to Implement Value-based Care
As Medicare, state Medicaid agencies, Medicare Advantage plans, Medicaid managed care organizations, and commercial insurers increasingly adopt alternative payment models (APMs), Health Management Associates (HMA) provides a range of innovative and successful approaches to value-based care (VBC).
Our subject matter experts can help you succeed with
value-based payments (VBP).
Offer insights for transforming the care delivery model to efficiently deliver optimal patient and population-level health outcomes while successfully managing total cost of care
Ensure quality is the primary goal of VBP program design and implementation
Develop payment models that align the incentives of payers and providers
Integrate physical and behavioral healthcare, and close gaps related to social determinants of health and health equity
Help clients successfully transition from fee-for-service to value-based payments by providing expertise in change management, analytics, network engagement, and IT infrastructure
Improve the patient and provider experience
Qualify, manage, and monitor health insurance risk
Prepare for and succeed in accreditation for VBP capabilities
ORGANIZATIONS WE SUPPORT
Those engaged in VBP or interested in engaging in VBP
Payers
Providers
Purchasers
Those interested in advancing the broader movement to value
Federal, State & Local Governments
Associations
Foundations
Investment Firms
HMA Can Support You Through All Phases of Value-Based Care
From contract to care plan, we have the experience and guidance tools to support your organization’s move to value-based care and risk-based contracting.
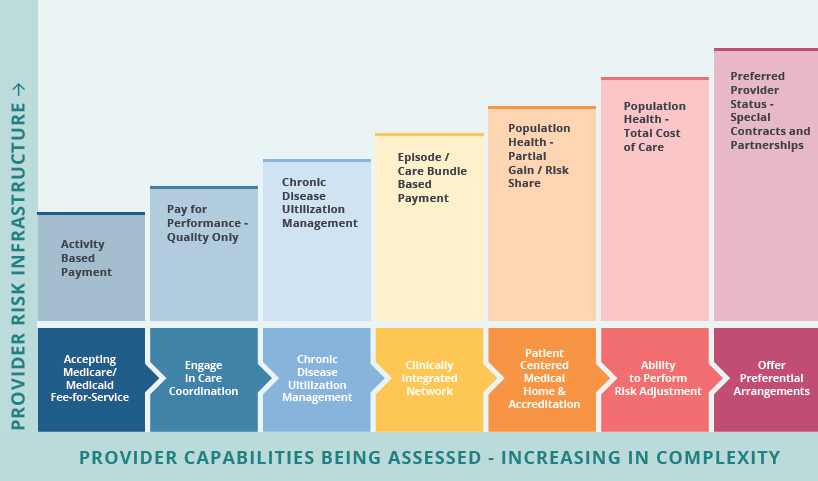
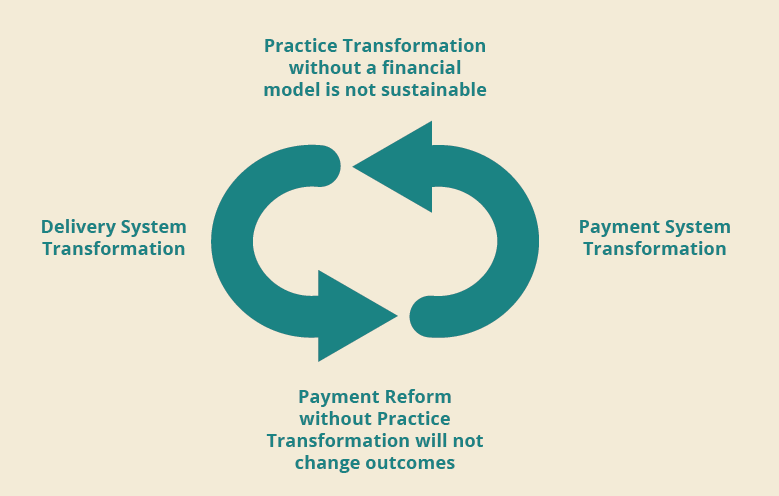
Our philosophy involves applying a health equity model to close social determinant gaps and health disparities. Value-based healthcare is all about the care delivery model. Under value-based care agreements, providers are rewarded for helping patients improve their health, reduce the effects of emerging/rising risks and incidence of chronic disease, and live healthier lives in an evidence-based way.
Our collaborative approach will be tailored and customized to your needs to help you successfully implement VBP.
Determine readiness across key building blocks for moving to value-based payments and achieving continuous improvement across healthcare organizations.
Implementation that includes benchmarks and measurements of success. We facilitate stakeholder input to capture and analyze data from these interactions through surveys, focus groups, and interviews.
Aligning incentives with providers is key to successful value-based care strategies. Understanding methods for identifying and closing gaps in care pathways for common chronic conditions or addressing rising/emergent risks as well as how to create buy-in among providers and other members of the care team.
Including actuarial expertise required for contracting in key areas such as financial projections, reserves, total cost of care analysis, and benchmarking. We provide an assessment of third-party software to support APMs.
Including methods for incorporating whole-person care into clinical algorithms that apply to every interaction with the patient and their families. Integrating behavioral health with physical health and addressing social determinants of health/health-related social needs into VBC programs.
Assist with identifying key performance indicators (KPIs) and quality measurement incentives
for pay-for-performance or pay-for- value to support population health outcomes and support total cost of care in various VBP arrangements.
Provide support and consultation on scope of requirements to ensure VBC contract meets delegation requirements for operational, state, CMS regulatory and accreditation requirements.
Providers including hospitals, academic medical centers, physician practices, community health centers, rural health centers, and federally qualified health centers
Medicaid, Medicare, Marketplace and Commercial MCOs
State and federal agencies
Contact our experts:

HMA is pleased to welcome new experts to our family of companies in November 2023.
Kenneth Cochran is a healthcare executive with more than 20 years leveraging his clinical, business and academic background to deliver strategic planning, operational excellence, top-line revenue growth, positive physician relations and organizational alignment.
Matt Smith, ASA, has experience with population health analytics, total cost of care analysis, value-based care contracts, financial modeling, pricing and reserving, and risk adjustment. Read more about Matt.
Jimmy Mans, FSA, MAAA, has extensive experience working with health plans, providers, state and federal governments, and pharmaceutical manufacturers. Read more about Jimmy.
